

The Outcome Relevance of Pre-ECMO Liver Impairment in Adults with Acute Respiratory Distress Syndrome

Abstract
:1. Introduction
- A significant liver impairment before ECMO initiation (pre-ECMO), indicated by the presence of acute liver injury or a higher MELD score, is associated with increased mortality;
- The requirement of V-VA ECMO support due to an acute cor pulmonale or cate-cholamine refractory shock is associated with (a) a higher prevalence of pre-ECMO acute liver injury and (b) a higher pre-ECMO MELD score and, therefore, (c) an increased mortality.
2. Materials and Methods
2.1. Data Acquisition, Inclusion, and Exclusion Criteria
2.2. ECMO Management
2.3. Definitions and Scores Calculation
2.4. Statistical Analysis
3. Results
3.1. Patient’s Demographics and Characteristics
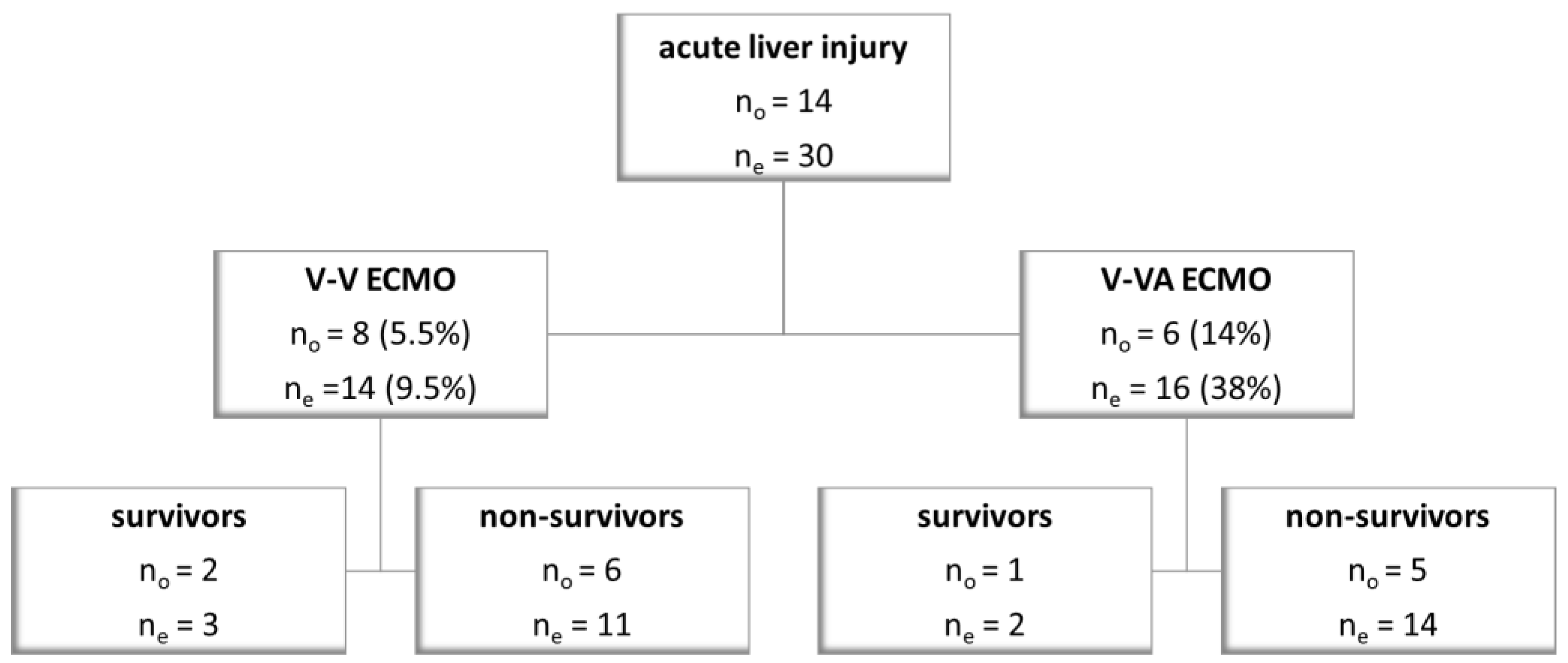
3.2. The Development of Acute Liver Injury
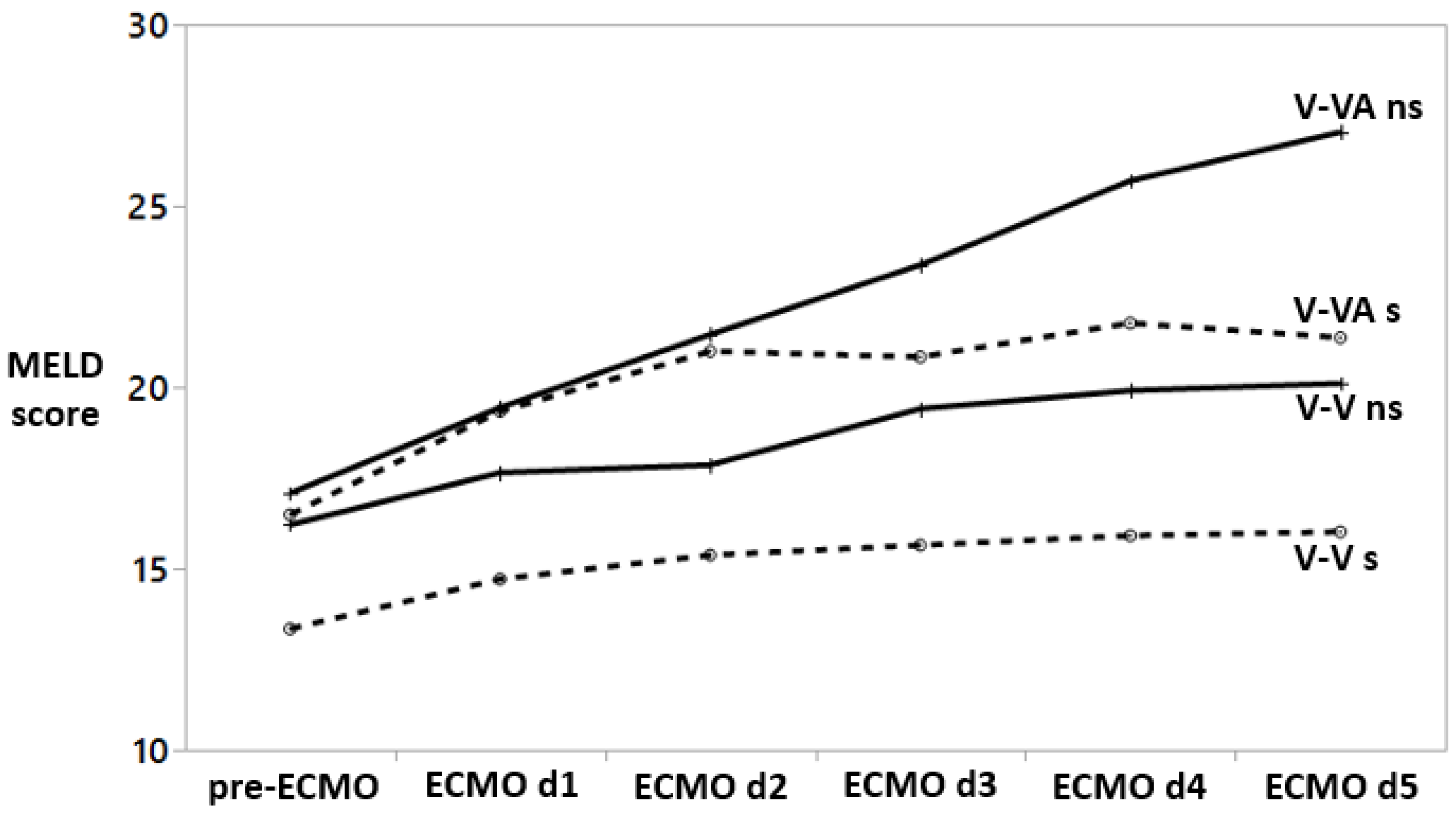
3.3. The Course of MELD Score
3.4. Outcome Predictors
3.5. The Impact of Liver Injury and a High Pre-ECMO MELD and SAPS II Scores on Outcome
4. Discussion
4.1. Acute Liver Injury
4.2. MELD Score as an Independent Outcome Predictor
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Model for End-Stage Liver Disease (MELD) Score
Appendix A.1. Factors Related to Pre-ECMO MELD Score

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors Affecting Pre-ECMO MELD Score | p-Values (Univariate) | p-Values (Multivariable) |
