
The Croatian Primary Sjögren’s Disease Oral Health Study: Oral Status and Oral Health-Related Quality of Life

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
- -
- Intake of anticholinergics, tricyclic antidepressants, antihypertensives, and antihistamines; systemic diseases (such as anorexia, bulimia, diabetes, HIV infection, hepatitis C (HCV)) that could cause salivary gland dysfunction,
- -
- Radiation therapy to the head and neck region,
- -
- Smoking.
2.2. Outcomes Measures
2.3. Statistical Analysis
3. Results
3.1. Study Subjects
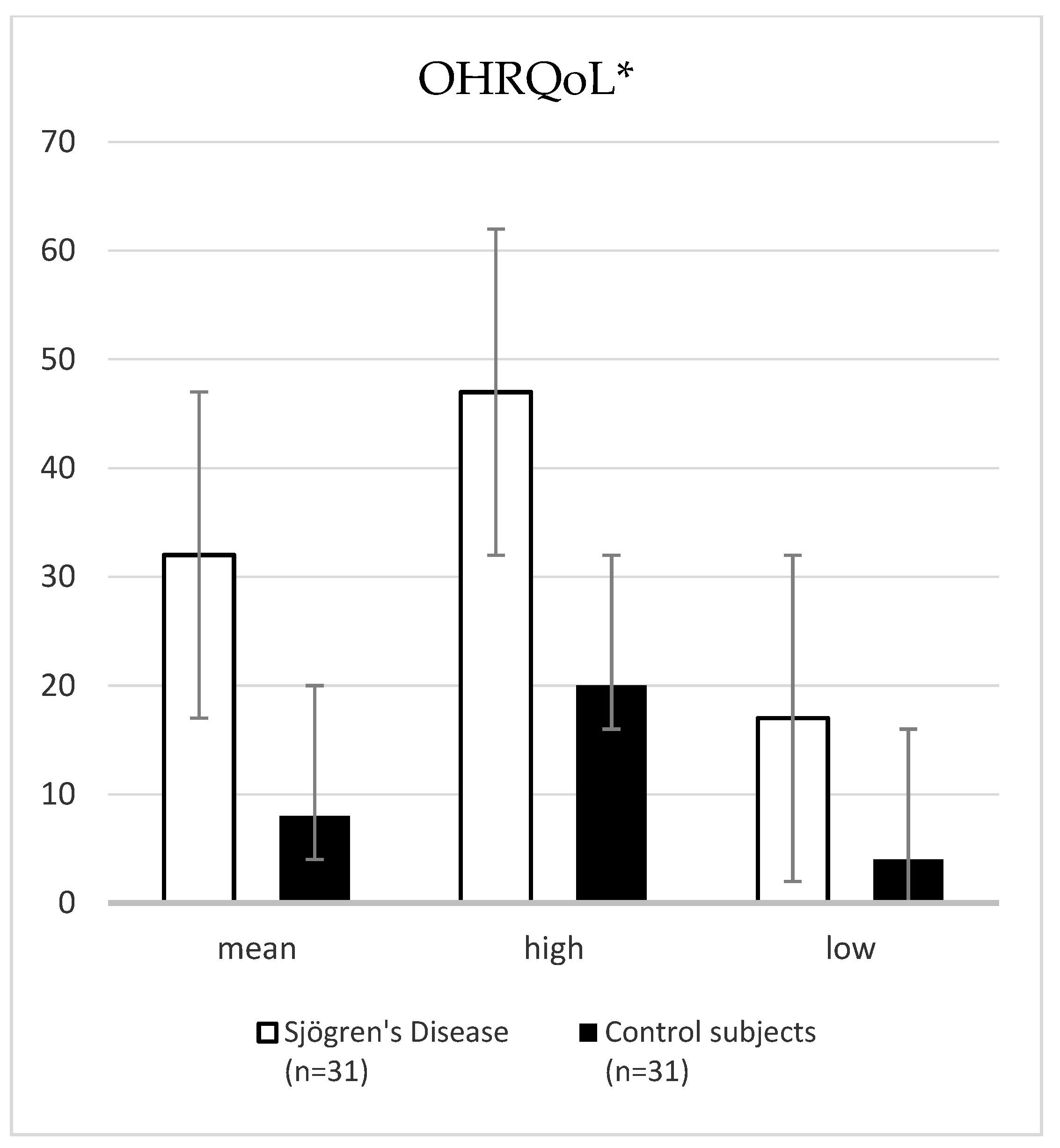
3.2. Oral Status and OHRQoL
3.3. ESSDAI, ESSPRI, 6-Items-VAS-SS, Profile of Fatigue
3.4. Serum Antibody Reactivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Dryness (0 1 2 3 4 5 6 7 8 9 10)
- Arthralgias (0 1 2 3 4 5 6 7 8 9 10)
- Myalgias (0 1 2 3 4 5 6 7 8 9 10)
- Paresthesias (0 1 2 3 4 5 6 7 8 9 10)
- Somatic fatigue (0 1 2 3 4 5 6 7 8 9 10)
- Mental fatigue (0 1 2 3 4 5 6 7 8 9 10)
References
- López-Pintor, R.M.; Fernández Castro, M.; Hernández, G. Oral Involvement in Patients with Primary Sjögren’s Syndrome. Multidisciplinary Care by Dentists and Rheumatologists. Reumatol. Clín. 2015, 11, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Stefanski, A.-L.; Tomiak, C.; Pleyer, U.; Dietrich, T.; Burmester, G.R.; Dörner, T. The Diagnosis and Treatment of Sjögren’s Syndrome. Dtsch. Arztebl. Int. 2017, 114, 354–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negrini, S.; Emmi, G.; Greco, M.; Borro, M.; Sardanelli, F.; Murdaca, G.; Indiveri, F.; Puppo, F. Sjögren’s Syndrome: A Systemic Autoimmune Disease. Clin. Exp. Med. 2022, 22, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-Y.; Wu, C.-Y.; Chen, M.-H.; Huang, H.-Y.; Chen, Y.-H.; Tsao, Y.-P.; Lai, Y.-L.; Lee, S.-Y. Periodontal Conditions in Patients with Sjögren’s Syndrome: A Meta-Analysis. J. Dent. Sci. 2021, 16, 1222–1232. [Google Scholar] [CrossRef] [PubMed]
- Lendrem, D.; Mitchell, S.; McMeekin, P.; Bowman, S.; Price, E.; Pease, C.T.; Emery, P.; Andrews, J.; Lanyon, P.; Hunter, J.; et al. UK primary Sjögren’s Syndrome Registry. Health-Related Utility Values of Patients with Primary Sjögren’s Syndrome and Its Predictors. Ann. Rheum. Dis. 2014, 73, 1362–1368. [Google Scholar] [CrossRef]
- Parrini, S.; Chisci, G.; Leoncini, S.; Signorini, C.; Volpi, N.; Capuano, A.; Ciccoli, L.; De Felice, C. F2-Isoprostanes in soft oral tissues and degree of oral disability after mandibular third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 344–349. [Google Scholar] [CrossRef]
