

Predictors of Conduction Disturbances Requiring New Permanent Pacemaker Implantation following Transcatheter Aortic Valve Implantation Using the Evolut Series
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
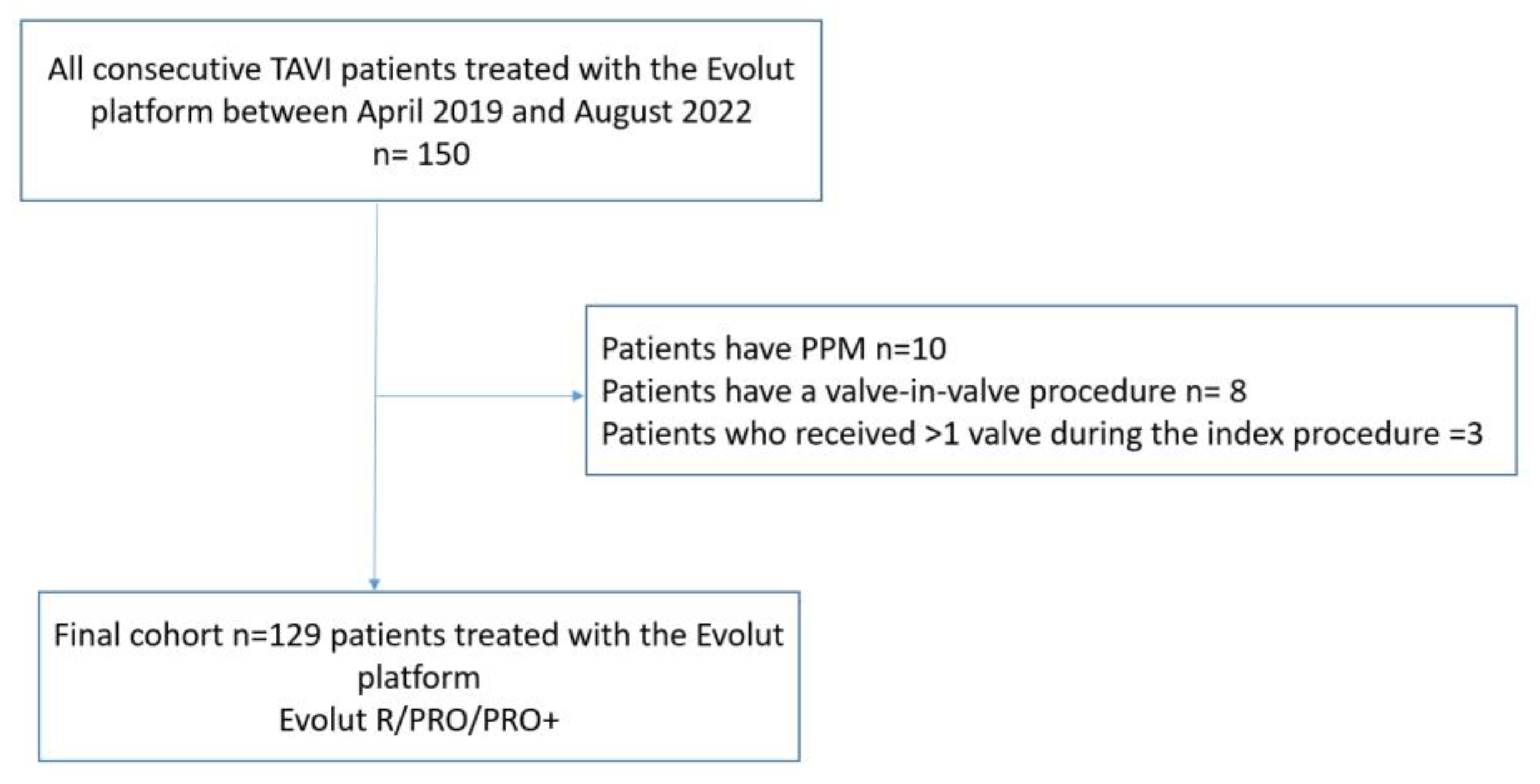
2.1. Study Design and Patient Population
2.2. TAVI Procedure