|---|---|---|
| Age > 60 years | 0.01 | 0.2 |
| Male sex | 0.03 | 0.05 |
| Body-Mass Index | 0.4 | |
| chronic liver disease | 0.1 | |
| chronic renal disease | 0.1 | |
| cardiac failure | 0.009 | 0.9 |
| septic shock | <0.0001 | 0.1 |
| acute liver injury | <0.0001 | 0.005 |
| SOFA score > 13 | <0.0001 | |
| PRESERVE score > 4 | 0.04 | 0.1 |
| RESP score < 2 | 0.6 | 0.8 |
| SAPS II > 75 | <0.0001 | <0.0001 |
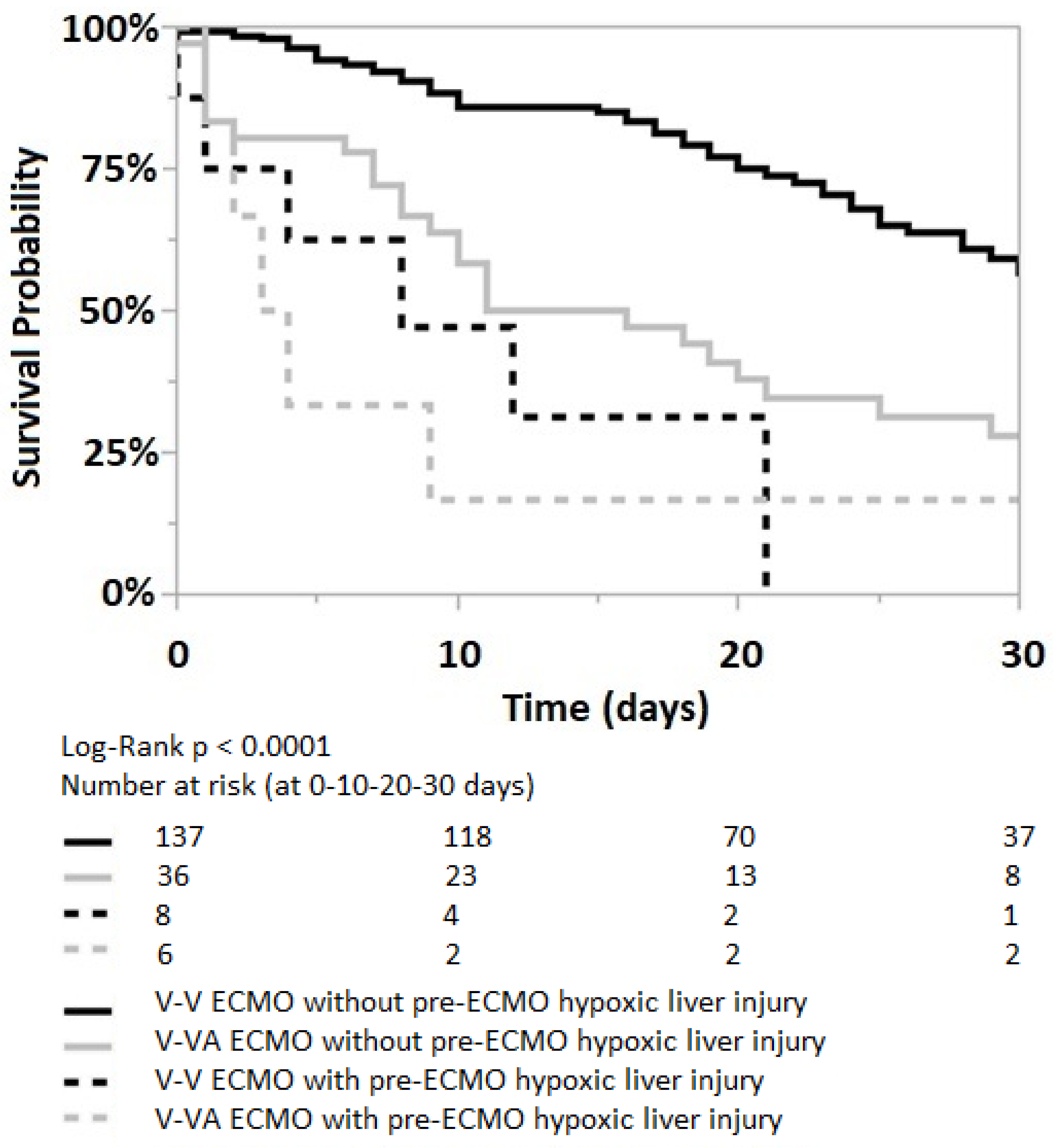
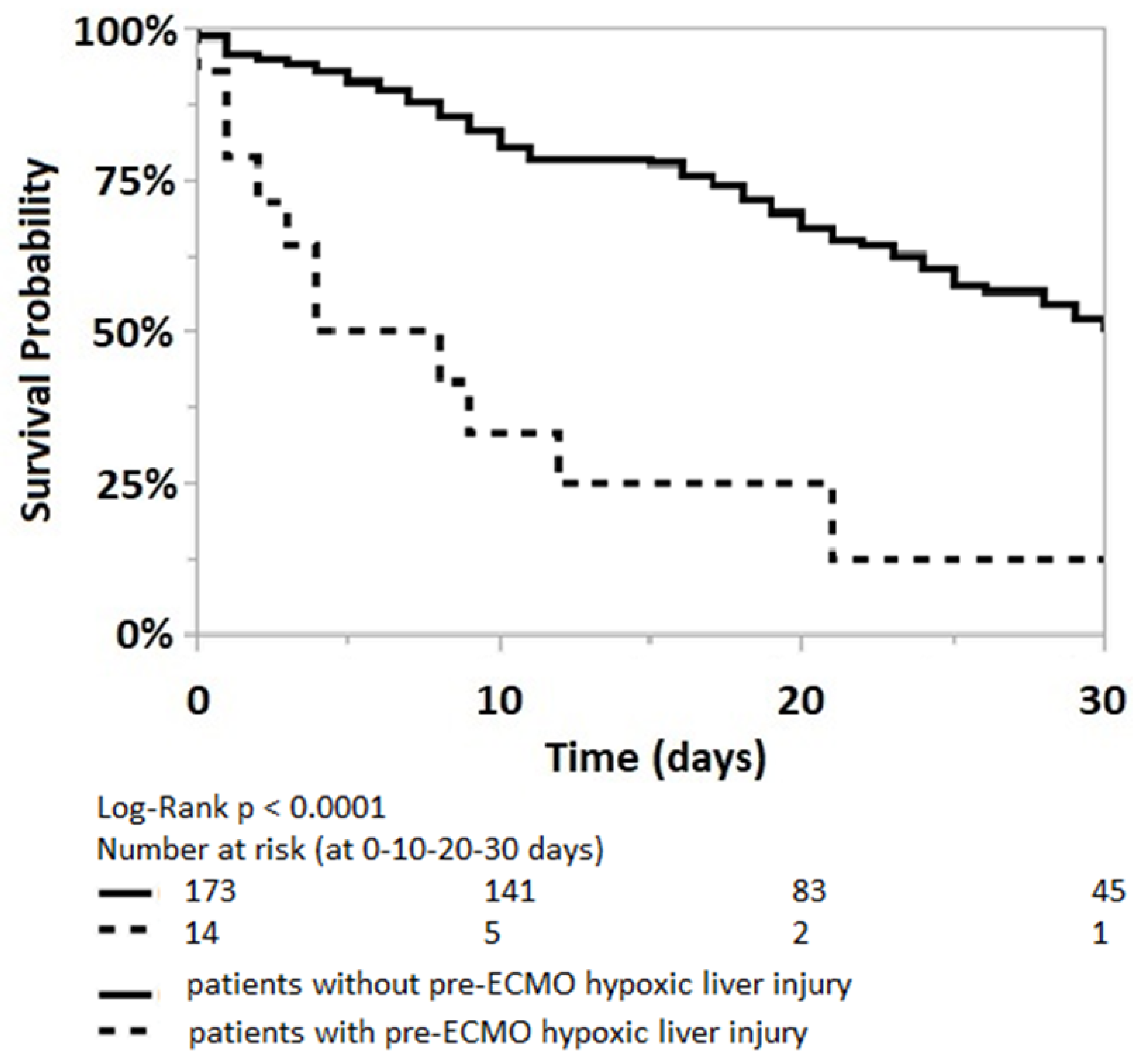
Appendix A.2. The Impact of Pre-ECMO Acute/Hypoxic Liver Injury

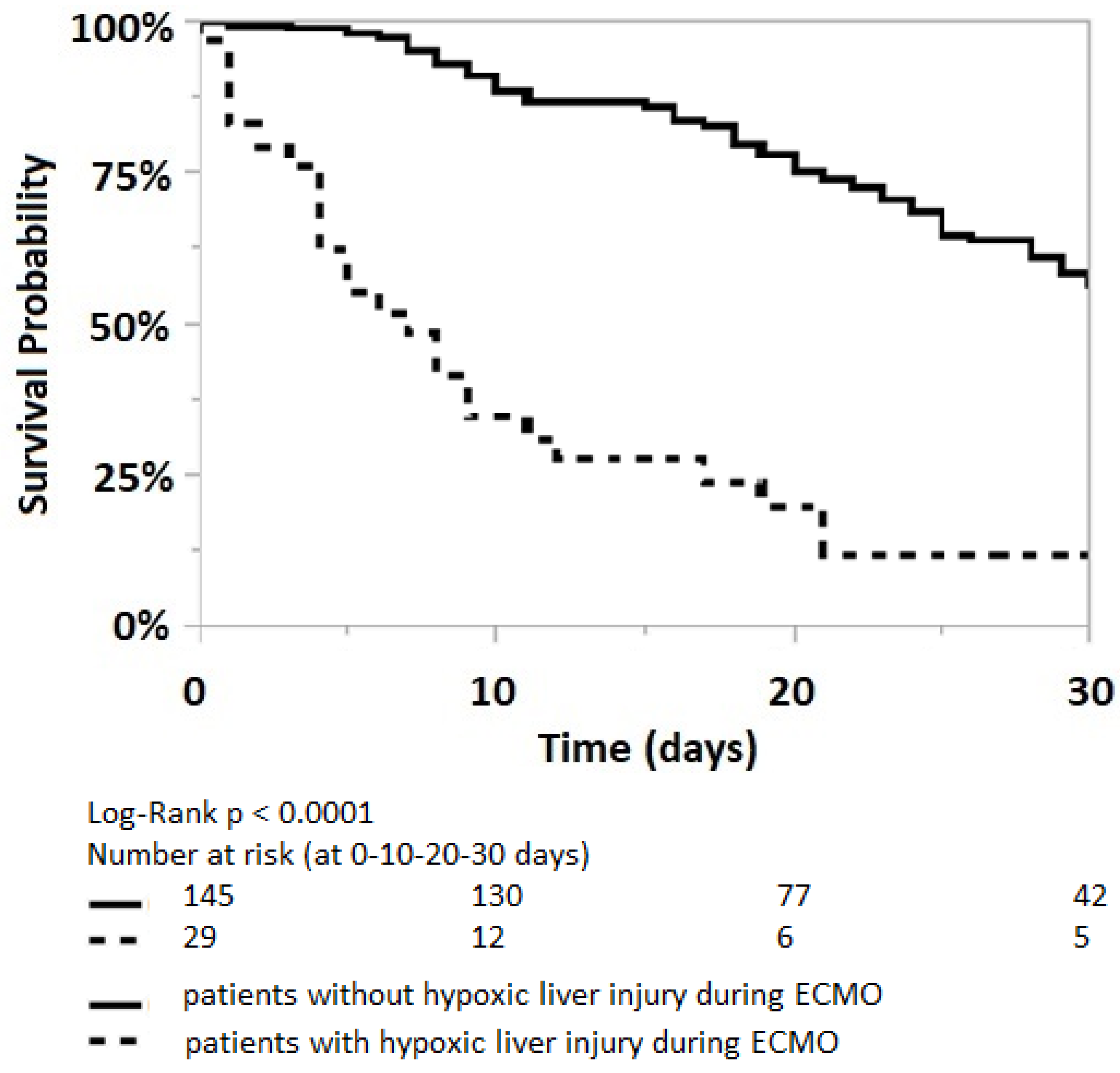
Appendix A.3. The Impact of Acute/Hypoxic Liver Injury during the First Five Days on ECMO

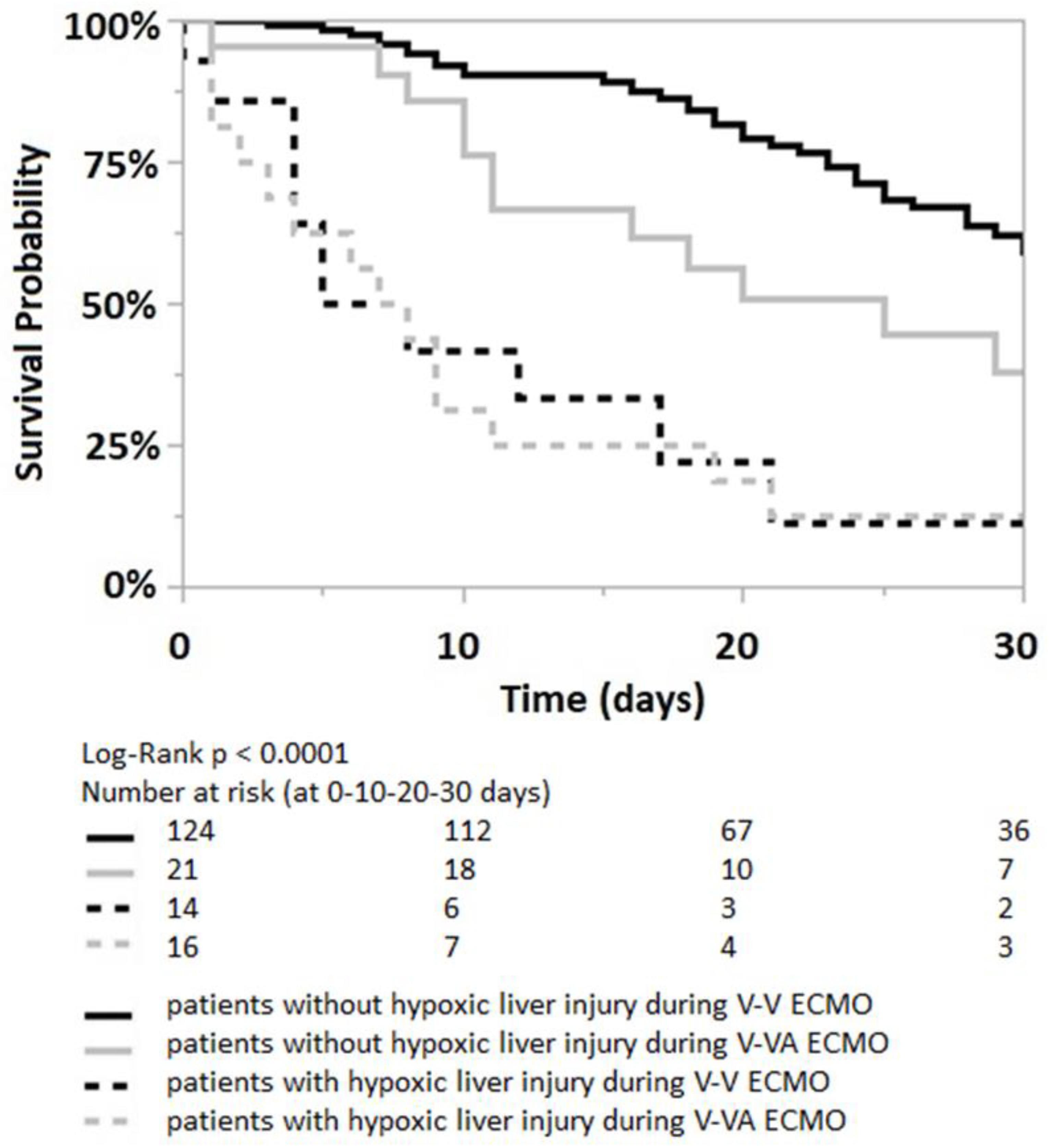
Appendix A.4. The Impact of V-V and V-VA ECMO Strategies in Patients with Acute Liver Injury

References
- Combes, A.; Peek, G.J.; Hajage, D.; Hardy, P.; Abrams, D.; Schmidt, M.; Dechartres, A.; Elbourne, D. ECMO for severe ARDS: Systematic review and individual patient data meta-analysis. Intensive Care Med. 2020, 46, 2048–2057. [Google Scholar] [CrossRef]
- Pappalardo, F.; Pieri, M.; Greco, T.; Patroniti, N.; Pesenti, A.; Arcadipane, A.; Ranieri, V.M.; Gattinoni, L.; Landoni, G.; Holzgraefe, B.; et al. Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: The ECMOnet score. Intensive Care Med. 2013, 39, 275–281. [Google Scholar] [CrossRef]