- Chisci, G.; De Felice, C.; Parrini, S.; Signorini, C.; Leoncini, S.; Ciccoli, L.; Volpi, N.; Capuano, A. The role of preoperative oxidative stress and mandibular third molar postoperative outcome. Int. J. Oral Maxillofac. Surg. 2013, 42, 1499–1500. [Google Scholar] [CrossRef]
- Bennadi, D.; Reddy, C.V.K. Oral health related quality of life. J. Int. Soc. Prev. Community Dent. 2013, 3, 1–6. [Google Scholar] [CrossRef]
- Rener–Sitar, K.; Petričević, N.; Čelebić, A.; Marion, L. Psychometric Properties of Croatian and Slovenian Short Form of Oral Health Impact Profile Questionnaires. Croat. Med. J. 2008, 49, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Lόpez-Jornet, P.; Camacho-Alonso, F. Quality of life in patients with Sjögren’s syndrome and sicca complex. J. Oral Rehabil. 2008, 35, 875–881. [Google Scholar] [CrossRef]
- Seror, R.; Ravaud, P.; Bowman, S.J. EULAR Sjogren’s Syndrome Disease Activity Index: Development of a Consensus Systemic Disease Activity Index for Primary Sjogren’s Syndrome. Ann. Rheum. Dis. 2010, 69, 1103–1109. [Google Scholar] [CrossRef]
- Seror, R.; Ravaud, P.; Mariette, X.; Bootsma, H.; Theander, E.; Hansen, A.; Ramos-Casals, M.; Dörner, T.; Bombardieri, S.; Hachulla, E.; et al. EULAR Sjögren’s Task Force. EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI): Development of a Consensus Patient Index for Primary Sjögren’s Syndrome. Ann. Rheum. Dis. 2011, 70, 968–972. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R. ACR-EULAR Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involoving Three International Patient Cohorts. Arthritis Rheumatol. 2016, 69, 35–45. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Cox, S.C.; Walker, D.M. Establishing a Normal Range for Mouth Opening: Its Use in Screening for Oral Submucous Fibrosis. Br. J. Oral Maxillofac. Surg. 1997, 35, 40–42. [Google Scholar] [CrossRef]
- Oral Health Database. Available online: www.mah.se/CAPP/Methods-and-Indices/ (accessed on 13 March 2022).
- Petersen, P.E. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century-the Approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31 (Suppl. 1), 3–24. [Google Scholar]
- World Health Organization. Oral Health Surveys-Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Page, R.C.; Eke, P.I. Case Definitions for Use in Population-Based Surveillance of Periodontitis. J. Periodontol. 2007, 78 (Suppl. 7), 1387–1399. [Google Scholar] [CrossRef] [Green Version]
- Savage, A.; Eaton, K.A.; Moles, D.R.; Needleman, I. A Systematic Review of Definitions of Periodontitis and Methods That Have Been Used to Identify This Disease. J. Clin. Periodontol. 2009, 36, 458–467. [Google Scholar] [CrossRef]