2.3. MSCT Analysis
2.4. ID Measurement
2.5. ECG Data
2.6. Clinical Data and TAVI Clinical Outcome
2.7. Study Outcome
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Conduction Disturbance
3.3. Predictors of New PPM
3.4. Multivariate Predictors of New PPM
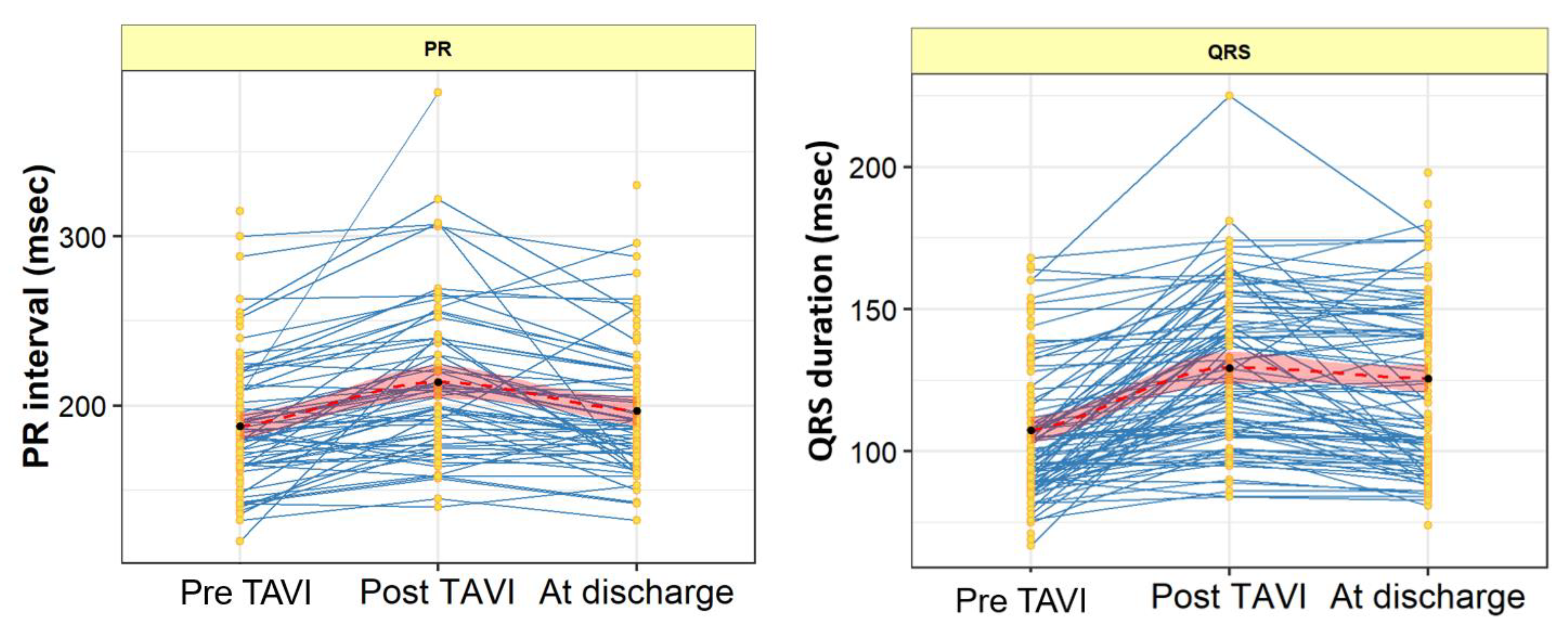