- Sandrio, S.; Krebs, J.; Leonardy, E.; Thiel, M.; Schoettler, J.J. Vasoactive Inotropic Score as a Prognostic Factor during (Cardio-) Respiratory ECMO. J. Clin. Med. 2022, 11, 2390. [Google Scholar] [CrossRef]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoue, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Kallet, R.H.; Lipnick, M.S.; Zhuo, H.; Pangilinan, L.P.; Gomez, A. Characteristics of Nonpulmonary Organ Dysfunction at Onset of ARDS Based on the Berlin Definition. Respir. Care 2019, 64, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Kurihara, C.; Manerikar, A.; Thakkar, S.; Saine, M.; Bharat, A. MELD Score Predicts Outcomes in Patients Undergoing Venovenous Extracorporeal Membrane Oxygenation. ASAIO J. 2020, 67, 871–877. [Google Scholar] [CrossRef]
- Lazzeri, C.; Bonizzoli, M.; Cianchi, G.; Batacchi, S.; Chiostri, M.; Fulceri, G.E.; Buoninsegni, L.T.; Peris, A. Bilirubin in the early course of venovenous extracorporeal membrane oxygenation support for refractory ARDS. J. Artif. Organs 2018, 21, 61–67. [Google Scholar] [CrossRef]
- Masha, L.; Peerbhai, S.; Boone, D.; Shobayo, F.; Ghotra, A.; Akkanti, B.; Zhao, Y.; Banjac, I.; Gregoric, I.D.; Kar, B. Yellow Means Caution: Correlations Between Liver Injury and Mortality with the Use of VA-ECMO. ASAIO J. 2019, 65, 812–818. [Google Scholar] [CrossRef]