- Petričević, N.; Čelebić, A.; Papić, M.; Rener-Sitar, K. The Croatian Version of the Oral Helath Impact Profile Questionnaire. Coll. Antropol. 2009, 33, 841–847. [Google Scholar]
- Pai, S.; Ghezzi, E.M.; Ship, J.A. Development of a Visual Analogue Scale Questionnaire for Subjective Assessment of Salivary Dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 311–316. [Google Scholar] [CrossRef]
- Xin, W.; Leung, C.M.; Lo, E.; Mok, M.Y.; Leung, M.H. Sicca Symptoms, Oral Health Conditions, Salivary Flow and Oral Candidia in Sjögren’s Syndrome Patients. Int. J. Environ. Res. Public Health 2020, 17, 3625. [Google Scholar] [CrossRef] [PubMed]
- Maarse, F.; Jager, D.H.J.; Alterch, S.; Korfage, A.; Forouzanfar, T.; Vissink, A.; Brand, H.S. Sjögren’s Syndrome Is Not a Risk Factor for Periodontal Disease: A Systematic Review. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 118), 225–233. [Google Scholar] [PubMed]
- Christensen, L.B.; Petersen, P.E.; Thorn, J.J.; Schiødt, M. Dental Caries and Dental Health Behavior of Patients with Primary Sjögren Syndrome. Acta Odontol. Scand. 2001, 59, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Márton, K.; Boros, I.; Varga, G.; Zelles, T.; Fejérdy, P.; Zeher, M.; Nagy, G. Evaluation of Palatal Saliva Flow Rate and Oral Manifestations in Patients with Sjögren’s Syndrome. Oral Dis. 2006, 12, 480–486. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Tseng, C.-F.; Liu, J.-M.; Chuang, H.-C.; Lei, W.-T.; Liu, L.Y.-M.; Yu, Y.-C.; Hsu, R.-J. Association between Periodontal Disease and Subsequent Sjögren’s Syndrome: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 771. [Google Scholar] [CrossRef] [Green Version]
- de Goés Soares, L.; Rocha, R.L.; Bagordakis, E.; Galvão, E.L.; Douglas-de-Oliveira, D.W.; Falci, S.G.M. Relationship between Sjögren Syndrome and Periodontal Status: A Systematic Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 223–231. [Google Scholar] [CrossRef]
- Lugonja, B.; Yeo, L.; Milward, M.R.; Smith, D.; Dietrich, T.; Chapple, I.L.C.; Rauz, S.; Williams, G.P.; Barone, F.; de Pablo, P.; et al. Periodontitis Prevalence and Serum Antibody Reactivity to Periodontal Bacteria in Primary Sjögren’s Syndrome: A Pilot Study. J. Clin. Periodontol. 2016, 43, 26–33. [Google Scholar] [CrossRef]
- Jorkjend, L.; Johansson, A.; Johansson, A.-K.; Bergenholtz, A. Periodontitis, Caries and Salivary Factors in Sjögren’s Syndrome Patients Compared to Sex- and Age-Matched Controls: SECONDARY SJÖGREN’S SYNDROME. J. Oral. Rehabil. 2003, 30, 369–378. [Google Scholar] [CrossRef]