3.5. PR Interval and QRS Duration Changes from Baseline to Post-Procedure and Discharge
3.6. Procedural and Short-Term Outcomes
4. Discussion
- (1)
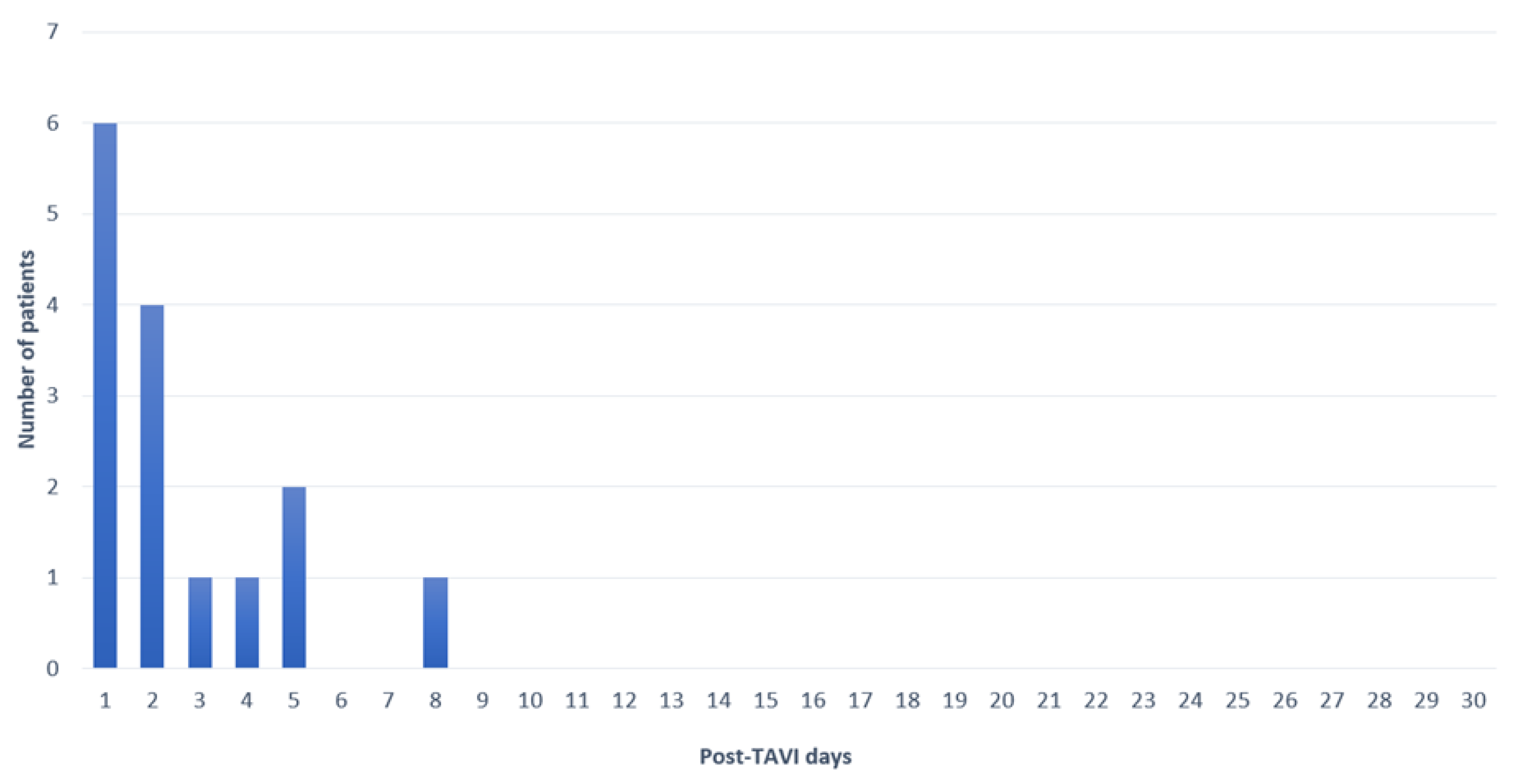
- At 30 days, the rate of new PPM implantation was 11.6%.
- (2)
- On multivariate analysis, pre-existing RBBB, MS length, and ID were found to be the strongest predictors of new PPM.
