
Long-Term Prognosis of Patients with Polypoidal Choroidal Vasculopathy Treated with Photodynamic Therapy
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Patients
2.3. Research and Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Additional Treatments
3.3. Changes in BCVA and CRT
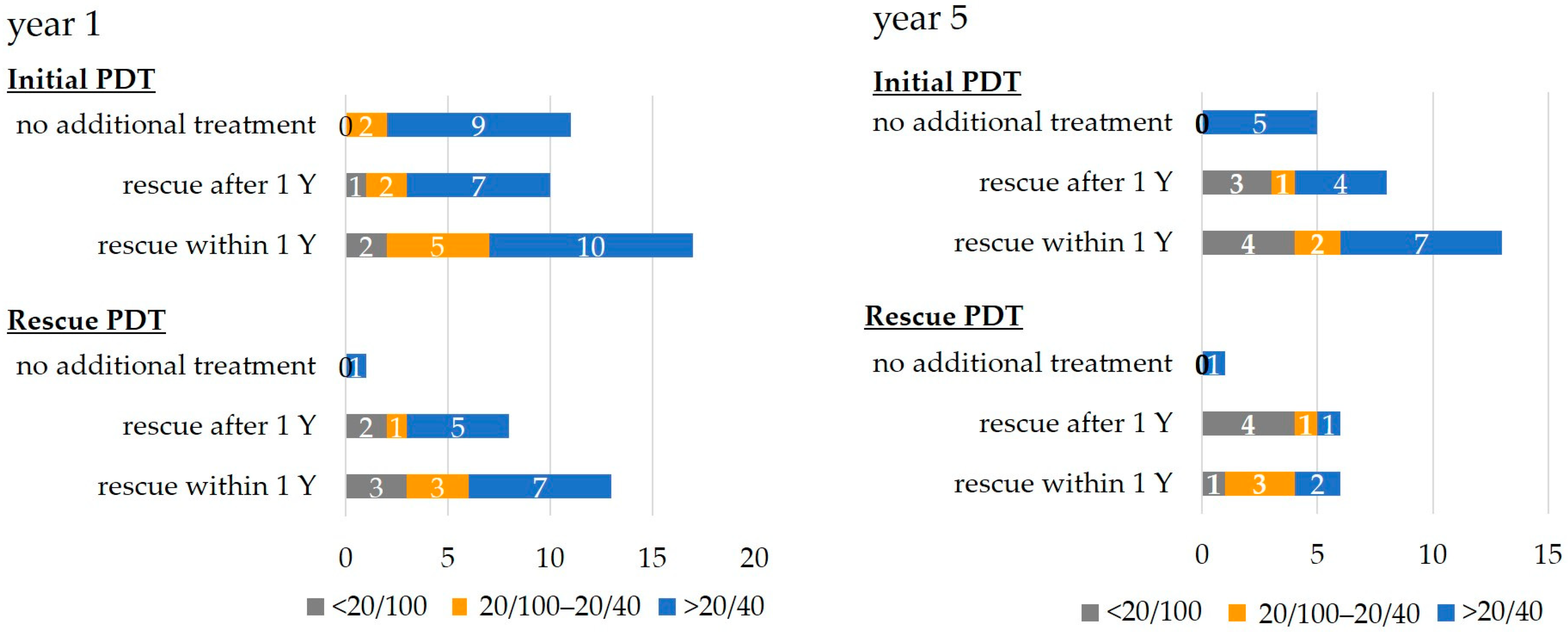
3.4. Distribution of Final BCVAs
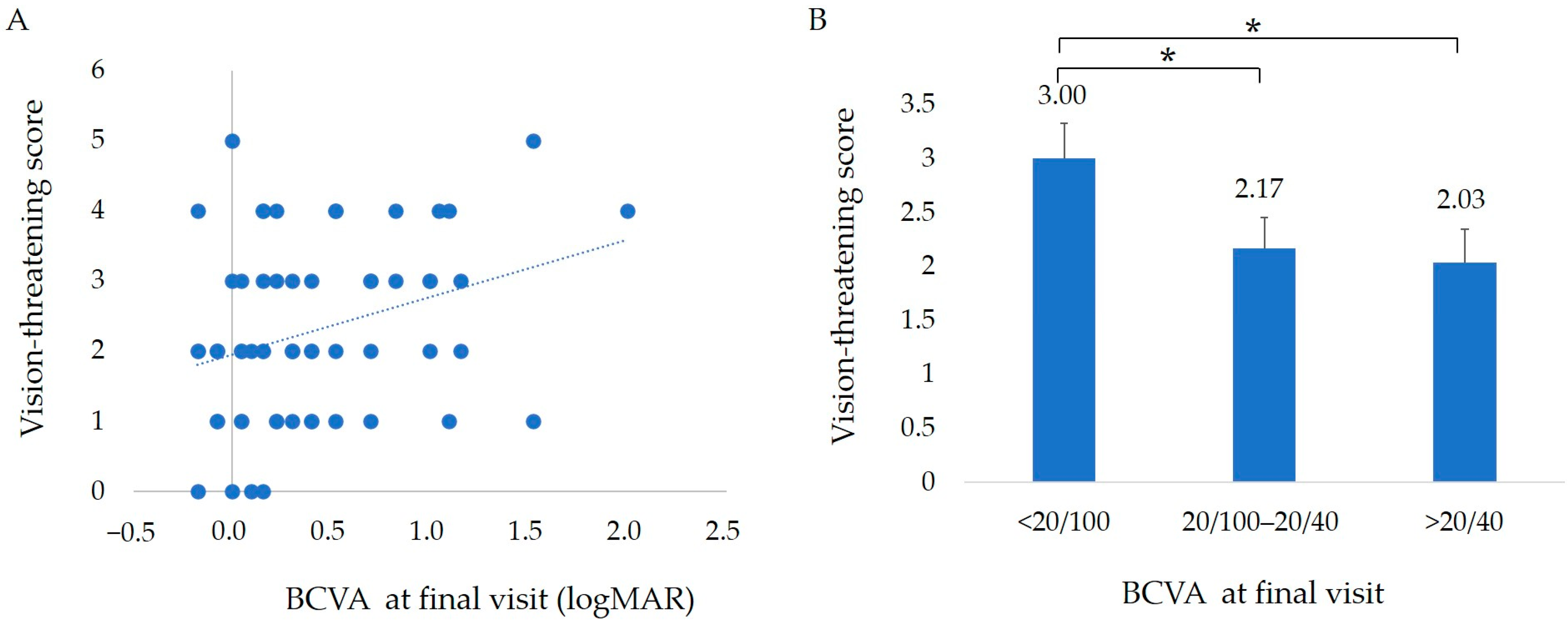
3.5. Score of Vision-Threatening Findings and Final BCVA
3.6. Correlations between the Final VA and Each Parameter
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morizane, Y.; Morimoto, N.; Fujiwara, A.; Kawasaki, R.; Yamashita, H.; Ogura, Y.; Shiraga, F. Incidence and causes of visual impairment in Japan: The first nation-wide complete enumeration survey of newly certified visually impaired individuals. Jpn. J. Ophthalmol. 2019, 63, 26–33. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Wong, D.W.; Sforzolini, B.S.; Goldbaum, M.; Tang, K.C.; Spaide, R.F.; Freund, K.B.; Slakter, J.S.; Guyer, D.R.; Sorenson, J.A.; et al. Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch. Ophthalmol. 1999, 117, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Yannuzzi, L.A.; Sorenson, J.; Spaide, R.F.; Lipson, B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina 1990, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maruko, I.; Iida, T.; Saito, M.; Nagayama, D.; Saito, K. Clinical characteristics of exudative age-related macular degeneration in Japanese patients. Am. J. Ophthalmol. 2007, 144, 15–22. [Google Scholar] [CrossRef]
- Kawasaki, R.; Wang, J.J.; Ji, G.J.; Taylor, B.; Oizumi, T.; Daimon, M.; Kato, T.; Kawata, S.; Kayama, T.; Tano, Y.; et al. Prevalence and risk factors for age-related macular degeneration in an adult Japanese population: The Funagata study. Ophthalmology 2008, 115, 1376–1381.e2. [Google Scholar] [CrossRef]
- Sho, K.; Takahashi, K.; Yamada, H.; Wada, M.; Nagai, Y.; Otsuji, T.; Nishikawa, M.; Mitsuma, Y.; Yamazaki, Y.; Matsumura, M.; et al. Polypoidal choroidal vasculopathy: Incidence, demographic features, and clinical characteristics. Arch. Ophthalmol. 2003, 121, 1392–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: One-year results of 2 randomized clinical trials—TAP report. Arch. Ophthalmol. 1999, 117, 1329–1345. [Google Scholar] [CrossRef] [Green Version]