- Schmidt, M.; Burrell, A.; Roberts, L.; Bailey, M.; Sheldrake, J.; Rycus, P.T.; Hodgson, C.; Scheinkestel, C.; Cooper, D.J.; Thiagarajan, R.R.; et al. Predicting survival after ECMO for refractory cardiogenic shock: The survival after veno-arterial-ECMO (SAVE)-score. Eur. Heart J. 2015, 36, 2246–2256. [Google Scholar] [CrossRef] [Green Version]
- Lescot, T.; Karvellas, C.; Beaussier, M.; Magder, S. Acquired liver injury in the intensive care unit. Anesthesiology 2012, 117, 898–904. [Google Scholar] [CrossRef]
- Matthews, J.C.; Pagani, F.D.; Haft, J.W.; Koelling, T.M.; Naftel, D.C.; Aaronson, K.D. Model for end-stage liver disease score predicts left ventricular assist device operative transfusion requirements, morbidity, and mortality. Circulation 2010, 121, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Kamath, P.S.; Heimbach, J.; Wiesner, R.H. Acute Liver Failure Prognostic Scores: Is Good Enough Good Enough? Clin. Gastroenterol. Hepatol. 2016, 14, 621–623. [Google Scholar] [CrossRef] [Green Version]
- Ayers, B.; Wood, K.; Melvin, A.; Prasad, S.; Gosev, I. MELD-XI is predictive of mortality in venoarterial extracorporeal membrane oxygenation. J. Card Surg. 2020, 35, 1275–1282. [Google Scholar] [CrossRef]
- Henrion, J.; Schapira, M.; Luwaert, R.; Colin, L.; Delannoy, A.; Heller, F.R. Hypoxic hepatitis: Clinical and hemodynamic study in 142 consecutive cases. Medicine 2003, 82, 392–406. [Google Scholar] [CrossRef]