- Ambrósio, L.M.B.; Rovai, E.d.S.; França, B.N.d.; Balzarini, D.A.; Abreu, I.S.; Lopes, S.B.B.; Nunes, T.B.; Lourenço, S.V.; Pasoto, S.G.; Saraiva, L.; et al. Effects of Periodontal Treatment on Primary Sjȫgren’s Syndrome Symptoms. Braz. Oral Res. 2017, 31, e8. [Google Scholar] [CrossRef] [Green Version]
- Azuma, N.; Katada, Y.; Yoshikawa, T.; Yokoyama, Y.; Nishioka, A.; Sekiguchi, M.; Kitano, M.; Kitano, S.; Sano, H.; Matsui, K. Evaluation of Changes in Oral Health-Related Quality of Life over Time in Patients with Sjögren’s Syndrome. Mod. Rheumatol. 2021, 31, 669–677. [Google Scholar] [CrossRef]
- Gobeljić, M.Š.; Milić, V.; Pejnovic, N.; Damjanov, N. Chemosensory Dysfunction, Oral Disorders and Oral Health-Related Quality of Life in Patients with Primary Sjögren’s Syndrome: Comparative Cross-Sectional Study; Research Square: Durham, NC, USA, 2020. [Google Scholar] [CrossRef]
- Schmalz, G.; Patschan, S.; Patschan, D.; Ziebolz, D. Oral-Health-Related Quality of Life in Adult Patients with Rheumatic Diseases—A Systematic Review. J. Clin. Med. 2020, 9, 1172. [Google Scholar] [CrossRef] [Green Version]
- Rusthen, S.; Young, A.; Herlofson, B.B.; Aqrawi, L.A.; Rykke, M.; Hove, L.H.; Palm, Ø.; Jensen, J.L.; Singh, P.B. Oral Disorders, Saliva Secretion, and Oral Health-Related Quality of Life in Patients with Primary Sjögren’s Syndrome. Eur. J. Oral Sci. 2017, 125, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Wen, S.; Beltrán, V.; Chaparro, A.; Espinoza, F.; Riedemann, J.P. Association between chronic periodontitis and rheumatoid arthritis. A systematic review. Rev. Med. Chil. 2019, 147, 762–775. [Google Scholar] [CrossRef] [Green Version]
- González-Febles, J.; Sanz, M. Periodontitis and Rheumatoid Arthritis: What Have We Learned about Their Connection and Their Treatment? Periodontol. 2000 2021, 87, 181–203. [Google Scholar] [CrossRef]
- Vigu, A.; Stanciu, D.; Lotrean, L.M.; Campian, R.S. Complex Interrelations between Self-Reported Oral Health Attitudes and Behaviors, the Oral Health Status, and Oral Health-Related Quality of Life. Patient Prefer. Adherence 2018, 12, 539–549. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Sjögren’s Disease (n = 31) | Control Subjects (n = 31) | Z (p-Value) | |
|---|---|---|---|
| Mean (IQR) ** | Mean (IQR) ** | ||
| Disease duration | 5.50 (2.50–9.00) | ||
| UWSFR (mL/min) | 0.20 (0.00–3.00) | 0.90 (4.00–5.50) | −5.74 (<0.001) * |
| SWSFR (mL/min) | 0.56 (0.60–4.60) | 1.64 (7.10–9.20) | −6.17 (<0.001) * |
