
The Association of Infection with Delirium in the Post-Operative Period after Elective CABG Surgery

Abstract
:1. Introduction
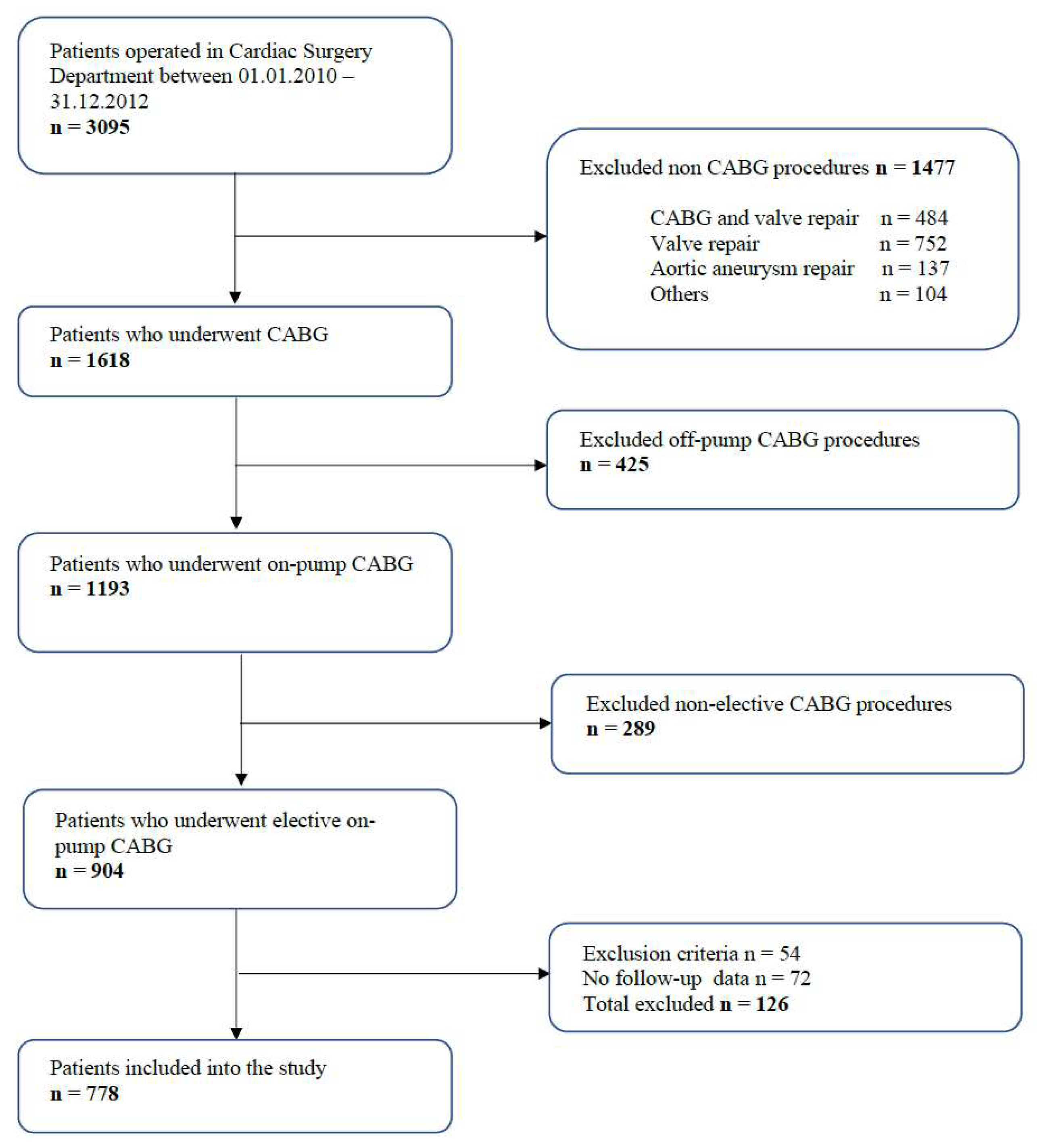
2. Materials and Methods
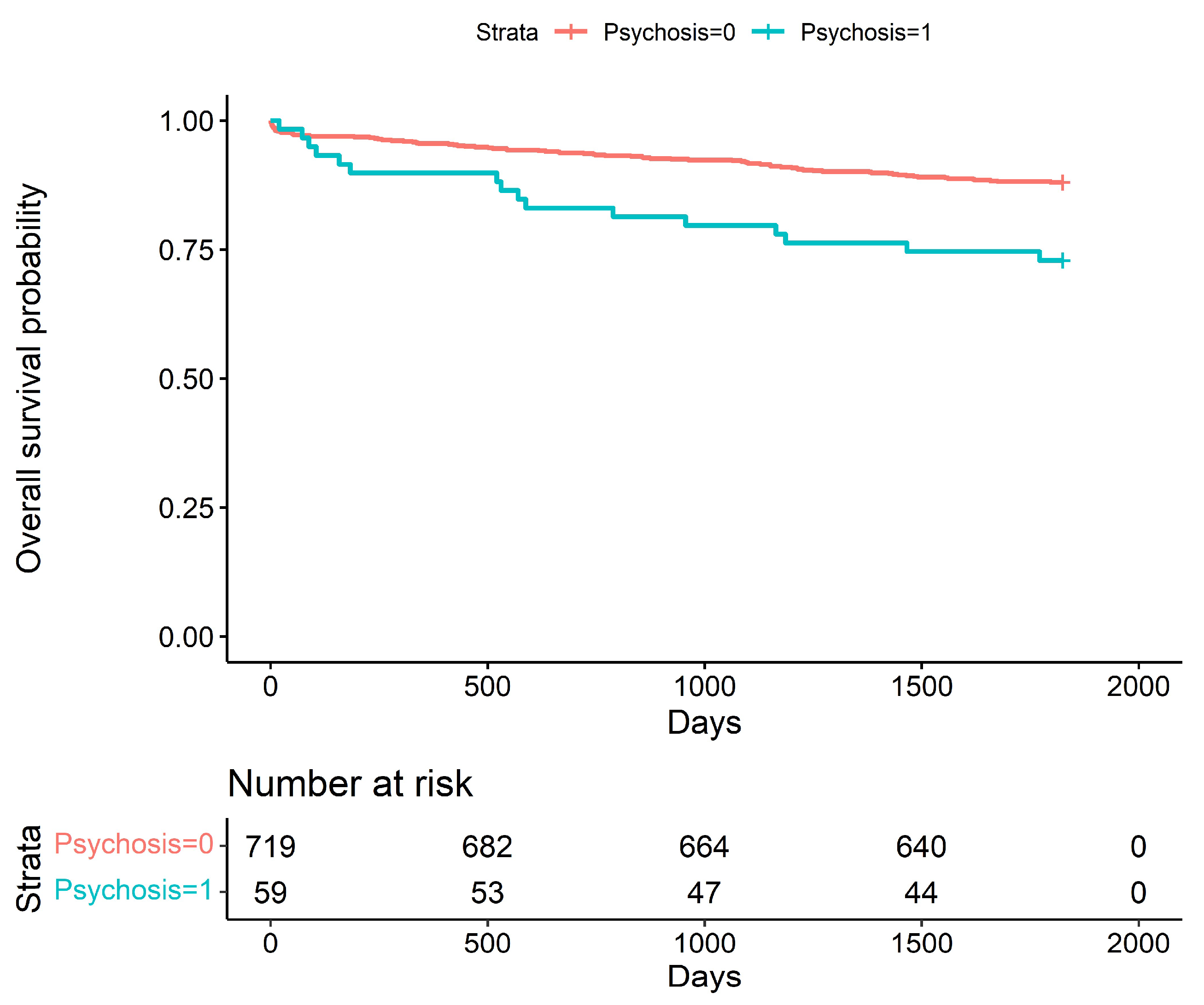
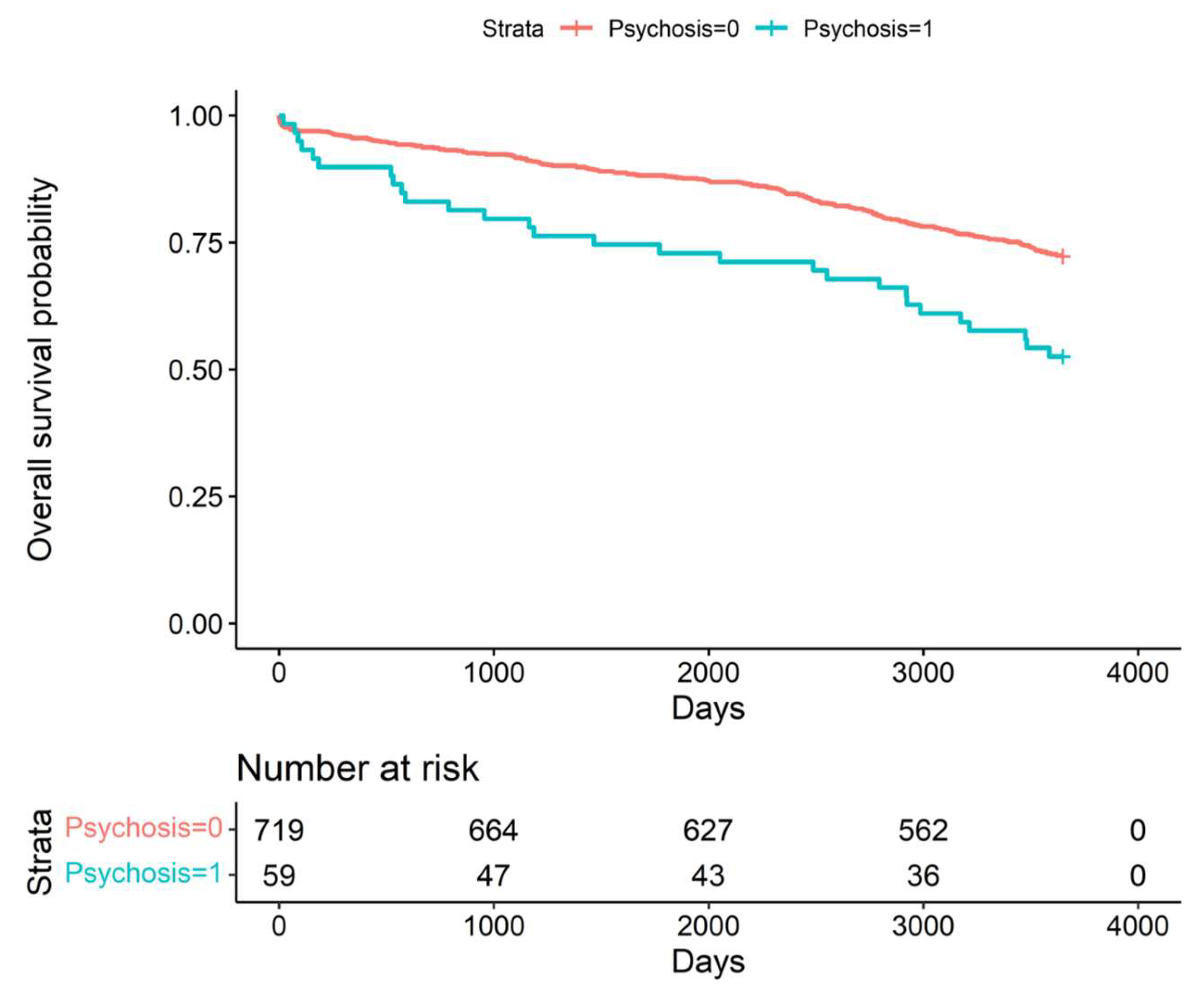
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; AlKatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S. Lootah SNAH. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R.; Shepard, D.; VanderZanden, A.; Naghavi, M.; Roth, G.A.; Huffman, M.D.; et al. Mortality From Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Smulter, N.; Lingehall, H.C.; Gustafson, Y.; Olofsson, B.; Engström, K.G. Delirium after cardiac surgery: Incidence and risk factors. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 790–796. [Google Scholar] [CrossRef] [Green Version]
- Sadlonova, M.; Vogelgsang, J.; Lange, C.; Günther, I.; Wiesent, A.; Eberhard, C.; Ehrentraut, J.; Kirsch, M.; Hansen, N.; Esselmann, H.; et al. Identification of risk factors for delirium, cognitive decline, and dementia after cardiac surgery (FINDERI-find delirium risk factors): A study protocol of a prospective observational study. BMC Cardiovasc. Disord. 2022, 22, 299. [Google Scholar] [CrossRef]
- Rose, L.; Burry, L.; Agar, M.; Blackwood, B.; Campbell, N.L.; Clarke, M.; Devlin, J.W.; Lee, J.; Marshall, J.C.; Needham, D.M.; et al. A core outcome set for studies evaluating interventions to prevent and/or treat delirium for adults requiring an acute care hospital admission: An international key stakeholder informed consensus study. BMC Med. 2021, 19, 143. [Google Scholar] [CrossRef] [PubMed]
- Kassie, G.M.; Nguyen, T.A.; Ellett, L.M.K.; Pratt, N.L.; Roughead, E.E. Preoperative medication use and postoperative delirium: A systematic review. BMC. Geriatr. 2017, 17, 298. [Google Scholar] [CrossRef] [Green Version]