- Waseem, N.; Chen, P.H. Hypoxic Hepatitis: A Review and Clinical Update. J. Clin. Transl. Hepatol. 2016, 4, 263–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekontso Dessap, A.; Boissier, F.; Charron, C.; Begot, E.; Repesse, X.; Legras, A.; Brun-Buisson, C.; Vignon, P.; Vieillard-Baron, A. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: Prevalence, predictors, and clinical impact. Intensive Care Med. 2016, 42, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Ling, R.R.; Ramanathan, K.; Poon, W.H.; Tan, C.S.; Brechot, N.; Brodie, D.; Combes, A.; MacLaren, G. Venoarterial extracorporeal membrane oxygenation as mechanical circulatory support in adult septic shock: A systematic review and meta-analysis with individual participant data meta-regression analysis. Crit. Care 2021, 25, 246. [Google Scholar] [CrossRef] [PubMed]
- Kon, Z.N.; Bittle, G.J.; Pasrija, C.; Pham, S.M.; Mazzeffi, M.A.; Herr, D.L.; Sanchez, P.G.; Griffith, B.P. Venovenous Versus Venoarterial Extracorporeal Membrane Oxygenation for Adult Patients With Acute Respiratory Distress Syndrome Requiring Precannulation Hemodynamic Support: A Review of the ELSO Registry. Ann. Thorac. Surg. 2017, 104, 645–649. [Google Scholar] [CrossRef] [Green Version]