| pH values | 6.00 (5.50–6.50) | 7.00 (6.40–7.00) | −3.77 (<0.001) * |
| ESSDAI | 10.00 (7.00–14.00) | ||
| ESSPRI | 22.00 (15.00–25.00) | ||
| 6-items-VAS-SS | 35.00 (28.00–42.00) | ||
| Profile of Fatigue (VAS) | 28.00 (22.00–36.00) |
| Sjögren’s Disease (n = 31) | Control Subjects (n = 31) | t (p-Value) | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Interincisal distance (mm) | 43.80 (0.38) | 47.60 (0.50) | −3.09 (0.003) * |
| DMFT index | 23.74 (7.28) | 20.77 (5.73) | 1.78 (0.080) * |
| ESSDAI | ESSPRI | 6-Items-VAS-SS | Profile of Fatigue | ||
|---|---|---|---|---|---|
| Disease duration | rho | 0.277 | 0.185 | 0.262 | 0.315 |
| p | 0.15 | 0.35 | 0.18 | 0.10 | |
| UWSFR (mL/min) | rho | 0.708 ** | 0.650 ** | −0.599 ** | −0.630 ** |
| p | <0.001 | <0.001 | <0.001 | <0.001 | |
| SWSFR (mL/min) | rho | 0.743 ** | 0.703 ** | −0.664 ** | −0.700 ** |
| p | <0.001 | <0.001 | <0.001 | <0.001 | |
| pH values | rho | −0.406 * | −0.441 * | −0.501 ** | −0.413 * |
| p | 0.02 | 0.013 | 0.004 | 0.02 | |
| Total OHIP-49 score | rho | 0.949 ** | 0.887 ** | 0.936 ** | 0.978 ** |
| p | <0.001 | <0.001 | <0.001 | <0.001 | |
| Interincisal distance (mm) | rho | 0.048 | 0.009 | 0.038 | 0.105 |
| p | 0.83 | 0.97 | 0.86 | 0.62 | |
| DMFT index | rho | 0.342 | 0.219 | 0.335 | 0.309 |
| p | 0.06 | 0.24 | 0.07 | 0.09 | |
| Periodontitis | rho | 0.017 | 0.074 | 0.034 | 0.017 |
| p | 0.93 | 0.70 | 0.86 | 0.93 |
| The Salivary Glands Can Produce Saliva: | The Salivary Glands Cannot Produce Saliva: |
|---|---|
|
|
| Oral hygiene instructions and dietary guidelines | |
| |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glavina, A.; Božić, I.; Parat, K.; Perković, D.; Biočina-Lukenda, D.; Martinović Kaliterna, D.; Radić, M. The Croatian Primary Sjögren’s Disease Oral Health Study: Oral Status and Oral Health-Related Quality of Life. J. Clin. Med. 2023, 12, 4804. https://doi.org/10.3390/jcm12144804
Glavina A, Božić I, Parat K, Perković D, Biočina-Lukenda D, Martinović Kaliterna D, Radić M. The Croatian Primary Sjögren’s Disease Oral Health Study: Oral Status and Oral Health-Related Quality of Life. Journal of Clinical Medicine. 2023; 12(14):4804. https://doi.org/10.3390/jcm12144804
Chicago/Turabian StyleGlavina, Ana, Ivona Božić, Katica Parat, Dijana Perković, Dolores Biočina-Lukenda, Dušanka Martinović Kaliterna, and Mislav Radić. 2023. "The Croatian Primary Sjögren’s Disease Oral Health Study: Oral Status and Oral Health-Related Quality of Life" Journal of Clinical Medicine 12, no. 14: 4804. https://doi.org/10.3390/jcm12144804