- John, M.; Ely, E.W.; Halfkann, D.; Schoen, J.; Sedemund-Adib, B.; Klotz, S.; Radtke, F.; Stehr, S.; Hueppe, M. Acetylcholinesterase and butyrylcholinesterase in cardiosurgical patients with postoperative delirium. J. Intensive. Care 2017, 5, 29. [Google Scholar] [CrossRef]
- Aiello, G.; Cuocina, M.; La Via, L.; Messina, S.; Attaguile, G.A.; Cantarella, G.; Sanfilippo, F.; Bernardini, R. Melatonin or Ramelteon for Delirium Prevention in the Intensive Care Unit: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 435. [Google Scholar] [CrossRef]
- Alvarez, E.A.; Rojas, V.A.; Caipo, L.I.; Galaz, M.M.; Ponce, D.P.; Gutierrez, R.G.; Salech, F.; Tobar, E.; Reyes, F.I.; Vergara, R.C.; et al. Non-pharmacological prevention of postoperative delirium by occupational therapy teams: A randomized clinical trial. Front. Med. 2023, 10, 1099594. [Google Scholar] [CrossRef]
- Pagad, S.; Somagutta, M.R.; May, V.; Arnold, A.A.; Nanthakumaran, S.; Sridharan, S.; Malik, B.H. Delirium in Cardiac Intensive Care Unit. Cureus 2020, 12, e10096. [Google Scholar] [CrossRef]
- Xu, Y.; Ma, Q.; Du, H.; Yang, C.; Lin, G. Postoperative Delirium in Neurosurgical Patients: Recent Insights into the Pathogenesis. Brain Sci. 2022, 12, 1371. [Google Scholar] [CrossRef] [PubMed]
- Fatehi Hassanabad, A.; Bahrami, N.; Novick, R.J.; Ali, I.S. Delirium and depression in cardiac surgery: A comprehensive review of risk factors, pathophysiology, and management. J. Card. Surg. 2021, 36, 2876–2889. [Google Scholar] [CrossRef] [PubMed]
- Deininger, M.M.; Schnitzler, S.; Benstoem, C.; Simon, T.P.; Marx, G.; Panagiotidis, D.; Ziles, D.; Schnoering, H.; Karasimos, E.; Breuer, T. Standardized pharmacological management of delirium after on-pump cardiac surgery reduces ICU stay and ventilation in a retrospective pre-post study. Sci. Rep. 2023, 13, 3741. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Zhang, X.; Xu, S.; Peng, Y.; Li, S.; Huang, X.; Chen, L.; Lin, Y. Outcomes of postoperative delirium in patients undergoing cardiac surgery: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 884144. [Google Scholar] [CrossRef]