- Verteporfin in Photodynamic Therapy Study Group. Verteporfin therapy of subfoveal choroidal neovascularization in age-related macular degeneration: Two-year results of a randomized clinical trial including lesions with occult with no classic choroidal neovascularization—Verteporfin in photodynamic therapy report 2. Am. J. Ophthalmol. 2001, 131, 541–560. [Google Scholar] [CrossRef]
- Japanese Age-Related Macular Degeneration Trial (JAT) Study Group. Japanese age-related macular degeneration trial: 1-year results of photodynamic therapy with verteporfin in Japanese patients with subfoveal choroidal neovascularization secondary to age-related macular degeneration. Am. J. Ophthalmol. 2003, 136, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Ogura, Y.; Ishibashi, T.; Shiraga, F.; Yuzawa, M. Treatment guidelines for age-related macular degeneration. Nippon. Ganka Gakkai Zasshi 2012, 116, 1150–1155. [Google Scholar]
- Lim, T.H.; Lai, T.Y.Y.; Takahashi, K.; Wong, T.Y.; Chen, L.J.; Ruamviboonsuk, P.; Tan, C.S.; Lee, W.K.; Cheung, C.M.G.; Ngah, N.F.; et al. Comparison of Ranibizumab With or Without Verteporfin Photodynamic Therapy for Polypoidal Choroidal Vasculopathy: The EVEREST II Randomized Clinical Trial. JAMA Ophthalmol. 2020, 138, 935–942. [Google Scholar] [CrossRef]
- Koh, A.; Lai, T.Y.Y.; Takahashi, K.; Wong, T.Y.; Chen, L.J.; Ruamviboonsuk, P.; Tan, C.S.; Feller, C.; Margaron, P.; Lim, T.H.; et al. Efficacy and Safety of Ranibizumab With or Without Verteporfin Photodynamic Therapy for Polypoidal Choroidal Vasculopathy: A Randomized Clinical Trial. JAMA Ophthalmol. 2017, 135, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Iida, T.; Ogura, Y.; Chen, S.J.; Wong, T.Y.; Mitchell, P.; Cheung, G.C.M.; Zhang, Z.; Leal, S.; Ishibashi, T. Efficacy and Safety of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy in the PLANET Study: A Randomized Clinical Trial. JAMA Ophthalmol. 2018, 136, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Tano, Y. Guidelines for PDT in Japan. Ophthalmology 2008, 115, 585–585.e586. [Google Scholar] [CrossRef]
- Gomi, F.; Ohji, M.; Sayanagi, K.; Sawa, M.; Sakaguchi, H.; Oshima, Y.; Ikuno, Y.; Tano, Y. One-year outcomes of photodynamic therapy in age-related macular degeneration and polypoidal choroidal vasculopathy in Japanese patients. Ophthalmology 2008, 115, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, K.; Yasuda, M.; Hata, J.; Oshima, Y.; Hashimoto, S.; Yoshitomi, T.; Kiyohara, Y.; Ishibashi, T.; Ninomiya, T.; Sonoda, K.H. Prevalence and Risk Factors for Polypoidal Choroidal Vasculopathy in a General Japanese Population: The Hisayama Study. Semin. Ophthalmol 2018, 33, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Iida, T.; Ishida, S.; Crawford, B.; Sakai, Y.; Mochizuki, A.; Tsujiuchi, R.; Tanaka, S.; Imai, K. Effectiveness of Current Treatments for Wet Age-Related Macular Degeneration in Japan: A Systematic Review and Pooled Data Analysis. Clin. Ophthalmol. 