- (3)
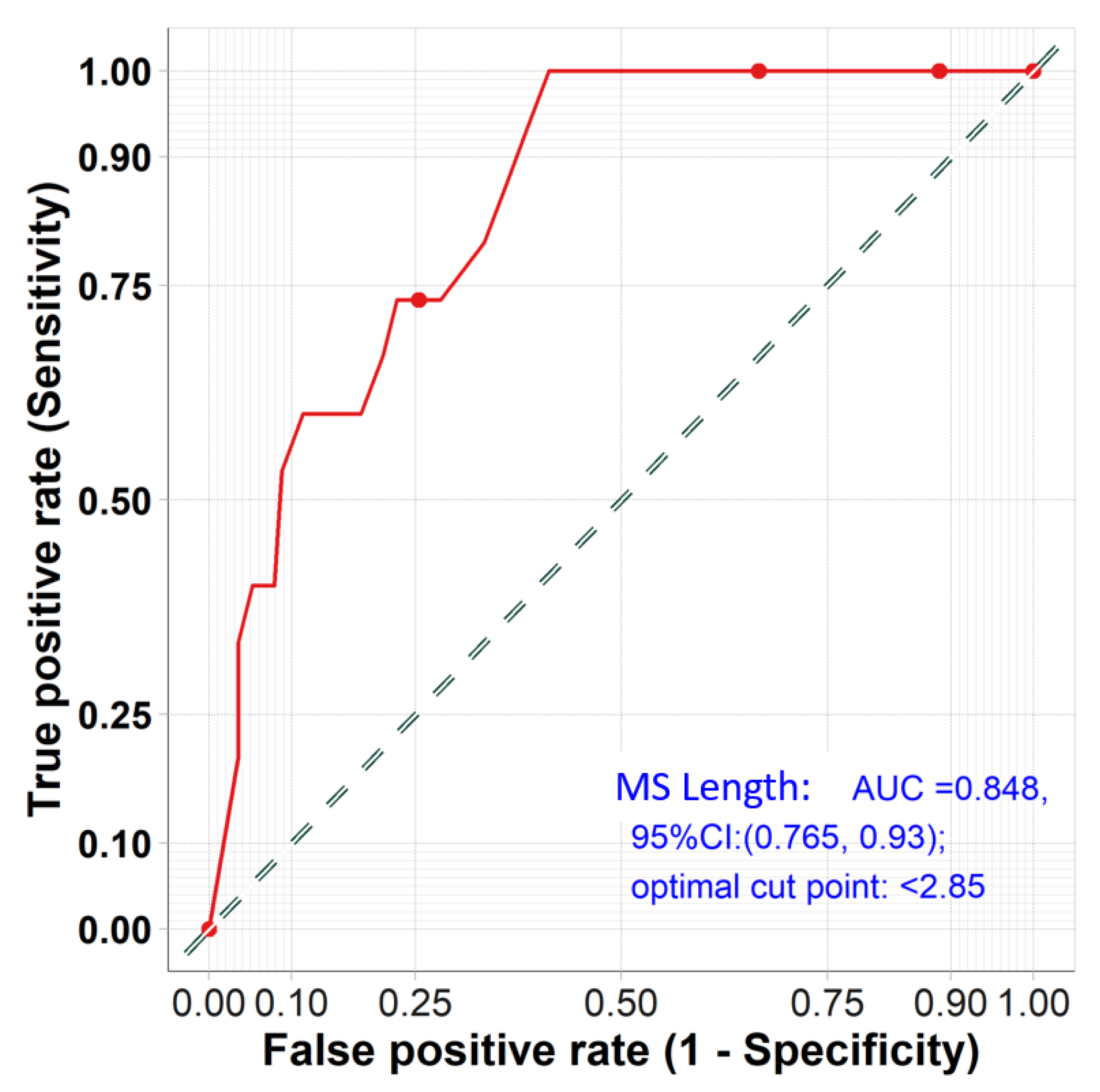
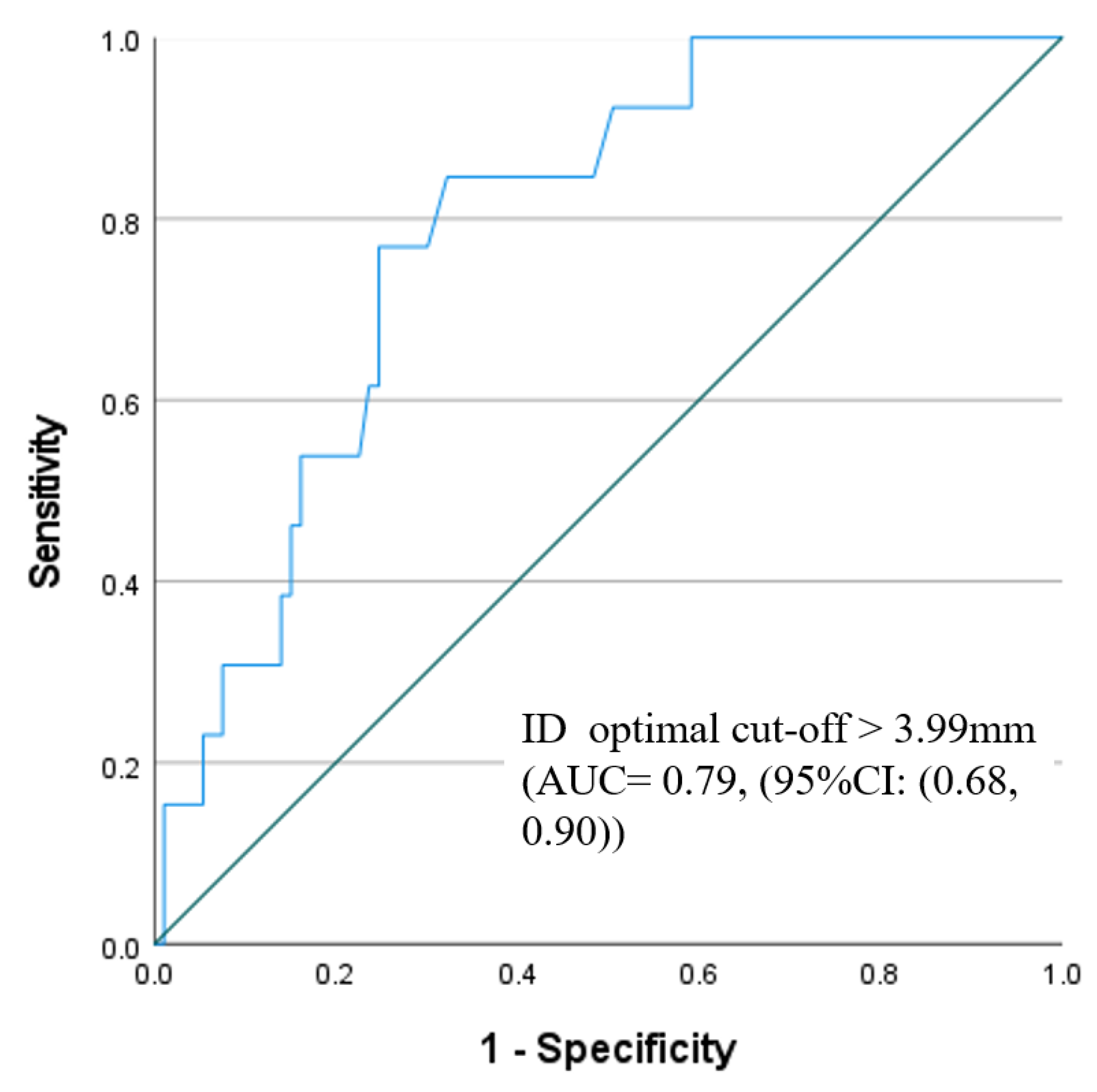
- The optimal membranous septum length cut-off to predict new PPM was <2.85 mm AUC = 0.85, (95% CI: 0.77–0.93) while the optimal implantation depth cut-off was >3.99 mm and AUC = 0.79 (95% CI: 0.68–0.90).