- Satomoto, M. Predicting Postoperative Emergence Delirium From the Heart Rate Variability of Patients Undergoing Elective Cardiac Surgery. Cureus 2023, 15, e34613. [Google Scholar] [CrossRef]
- Sari, S.; Brooker, J.; Montalvo-Campana, M.; Shehata, P.; Pu, X.; Insler, S.; Ruetzler, K.; Troianos, C.A.; Turan, A. The association of hemoglobin with postoperative delirium and atrial fibrillation after cardiac surgery: A retrospective sub-study. Braz. J. Anesthesiol. 2023, in press. [Google Scholar] [CrossRef]
- Chen, H.; Mo, L.; Hu, H.; Ou, Y.; Luo, J. Risk factors of postoperative delirium after cardiac surgery: A meta-analysis. J. Cardiothorac. Surg. 2021, 16, 113. [Google Scholar] [CrossRef]
- Ma, X.; Chu, H.; Han, K.; Shao, Q.; Yu, Y.; Jia, S.; Wang, D.; Wang, Z.; Zhou, Y. Postoperative delirium after transcatheter aortic valve replacement: An updated systematic review and meta-analysis. J. Am. Geriatr. Soc. 2023, 71, 646–660. [Google Scholar] [CrossRef]
- Andrási, T.B.; Talipov, I.; Dinges, G.; Arndt, C.; Rastan, A.J. Risk factors for postoperative delirium after cardiac surgical procedures with cardioplegic arrest. Eur. J. Cardiothorac. Surg. 2022, 62, ezab570. [Google Scholar] [CrossRef]
- Kuswardhani, R.A.T.; Sugi, Y.S. Factors Related to the Severity of Delirium in the Elderly Patients With Infection. Gerontol. Geriatr. Med. 2017, 3, 2333721417739188. [Google Scholar] [CrossRef]
- Dutta, C.; Pasha, K.; Paul, S.; Abbas, M.S.; Nassar, S.T.; Tasha, T.; Desai, A.; Bajgain, A.; Ali, A.; Mohammed, L. Urinary Tract Infection Induced Delirium in Elderly Patients: A Systematic Review. Cureus 2022, 14, e32321. [Google Scholar] [CrossRef] [PubMed]