2022, 16, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, M.; Baba, T.; Kitahashi, M.; Yokouchi, H.; Kubota-Taniai, M.; Bikbova, G.; Oshitari, T.; Yamamoto, S. One-year results of intravitreal ranibizumab combined with reduced-fluence photodynamic therapy for polypoidal choroidal vasculopathy. Clin. Ophthalmol. 2014, 8, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Hatta, Y.; Ishikawa, K.; Nishihara, H.; Ozawa, S.; Ito, Y.; Terasaki, H. Effect of photodynamic therapy alone or combined with posterior subtenon triamcinolone acetonide or intravitreal bevacizumab on choroidal hypofluorescence by indocyanine green angiography. Retina 2010, 30, 495–502. [Google Scholar] [CrossRef]
- Yoshizawa, C.; Saito, W.; Hirose, S.; Kitamei, H.; Noda, K.; Ishida, S. Photodynamic therapy combined with intravitreal bevacizumab and sub-tenon triamcinolone acetonide injections for age-related macular degeneration. Jpn. J. Ophthalmol. 2013, 57, 68–73. [Google Scholar] [CrossRef]
- Wada, I.; Shiose, S.; Ishikawa, K.; Kano, K.; Notomi, S.; Mori, K.; Akiyama, M.; Nakao, S.; Sonoda, K.H. One-year efficacy of “rescue photodynamic therapy” for patients with typical age-related macular degeneration, polypoidal choroidal vasculopathy, and pachychoroid neovasculopathy refractory to anti-vascular endothelial growth factor therapy. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Fur Klin. Und Exp. Ophthalmol. 2022, 260, 2029–2036. [Google Scholar] [CrossRef]
- Liu, S.; Chhabra, R. Comparison of 3-year outcomes of photodynamic therapy combined with intravitreal ranibizumab or aflibercept for polypoidal choroidal vasculopathy in a European cohort. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Fur Klin. Und Exp. Ophthalmol. 2022, 260, 3533–3542. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, G.J.; Ying, G.S.; Toth, C.A.; Daniel, E.; Grunwald, J.E.; Martin, D.F.; Maguire, M.G. Macular Morphology and Visual Acuity in Year Five of the Comparison of Age-related Macular Degeneration Treatments Trials. Ophthalmology 2019, 126, 252–260. [Google Scholar] [CrossRef]