- Vogel, D.J.; Murray, J.; Czapran, A.Z.; Camporota, L.; Ioannou, N.; Meadows, C.I.S.; Sherren, P.B.; Daly, K.; Gooby, N.; Barrett, N. Veno-arterio-venous ECMO for septic cardiomyopathy: A single-centre experience. Perfusion 2018, 33, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Ius, F.; Sommer, W.; Tudorache, I.; Avsar, M.; Siemeni, T.; Salman, J.; Puntigam, J.; Optenhoefel, J.; Greer, M.; Welte, T.; et al. Veno-veno-arterial extracorporeal membrane oxygenation for respiratory failure with severe haemodynamic impairment: Technique and early outcomes. Interact. Cardiovasc. Thorac. Surg. 2015, 20, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stohr, F.; Emmert, M.Y.; Lachat, M.L.; Stocker, R.; Maggiorini, M.; Falk, V.; Wilhelm, M.J. Extracorporeal membrane oxygenation for acute respiratory distress syndrome: Is the configuration mode an important predictor for the outcome? Interact. Cardiovasc. Thorac. Surg. 2011, 12, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grasselli, G.; Calfee, C.S.; Camporota, L.; Poole, D.; Amato, M.B.P.; Antonelli, M.; Arabi, Y.M.; Baroncelli, F.; Beitler, J.R.; Bellani, G.; et al. ESICM guidelines on acute respiratory distress syndrome: Definition, phenotyping and respiratory support strategies. Intensive Care Med. 2023, 49, 727–759. [Google Scholar] [CrossRef]
- OPTN Policies. Available online: https://optn.transplant.hrsa.gov/media/eavh5bf3/optn_policies.pdf (accessed on 27 November 2022).