- Krinitski, D.; Kasina, R.; Klöppel, S.; Lenouvel, E. Associations of delirium with urinary tract infections and asymptomatic bacteriuria in adults aged 65 and older: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2021, 69, 3312–3323. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.; Bowden, A.; Sundvall, P.-D.; Gunnarsson, R. The scientific evidence for a potential link between confusion and urinary tract infection in the elderly is still confusing—A systematic literature review. BMC Geriatr. 2019, 19, 32. [Google Scholar] [CrossRef] [Green Version]
- Spiropoulou, E.; Samanidis, G.; Kanakis, M.; Nenekidis, I. Risk Factors for Acute Postoperative Delirium in Cardiac Surgery Patients >65 Years Old. J. Pers. Med. 2022, 12, 1529. [Google Scholar] [CrossRef]
- Archbald-Pannone, L.R.; McMurry, T.L.; Guerrant, R.L.; Warren, C.A. Delirium and other clinical factors with Clostridium difficile infection that predict mortality in hospitalized patients. Am. J. Infect. Control. 2015, 43, 690–693. [Google Scholar] [CrossRef] [Green Version]
- de la Varga-Martínez, O.; Gutiérrez-Bustillo, R.; Muñoz-Moreno, M.F.; López-Herrero, R.; Gómez-Sánchez, E.; Tamayo, E. Postoperative delirium: An independent risk factor for poorer quality of life with long-term cognitive and functional decline after cardiac surgery. J. Clin. Anesth. 2023, 85, 111030. [Google Scholar] [CrossRef]
- Dzahini, O.; Singh, N.; Taylor, D.; Haddad, P.M. Antipsychotic drug use and pneumonia: Systematic review and meta-analysis. J. Psychopharmacol. 2018, 32, 1167–1181. [Google Scholar] [CrossRef]
- Lewin, J.; Maconochie, I. Capillary refill time in adults. Emerg. Med. J. 2008, 25, 325–326. [Google Scholar] [CrossRef] [PubMed]
- La Via, L.; Sanfilippo, F.; Continella, C.; Triolo, T.; Messina, A.; Robba, C.; Astuto, M.; Hernandez, G.; Noto, A. Agreement between Capillary Refill Time measured at Finger and Earlobe sites in different positions: A pilot prospective study on healthy volunteers. BMC Anesthesiol. 2023, 23, 30. [Google Scholar] [CrossRef]