- (4)
- Detailed ECG analysis showed significant prolongation of the PR interval and QRS duration post-TAVI. The PR interval prolongation recovered pre-discharge, while QRS duration persisted until discharge compared to the baseline measurements.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Faroux, L.; Chen, S.; Muntané-Carol, G.; Regueiro, A.; Philippon, F.; Sondergaard, L.; Jørgensen, T.H.; Lopez-Aguilera, J.; Kodali, S.; Leon, M.; et al. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: A systematic review and meta-analysis. Eur. Heart J. 2020, 41, 2771–2781. [Google Scholar] [CrossRef]
- Sammour, Y.; Krishnaswamy, A.; Kumar, A.; Puri, R.; Tarakji, K.G.; Bazarbashi, N.; Harb, S.; Griffin, B.; Svensson, L.; Wazni, O.; et al. Incidence, Predictors, and Implications of Permanent Pacemaker Requirement after Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2021, 14, 115–134. [Google Scholar] [CrossRef]
- Moreno, R.; Dobarro, D.; LóPez De Sá, E.; Prieto, M.; Morales, C.; Calvo Orbe, L.; Moreno-Gomez, I.; Filgueiras, D.; Sanchez-Recalde, A.; Galeote, G.; et al. Cause of Complete Atrioventricular Block after Percutaneous Aortic Valve Implantation. Circulation 2009, 120, e29–e30. [Google Scholar] [CrossRef] [Green Version]
- van Rosendael, P.J.; Delgado, V.; Bax, J.J. Pacemaker implantation rate after transcatheter aortic valve implantation with early and new-generation devices: A systematic review. Eur. Heart J. 2018, 39, 2003–2013. [Google Scholar] [CrossRef]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction Disturbances after Transcatheter Aortic Valve Replacement. Circulation 2017, 136, 1049–1069. [Google Scholar] [CrossRef]
- Saia, F.; Gandolfo, C.; Palmerini, T.; Berti, S.; Doshi, S.N.; Laine, M.; Marcelli, C.; Piva, T.; Ribichini, F.; De Benedictis, M.; et al. In-hospital and thirty-day outcomes of the SAPIEN 3 Ultra balloon-expandable transcatheter aortic valve: The S3U registry. EuroIntervention 2020, 15, 1240–1247. [Google Scholar] [CrossRef] [Green Version]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef]
- Kroon, H.G.; van Gils, L.; Ziviello, F.; van Wiechen, M.; Ooms, J.; Rahhab, Z.; El Faquir, N.; Maugenest, A.-M.; Kardys, I.; Daemen, J.; et al. Impact of Baseline and Newly Acquired Conduction Disorders on Need for Permanent Pacemakers with 3 Consecutive Generations of Self-Expanding Transcatheter Aortic Heart Valves. Cardiovasc. Revascularization Med. 2022, 34, 40–45. [Google Scholar] [CrossRef]
- Chen, Y.H.; Chang, H.H.; Liao, T.W.; Leu, H.B.; Chen, I.M.; Chen, P.L.; Lin, S.M. Membranous septum length predicts conduction disturbances following transcatheter aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2022, 164, 42–51.e2. [Google Scholar] [CrossRef]
- Hokken, T.W.; van Wiechen, M.P.; Ooms, J.F.; El Azzouzi, I.; de Ronde, M.; Kardys, I.; Budde, R.; Daemen, J.; de Jaegere, P.P.; Van Mieghem, N.M. Impact of Interventricular membranous septum length on pacemaker need with different Transcatheter aortic valve implantation systems. Int. J. Cardiol. 2021, 333, 152–158. [Google Scholar] [CrossRef]
- Jilaihawi, H.; Zhao, Z.; Du, R.; Staniloae, C.; Saric, M.; Neuburger, P.J.; Querijero, M.; Vainrib, A.; Hisamoto, K.; Ibrahim, H.; et al. Minimizing Permanent Pacemaker Following Repositionable Self-Expanding Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 1796–1807. [Google Scholar] [CrossRef]
- Blanke, P.; Weir-McCall, J.R.; Achenbach, S.; Delgado, V.; Hausleiter, J.; Jilaihawi, H.; Marwan, M.; Nørgaard, B.L.; Piazza, N.; Schoenhagen, P.; et al. Computed Tomography Imaging in the Context of Transcatheter Aortic Valve Implantation (TAVI)/Transcatheter Aortic Valve Replacement (TAVR): An Expert Consensus Document of the Society of Cardiovascular Computed Tomography. JACC Cardiovasc. Imaging 2019, 12, 1–24. [Google Scholar] [CrossRef]