- Organ Procurement and Transplantation Network, L.a.I.O.T.C. Clerical Changes for Implementation of Adding Serum Sodium to the MELD Score. Available online: https://optn.transplant.hrsa.gov/media/1575/policynotice_20151101.pdf (accessed on 27 November 2022).
- Kamath, P.S. MELD Score (Model for End-Stage Liver Disease) (12 and Older). Available online: https://www.mdcalc.com/meld-score-model-end-stage-liver-disease-12-older (accessed on 1 November 2022).
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef]
- Schmidt, M.; Zogheib, E.; Roze, H.; Repesse, X.; Lebreton, G.; Luyt, C.E.; Trouillet, J.L.; Brechot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Ucgun, I.; Ozakyol, A.; Metintas, M.; Moral, H.; Orman, A.; Bal, C.; Yildirim, H. Relationship between hypoxic hepatitis and cor pulmonale in patients treated in the respiratory ICU. Int. J. Clin. Pract. 2005, 59, 1295–1300. [Google Scholar] [CrossRef]
- Seeto, R.K.; Fenn, B.; Rockey, D.C. Ischemic hepatitis: Clinical presentation and pathogenesis. Am. J. Med. 2000, 109, 109–113. [Google Scholar] [CrossRef]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sern Lim, H. Baseline MELD-XI score and outcome from veno-arterial extracorporeal membrane oxygenation support for acute decompensated heart failure. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 82–88. [Google Scholar] [CrossRef] [PubMed]




| Survivors n = 95 | Nonsurvivors n = 92 | p Values | |
|---|---|---|---|
| Age (years) | 55 (42–61) | 57 (49–64) | 0.07 |
| Sex | female n = 29 (31%) male n = 66 (69%) | female n = 30 (33%) male n = 62 (67%) | 0.87 |
| Body-mass index (kg/m2) | 29 (25–35) | 27 (25–31) | 0.08 |
| ICU length of stay (days) | 21 (14–33) | 11.5 (6–24) | <0.0001 |
| ECMO strategies | |||
| n = 84 (88%) | n = 61 (66%) | 0.0004 |
| n = 11 (12%) | n = 31 (34%) | |
| Duration of ECMO support (days) | 12 (8–16) | 9.5 (4–19) | 0.08 |
| Clinical presentation prior to ECMO initiation other than respiratory failure: | |||
| n = 1 (1%) | n = 4 (4%) | 0.2 |
| n = 3 (3%) | n = 9 (4.5%) | 0.08 |
| n = 18 (19%) | n = 40 (43%) | 0.0005 |
| n = 53 (56%) | n = 62 (67%) | 0.13 |
| n = 3 (3%) | n = 11 (12%) | 0.03 |
| Bilirubin | 0.6 (0.3–1.2) | 0.9 (0.5–1.8) | 0.01 |
| Aspartate transaminase | 77 (38.2–146.5) | 143 (58.2–414) | 0.0002 |
| Alanine transaminase | 39 (28–70.2) | 53 (30–159) | 0.02 |
| Creatinine | 1.4 (0.7–2.4) | 1.8 (1.1–2.9) | 0.01 |
| INR | 1.1 (1.0–1.2) | 1.2 (1.1–1.5) | <0.0001 |