- Yamamoto, M.; Doi, K.; Hayase, N.; Asada, T.; Akamatsu, N.; Kaneko, J.; Hasegawa, K.; Morimura, N. Pulse oximetry-based capillary refilling evaluation predicts postoperative outcomes in liver transplantation: A prospective observational cohort study. BMC Anesthesiol. 2020, 20, 251. [Google Scholar] [CrossRef] [PubMed]
- Fahmei, T.B.; El-Shazly, S.; Ibrahim, H.S. Factors Associated with Postoperative Delirium among Geriatric Patients. Alex. Sci. Nurs. J. 2014, 16, 145–160. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Delirium (−) n = 719 | Delirium (+) n = 59 | p |
|---|---|---|---|
| Female (n. %) | 170/719 (24%) | 17/59 (29%) | 0.9999 |
| Age (years. mean ± SD) | 64 (9) | 70 (10) | 0.0002 |
| Weight (kg. mean ± SD) | 81 (13) | 78 (11) | 0.3110 |
| BMI | 29.3 (8.4) | 28.8 (3.6) | 0.6530 |
| Smoking (n. %) | 312/719 (11) | 14 (59) | 0.0602 |
| ES (mean ± SD) | 3.77 (2.69) | 5.32 (2.41) | <0.0001 |
| ESlog (mean ± SD) | 4.7 (5.3) | 6.7 (4.7) | <0.0001 |
| LVEF (%. mean ± SD) | 50 (11) | 48 (11) | 0.5801 |
| NYHA functional class (n. %) | 0.9999 | ||
| 1 | 3/706 (0.4%) | 1/59 (1.7%) | |
| 2 | 138/706 (20%) | 10/59 (17%) | |
| 3 | 400/706 (57%) | 36/59 (61%) | |
| 4 | 165/706 (23%) | 12/59 (20%) | |
| Insulin intake (n. %) | 101/718 (14%) | 10/59 (17%) | 0.7277 |
| HbA1c (%, mean ± SD) | 2.11 (3.25) | 3.18 (3.80) | 0.1557 |
| Hb (mg/dL, mean ± SD) | 8.45 (0.79) | 8.17 (0.76) | 0.0711 |
| Hct (%, mean ± SD) | 0.41 (0.04) | 0.39 (0.04) | 0.1577 |
| PLT (mean ± SD) | 246 (66) | 261 (72) | 0.4609 |
| Serum creatinine level mg/dL (mean ± SD) | 0.95 (0.50) | 1.07 (1.08) | 0.5478 |
| Parameter | Delirium (−) n = 719 | Delirium (+) n = 59 | p |
|---|---|---|---|
| Insulin dependent diabetes (n. %) | 8/719 (1.1%) | 0/59 (0%) | 0.9999 |
| Insulin non-dependent diabetes (n. %) | 225/719 (31%) | 26/59 (44%) | 0.3664 |