- Higgins, J.; Mayo, J.; Skarsgard, P. Cardiac Computed Tomography Facilitates Operative Planning in Patients with Mitral Calcification. Ann. Thorac. Surg. 2013, 95, e9–e11. [Google Scholar] [CrossRef]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part III: Intraventricular Conduction Disturbances a Scientific Statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society Endorsed by the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar] [CrossRef] [Green Version]
- Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; Blackstone, E.H.; et al. Valve Academic Research Consortium 3: Updated Endpoint Definitions for Aortic Valve Clinical Research. J. Am. Coll. Cardiol. 2021, 77, 2717–2746. [Google Scholar] [CrossRef]
- Kawashima, T.; Sasaki, H. A macroscopic anatomical investigation of atrioventricular bundle locational variation relative to the membranous part of the ventricular septum in elderly human hearts. Surg. Radiol. Anat. 2005, 27, 206–213. [Google Scholar] [CrossRef]
- Hokken, T.W.; Muhemin, M.; Okuno, T.; Veulemans, V.; Lopes, B.B.; Beneduce, A.; Vittorio, R.; Ooms, J.F.; Adrichem, R.; Neleman, T.; et al. Impact of membranous septum length on pacemaker need with different transcatheter aortic valve replacement systems: The INTERSECT registry. J. Cardiovasc. Comput. Tomogr. 2022, 16, 524–530. [Google Scholar] [CrossRef]
- Sammour, Y.; Banerjee, K.; Kumar, A.; Lak, H.; Chawla, S.; Incognito, C.; Patel, J.; Kaur, M.; Abdelfattah, O.; Svensson, L.G.; et al. Systematic Approach to High Implantation of SAPIEN-3 Valve Achieves a Lower Rate of Conduction Abnormalities Including Pacemaker Implantation. Circ. Cardiovasc. Interv. 2021, 14, e009407. [Google Scholar] [CrossRef]
- Sá, M.P.; Van den Eynde, J.; Jacquemyn, X.; Erten, O.; Rodriguez, R.; Goldman, S.; Coady, P.M.; Gnall, E.; Gray, W.A.; Jarrett, H.; et al. Computed tomography-derived membranous septum length as predictor of conduction abnormalities and permanent pacemaker implantation after TAVI: A meta-analysis of observational studies. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2023, 101, 1203–1213. [Google Scholar] [CrossRef]
- Gada, H.; Vora, A.N.; Tang, G.H.L.; Mumtaz, M.; Forrest, J.K.; Laham, R.J.; Yakubov, S.J.; Deeb, G.M.; Rammohan, C.; Huang, J.; et al. Site-Level Variation and Predictors of Permanent Pacemaker Implantation Following TAVR in the Evolut Low-Risk Trial. Cardiovasc. Revascularization Med. 2023, 47, 48–54. [Google Scholar] [CrossRef]
- Grubb, K.J.; Gada, H.; Mittal, S.; Nazif, T.; Rodés-Cabau, J.; Fraser, D.G.W.; Lin, L.; Rovin, J.D.; Khalil, R.; Sultan, I.; et al. Clinical Impact of Standardized TAVR Technique and Care Pathway: Insights from the Optimize PRO Study. JACC Cardiovasc. Interv. 2023, 16, 558–570. [Google Scholar] [CrossRef]
- Panagides, V.; Mesnier, J.; Nuche, J.; Delarochellière, R.; Paradis, J.-M.; Kalavrouziotis, D.; Dumont, E.; Mohammadi, S.; Rodes-Cabau, J. From the Evolut Pro to the Evolut FX self-expanding transcatheter aortic valve replacement systems: Current status and future perspectives. Expert Rev. Med. Devices 2022, 19, 561–569. [Google Scholar] [CrossRef]
- Khera, S.; Krishnamoorthy, P.; Sharma, S.K.; Kini, A.S.; Dangas, G.D.; Goel, S.; Lerakis, S.; Anastasius, M.; Moreno, P.; Tang, G.H.L. Improved Commissural Alignment in TAVR with the Newest Evolut FX Self-Expanding Supra-Annular Valve: First-in-Human Experience. JACC Cardiovasc. Interv. 2022, 16, 498–500. [Google Scholar] [CrossRef]