| MELD score | 12 (8–20) | 19 (11–23) | 0.0004 |
| SOFA score | 13 (11–16) | 15 (13–17.7) | 0.001 |
| PRESERVE score | 3 (2–5) | 4 (3–6) | 0.005 |
| RESP score | 1 (−2–3) | 0 (−2–2) | 0.04 |
| SAPS II score at ICU admission | 69 (59–80) | 78 (64–90) | 0.002 |
| Predicted mortality based on median SAPS II score | 82.6% | 91.2% | |
| Risk Factors | Cut-Off Values | p-Values (Univariate) | AUROC | p-Values (Multivariable) |
|---|---|---|---|---|
| Age | 60 | 0.06 | 0.58 | |
| Male sex | 0.9 | |||
| Body-Mass Index | 27.7 | 0.4 | 0.60 | |
| ECMO type (V-V or V-VA) | 0.0003 | 0.2 | ||
| Cardiac failure | 0.0003 | 0.4 | ||
| Septic shock | 0.1 | |||
| Chronic liver disease | 0.2 | |||
| Chronic renal disease | 0.06 | |||
| Acute liver injury | 0.03 | 0.2 | ||
| Bilirubin | 0.63 | 0.03 | 0.60 | |
| Aspartate transaminase | 112 | 0.0008 | 0.66 | |
| Alanine transaminase | 109 | 0.02 | 0.6 | |
| Creatinine | 1.6 | 0.23 | 0.60 | |
| INR | 1.15 | <0.0001 | 0.69 | |
| MELD score | 16 | 0.0001 | 0.65 | 0.04 |
| SOFA score | 13 | 0.001 | 0.64 | 0.6 |
| PRESERVE score | 4 | 0.009 | 0.61 | 0.06 |
| RESP score | 2 | 0.05 | 0.58 | 0.7 |
| SAPS II at admission | 75 | 0.002 | 0.63 | 0.09 |
| Risk Factors | Hazard Ratios (95% CI) | p Values |
|---|---|---|
| Pre-ECMO acute liver injury | ||
| 4.5 (2.3–8.5) | <0.0001 |
| 5.4 (2.3–12.9) | 0.0001 |
| 2.4 (0.9–6.3) | 0.07 |
| Acute liver injury during ECMO * | ||
| 4.7 (2.9–7.6) | <0.0001 |
| 5.7 (2.9–11.2) | <0.0001 |
| 2.7 (1.3–5.8) | 0.01 |
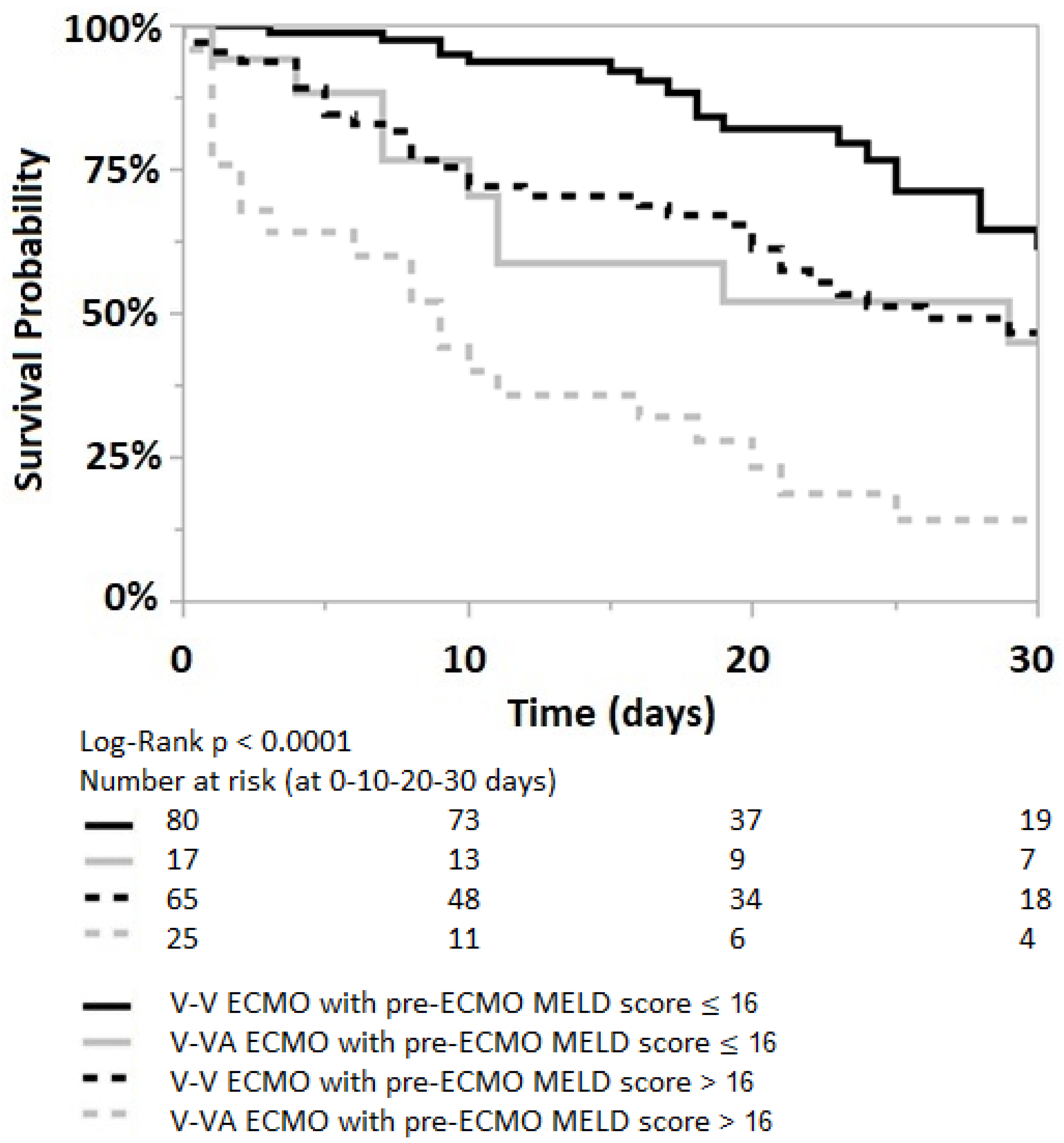
| Pre-ECMO MELD score > 16 | ||
| 1.9 (1.3–3.0) | 0.002 |
| 1.7 (1.0–2.8) | 0.04 |
| 2.6 (1.2–5.6) | 0.01 |
| SAPS II > 75 | ||
| 2.3 (1.5–3.5) | 0.0001 |
| 1.9 (1.1–3.1) | 0.01 |
| 4 (1.8–8.6) | 0.0004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandrio, S.; Thiel, M.; Krebs, J. The Outcome Relevance of Pre-ECMO Liver Impairment in Adults with Acute Respiratory Distress Syndrome. J. Clin. Med. 2023, 12, 4860. https://doi.org/10.3390/jcm12144860
Sandrio S, Thiel M, Krebs J. The Outcome Relevance of Pre-ECMO Liver Impairment in Adults with Acute Respiratory Distress Syndrome. Journal of Clinical Medicine. 2023; 12(14):4860. https://doi.org/10.3390/jcm12144860
Chicago/Turabian StyleSandrio, Stany, Manfred Thiel, and Joerg Krebs. 2023. "The Outcome Relevance of Pre-ECMO Liver Impairment in Adults with Acute Respiratory Distress Syndrome" Journal of Clinical Medicine 12, no. 14: 4860. https://doi.org/10.3390/jcm12144860