| Prior stroke (n. %) | 32/719 (4.5%) | 5/59 (8.5%) | 0.9999 |
| TIA (n. %) | 6/719 (0.8%) | 0/59 (0%) | 0.9999 |
| Hypertension (n. %) | 552/719 (77%) | 52/59 (88%) | 0.2622 |
| Myocardial infarction (n. %) | 245/718 (34%) | 19/59 (32%) | 0.9999 |
| Atrial fibrillation (n. %) | 23/719 (3.2%) | 3/59 (5.1%) | 0.9999 |
| Hypercholesterolemia (n. %) | 57/719 (7.9%) | 3/59 (5.1%) | 0.9999 |
| Dyslipidemia (n. %) | 66/719 (9.2%) | 2/59 (3.4%) | 0.8493 |
| Peripheral arterial disease (n. %) | 77/719 (11%) | 10/59 (17%) | 0.8493 |
| Renal failure (n. %) | 31/719 (4.3%) | 3/59 (5.1%) | 0.9999 |
| Autoimmune diseases (n. %) | 14/719 (1.9%) | 1/59 (1.7%) | 0.9999 |
| Parameter | Delirium (−) n = 719 | Delirium (+) n = 59 | p |
|---|---|---|---|
| Duration of surgery (min. mean ± SD) | 152 (50) | 150 (22) | 0.9973 |
| Duration of CPB (min. mean ± SD) | 50 (15) | 49 (13) | 0.9973 |
| CPB fluid balance (mL. mean ± SD) | 572 (613) | 498 (749) | 0.7277 |
| IntraoperativeUF (mL. mean ± SD) | 148 (469) | 351 (671) | 0.0215 |
| LVEF day after surgery % | 52 (10) | 49 (11) | 0.1503 |
| Day 1 fluid balance (mL. mean ± SD) | −1105 (1060) | −807 (1109) | 0.2682 |
| Day 2 fluid balance (mL. mean ± SD) | −179 (849) | −115 (874) | 0.5801 |
| Overall fluid balance (mL. mean ± SD) | −1255 (1429) | −928 (1291) | 0.1557 |
| Intra-aortic balloon pump (n. %) | 4/716 (0.6%) | 0/59 (0%) | 0.9999 |
| Milrinone (n. %) | 17/704 (2.4%) | 3/58 (5.2%) | 0.9999 |
| Postoperative drainage (mL. mean ± SD) | 545 (335) | 559 (397) | 0.9973 |
| Postoperative Hb (mg/dL, mean ± SD) | 6.72 (0.81) | 6.63 (0.75) | 0.5801 |
| Postoperative Hct (%, mean ± SD) | 0.34 (0.05) | 0.32 (0.04) | 0.4609 |
| Postoperative PLT (,mean ± SD) | 189 (54) | 198 (51) | 0.4609 |
| Postoperative Cr level mg/dL (mean ± SD) | 1.03 (0.66) | 1.14 (0.61) | 0.0711 |
| RBC (mL. mean ± SD) | 138 (288) | 174 (296) | 0.5478 |