- Manuel, A.M.; Almeida, J.; Guerreiro, C.; Dias, T.; Barbosa, A.; Teixeira, P.; Ribeiro, J.; Dias, A.; Caeiro, D.; Fonseca, M.; et al. The effects of transcatheter aortic valve implantation on cardiac electrical properties. Rev. Port. Cardiol. 2020, 39, 431–440. [Google Scholar] [CrossRef]
- Castro-Mejía, A.F.; Amat-Santos, I.; Ortega-Armas, M.E.; Baz, J.A.; Moreno, R.; Diaz, J.F.; Travieso, A.; Jimenez-Quevedo, P.; Santos-Martínez, S.; McInerney, A.; et al. Development of atrioventricular and intraventricular conduction disturbances in patients undergoing transcatheter aortic valve replacement with new generation self-expanding valves: A real world multicenter analysis. Int. J. Cardiol. 2022, 362, 128–136. [Google Scholar] [CrossRef]
- Lilly, S.M.; Deshmukh, A.J.; Epstein, A.E.; Ricciardi, M.J.; Shreenivas, S.; Velagapudi, P.; Wyman, J.F. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 76, 2391–2411. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 129 | PPM n = 15 | No PPM n = 114 | p Value | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age (years) | 81.3 ± 5.3 | 81.7 ± 4.3 | 82.1 ± 5.3 | 0.36 |
| Female, n (%) | 46 (36%) | 2 (13%) | 44 (38.6%) | 0.08 |
| Body Mass Index (kg/m2) | 26.8 [24.1, 31.1] | 30 [23.7, 33.8] | 26.8 [24.1, 30.7] | 0.35 |
| Hypertension, n (%) | 99 (77%) | 13 (87%) | 86 (75%) | 0.51 |
| Diabetes, n (%) | 43 (33%) | 7 (47%) | 36 (32%) | 0.25 |
| Dyslipidemia, n (%) | 73 (57%) | 12 (80%) | 61 (54%) | 0.058 |
| NYHA class ≥ III, n (%) | 76 (59%) | 6 (40%) | 70 (61.4%) | 0.16 |
| COPD, n (%) | 22 (17%) | 2 (13%) | 20 (18%) | >0.999 |
| Previous MI, n (%) | 19 (15%) | 2 (13%) | 17 (15%) | >0.999 |
| Prior CVA | 14 (11%) | 4 (27%) | 10 (9%) | 0.059 |
| Glomerular filtration rate (mL/min/1.73 m2) | 61.1 ± 16.7 | 59.1 ± 15.4 | 55.6 ± 20.3 | 0.42 |
| EuroSCORE II | 3.2 [2.0, 5.4] | 1.9 [1.7, 3.2] | 3.3 [2.1, 5.4] | 0.008 |
| Baseline ECG | ||||
| Atrial Fibrillation, n (%) | 28 (22%) | 2 (13%) | 26 (23%) | 0.52 |
| RBBB | 16 (12%) | 7 (47%) | 9 (8%) | <0.001 |
| LBBB | 12 (10%) | 0 (0%) | 12 (11%) | 0.35 |
| 1st-degree AV block | 32 (25%) | 4 (27%) | 28 (25%) | 0.92 |
| PR interval | 183 [164, 209.5] | 178 [156, 207.5] | 184 [164, 212] | 0.57 |
| QRS duration | 101 [89, 119] | 120 [89, 140] | 101 [89, 113] | 0.18 |
| Echocardiographic data | ||||
| LVEF ≤ 40% | 33 (26%) | 3 (20%) | 30 (26%) | 0.75 |
| Mean AoV gradient (mmHg) | 54.1 ± 32.4 | 60.1 ± 15.7 | 53.3 ± 34.1 | 0.45 |
| Peak AoV gradient (mmHg) | 80.8 ± 20.5 | 89.1 ± 18.3 | 79.6 ± 20.7 | 0.45 |
| MSCT characteristics | ||||
| Bicuspid morphology | 26 (20%) | 5 (33%) | 21 (18%) | 0.18 |
| Annulus diameter (mm) | 25.3± 2.5 | 26.3± 2.7 | 25.2 ± 2.4 | 0.08 |
| Annular eccentricity index | 0.25 ± 0.06 | 0.27 ± 0.05 | 0.24 ± 0.06 | 0.17 |
| Perimeter-derived annulus diameter (mm) | 25.5 ± 2.2 | 26.5 ± 2.6 | 25.3 ± 2.3 | 0.09 |
| Area-derived annulus diameter (mm) | 24.9 ± 2.2 | 25.9 ± 2.7 | 24.8 ± 2.3 | 0.07 |
| Annulus perimeter (mm) | 80.4 ± 7.1 | 82.9 ± 8.1 | 79.9 ± 7.5 | 0.14 |
| Annulus area (mm2) | 493.1 ± 88.1 | 530.5 ± 104.9 | 487.9 ± 90.9 | 0.09 |
| LCA height (mm) | 16.3 ± 3.3 | 16.1 ± 4.2 | 16 ± 3.2 | 0.93 |
| RCA height (mm) | 18.9 ± 3.5 | 18.8 ± 3.8 | 18.7 ± 3.6 | 0.88 |
| Aortic root angulation ≥ 49 | 56 (43%) | 8 (53%) | 48 (42%) | 0.42 |
| Membranous septum length (mm) | 3 [2.1, 3.8] | 1.5 [1.1, 2.5] | 3.1 [2.3, 4] | <0.001 |
| AoV calcification ≥ moderate | 106 (82%) | 14 (93%) | 92 (81%) | 0.30 |
| LVOT calcification ≥ moderate | 31 (24%) | 4 (27%) | 27 (24%) | 0.75 |
| MAC ≥ moderate | 46 (36%) | 9 (60%) | 37 (33%) | 0.047 |
| All Patients n = 129 | PPM n = 15 | No PPM n = 114 | p Value | |
|---|---|---|---|---|
| Procedural characteristics | ||||