| PLT (mL. n. %) | 0.9973 | ||
| 0 | 599/717 (84%) | 48/59 (81%) | |
| 200 | 1/717 (0.1%) | 0/59 (0%) | |
| 250 | 60/717 (8.4%) | 4/59 (6.8%) | |
| 300 | 47/717 (6.6%) | 7/59 (12%) | |
| 500 | 2/717 (0.3%) | 0/59 (0%) | |
| 550 | 5/717 (0.7%) | 0/59 (0%) | |
| 600 | 3/717 (0.4%) | 0/59 (0%) | |
| CK-MB after 6 h | 38 (25) | 42 (32) | 0.6933 |
| CK-MB after 12 h | 44 (46) | 54 (49) | 0.4609 |
| CK-MB after 24 h | 48 (63) | 54 (47) | 0.4675 |
| Parameter | Delirium (−) n = 719 | Delirium (+) n = 59 | p |
|---|---|---|---|
| Postoperative TIA (n. %) | 4/719 (0.6%) | 1/59 (1.7%) | 0.9999 |
| Postoperative MI (n. %) | 12/719 (1.7%) | 1/59 (1.7%) | 0.9999 |
| Postoperative stroke (n. %) | 6/719 (0.8%) | 1/59 (1.7%) | 0.9999 |
| Postoperative AF (n. %) | 161/719 (22%) | 16/59 (27%) | 0.9999 |
| Infection (n. %) | 53/719 (7.4%) | 13/58 (22%) | 0.0037 |
| Infection source (n. %) | 0.0025 | ||
| 0 | 666/719 (93%) | 45/58 (78%) | |
| BSI | 14/719 (1.9%) | 1/58 (1.7%) | |
| SSI sternal | 10/719 (1.4%) | 5/58 (8.6%) | |
| SSI leg | 2/719 (0.3%) | 1/58 (1.7%) | |
| Pneumonia | 27/719 (3.8%) | 6/58 (10%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zukowska, A.; Kaczmarczyk, M.; Listewnik, M.; Zukowski, M. The Association of Infection with Delirium in the Post-Operative Period after Elective CABG Surgery. J. Clin. Med. 2023, 12, 4736. https://doi.org/10.3390/jcm12144736
Zukowska A, Kaczmarczyk M, Listewnik M, Zukowski M. The Association of Infection with Delirium in the Post-Operative Period after Elective CABG Surgery. Journal of Clinical Medicine. 2023; 12(14):4736. https://doi.org/10.3390/jcm12144736
Chicago/Turabian StyleZukowska, Agnieszka, Mariusz Kaczmarczyk, Mariusz Listewnik, and Maciej Zukowski. 2023. "The Association of Infection with Delirium in the Post-Operative Period after Elective CABG Surgery" Journal of Clinical Medicine 12, no. 14: 4736. https://doi.org/10.3390/jcm12144736