| THV type | 0.78 | |||
| Evolut R | 34 (26%) | 5 (33%) | 29 (25%) | |
| Evolut PRO | 45 (35%) | 5 (33%) | 40 (35%) | |
| Evolut PRO+ | 50 (39%) | 5 (33%) | 45 (40%) | |
| THV size | 0.81 | |||
| 23 mm | 2 (2%) | 0 (0%) | 2 (2%) | |
| 26 mm | 23 (18%) | 2 (13%) | 21 (18%) | |
| 29 mm | 64 (50%) | 7 (47%) | 57 (50%) | |
| 34 mm | 40 (31%) | 6 (40%) | 34 (30%) | |
| Oversizing by annulus perimeter | 17.8 [13.6, 21.9] | 18 [10.6, 20.4] | 17.7 [13.9, 22] | 0.39 |
| Oversizing by annulus area | 45.2 [35.1, 57] | 45.9 [28.2, 55.8] | 44.11 [36, 57.1] | 0.35 |
| Balloon pre-dilation n (%) | 89 (69%) | 12 (80%) | 77 (68%) | 0.39 |
| Capture–redeployment attempts n (%) | 55 (42.6%) | 6 (40%) | 49 (43%) | 0.83 |
| Capture–redeployment numbers | 2.3 ± 1.5 | 2.3 ± 1.5 | 2.3 ± 1 | 0.96 |
| Balloon post-dilation | 51 (40%) | 8 (53%) | 43 (39%) | 0.27 |
| Cusp overlap | 83 (64%) | 76 (67%) | 7 (47%) | 0.16 |
| Implantation depth at NCC (mm) | 3.8 [2.8, 4.3] | 4.4 [4.1, 5.7] | 3.6 [2.6, 4.1] | <0.001 |
| MS length minus implant depth, (mm) | −0.6 ± 2.5 | −3.9 ± 1.5 | −0.3 ± 2.4 | <0.001 |
| ID > MS | 64 (50%) | 13 (87%) | 51 (45%) | 0.002 |
| In-hospital complications | ||||
| In-hospital death | 3 (2%) | 0 (0%) | 3 (3%) | >0.999 |
| Periprocedural MI | 0 (0%) | 0 (0%) | 0 (0%) | - |
| In-hospital stroke | 5 (4%) | 1 (7%) | 4 (4%) | 0.48 |
| Vascular complications | ||||
| Major | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Minor | 20 (16%) | 2 (13%) | 18 (16%) | >0.999 |
| PVL ≥ moderate (echo) | 8 (6%) | 1 (7%) | 7 (6%) | >0.999 |
| Predictors | Univariate Analysis | Adjusted Regression Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Preprocedural aspects | ||||
| EuroSCORE II | 0.62 (0.40–0.95) | 0.028 | ||
| RBBB | 10.21 (3.01–239.8) | <0.001 | 26.343 (3.924–176.837) | 0.001 |
| Membranous septum length | 0.34 (0.19–0.58) | <0.001 | 0.276 (0.132–0.576) | 0.001 |
| MAC ≥ moderate | 3.12 (1.03–9.42) | 0.043 | ||
| Procedural aspects | ||||
| Implantation depth at NCC | 1.62 (0.16–2.25) | 0.004 | 1.576 (1.020–2.435) | 0.04 |
| MS length minus implant depth | 0.56 (0.41–0.76) | <0.001 | ||
| Time | Median [IQR] | p-Value | |
|---|---|---|---|
| PR interval (msec) | Pre TAVI * | 182 [164, 209] | - |
| Post TAVI | 208 [178, 240] | 0.002 | |
| At discharge | 188 [171, 219] | 0.064 | |
| QRS dutaion (msec) | Pre TAVI * | 101 [89, 119] | - |
| Post TAVI | 127 [107, 150] | <0.001 | |
| At discharge | 125 [100, 149] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelshafy, M.; Elkoumy, A.; Elzomor, H.; Abdelghani, M.; Campbell, R.; Kennedy, C.; Kenny Gibson, W.; Fezzi, S.; Nolan, P.; Wagener, M.; et al. Predictors of Conduction Disturbances Requiring New Permanent Pacemaker Implantation following Transcatheter Aortic Valve Implantation Using the Evolut Series. J. Clin. Med. 2023, 12, 4835. https://doi.org/10.3390/jcm12144835
Abdelshafy M, Elkoumy A, Elzomor H, Abdelghani M, Campbell R, Kennedy C, Kenny Gibson W, Fezzi S, Nolan P, Wagener M, et al. Predictors of Conduction Disturbances Requiring New Permanent Pacemaker Implantation following Transcatheter Aortic Valve Implantation Using the Evolut Series. Journal of Clinical Medicine. 2023; 12(14):4835. https://doi.org/10.3390/jcm12144835
Chicago/Turabian StyleAbdelshafy, Mahmoud, Ahmed Elkoumy, Hesham Elzomor, Mohammad Abdelghani, Ruth Campbell, Ciara Kennedy, William Kenny Gibson, Simone Fezzi, Philip Nolan, Max Wagener, and et al. 2023. "Predictors of Conduction Disturbances Requiring New Permanent Pacemaker Implantation following Transcatheter Aortic Valve Implantation Using the Evolut Series" Journal of Clinical Medicine 12, no. 14: 4835. https://doi.org/10.3390/jcm12144835