- Yoshida, Y.; Kohno, T.; Yamamoto, M.; Yoneda, T.; Iwami, H.; Shiraki, K. Two-year results of reduced-fluence photodynamic therapy combined with intravitreal ranibizumab for typical age-related macular degeneration and polypoidal choroidal vasculopathy. Jpn. J. Ophthalmol. 2013, 57, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, A.; Shiraga, F.; Shiragami, C.; Shirakata, Y.; Fujiwara, A. Two-year results of reduced-fluence photodynamic therapy for polypoidal choroidal vasculopathy. Am. J. Ophthalmol. 2013, 155, 96–102.e101. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.D.; Callanan, D.; Solley, W.; Avery, R.L.; Pieramici, D.J.; Aaberg, T. A prospective pilot study comparing combined intravitreal ranibizumab and half-fluence photodynamic therapy with ranibizumab monotherapy in the treatment of neovascular age-related macular degeneration. Clin. Ophthalmol. 2012, 6, 1519–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngo, W.K.; Chee, W.K.; Tan, C.S.; Lim, T.H. Comparing efficacy of reduced-fluence and standard-fluence photodynamic therapy in the treatment of polypoidal choroidal vasculopathy. BMC Ophthalmol. 2020, 20, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katome, T.; Naito, T.; Nagasawa, T.; Shiota, H. Efficacy of combined photodynamic therapy and sub-Tenon’s capsule injection of triamcinolone acetonide for age-related macular degeneration. J. Med. Investig. 2009, 56, 116–119. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, K.; Nishihara, H.; Ozawa, S.; Piao, C.H.; Ito, Y.; Kondo, M.; Terasaki, H. Focal macular electroretinograms after photodynamic therapy combined with posterior juxtascleral triamcinolone acetonide. Retina 2009, 29, 803–810. [Google Scholar] [CrossRef]
- Saito, K.; Yamamoto, T.; Tsuchiya, D.; Kawasaki, R.; Haneda, S.; Yamashita, H. Effect of combined treatment with sub-Tenon injection of triamcinolone acetonide and photodynamic therapy in Japanese patients with age-related macular degeneration. Jpn. J. Ophthalmol. 2009, 53, 512–518. [Google Scholar] [CrossRef]
- Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Yoneyama, S.; Tanabe, N.; Matsubara, M.; Mabuchi, F.; Iijima, H. Comparison of two-year outcomes after photodynamic therapy with ranibizumab or aflibercept for polypoidal choroidal vasculopathy. Sci. Rep. 2017, 7, 16461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Khanani, A.M.; Guymer, R.H.; Basu, K.; Boston, H.; Heier, J.S.; Korobelnik, J.F.; Kotecha, A.; Lin, H.; Silverman, D.; Swaminathan, B.; et al. TENAYA and LUCERNE: Rationale and Design for the Phase 3 Clinical Trials of Faricimab for Neovascular Age-Related Macular Degeneration. Ophthalmol. Sci. 2021, 1, 100076. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Sakurada, Y.A.-O.; Matsubara, M.; Kotoda, Y.; Kasai, Y.; Sugiyama, A.; Kashiwagi, K. Comparison of one-year outcomes between as-needed brolucizumab and aflibercept for polypoidal choroidal vasculopathy. Jpn. J. Ophthalmol. 2023, 67, 402–409. [Google Scholar] [CrossRef]
- Tanaka, K.A.-O.; Koizumi, H.; Tamashiro, T.; Itagaki, K.; Nakayama, M.; Maruko, I.; Wakugawa, S.; Terao, N.; Onoe, H.; Wakatsuki, Y.; et al. Short-term results for brolucizumab in treatment-naïve neovascular age-related macular degeneration: A Japanese multicenter study. Jpn. J. Ophthalmol. 2022, 66, 379–385. [Google Scholar] [CrossRef]
- Ueda-Consolvo, T.; Tanigichi, A.; Numata, A.; Oiwake, T.; Nakamura, T.; Ishida, M.; Yanagisawa, S.; Hayashi, A.A.-O. Switching to brolucizumab from aflibercept in age-related macular degeneration with type 1 macular neovascularization and polypoidal choroidal vasculopathy: An 18-month follow-up study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 261, 345–352. [Google Scholar] [CrossRef]
- Gesualdo, C.; Rossi, S.; Iodice, C.A.-O.; Guarino, F.; Petrella, M.; D’Agostino, F.A.; Perrotta, R.; Simonelli, F. Brolucizumab Intravitreal Injections for Wet Age-Related Macular Degeneration: Real-Life Study on a Cohort of Italian Patients. Medicina 2023, 59, 1110. [Google Scholar] [CrossRef]
- Mukai, R.; Kataoka, K.; Tanaka, K.; Miyara, Y.; Maruko, I.; Nakayama, M.; Watanabe, Y.; Yamamoto, A.; Wakatsuki, Y.; Onoe, H.; et al. Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan. Sci. Rep. 2023, 13, 8747. [Google Scholar] [CrossRef]
- Stanga, P.A.-O.; Valentín-Bravo, F.J.; Stanga, S.E.F.; Reinstein, U.I.; Pastor-Idoate, S.; Downes, S.M. Faricimab in neovascular AMD: First report of real-world outcomes in an independent retina clinic. Eye 2023, 1–8. [Google Scholar] [CrossRef]
- Cheung, C.M.G.; Lee, W.K.; Koizumi, H.; Dansingani, K.; Lai, T.Y.Y.; Freund, K.B. Pachychoroid disease. Eye 2019, 33, 14–33. [Google Scholar] [CrossRef] [Green Version]
- Gulkas, S.; Sahin, O. Microperimetric changes and fixation stability status after half-dose photodynamic therapy for chronic central serous chorioretinopathy. Eur. J. Ophthalmol. 2020, 30, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Maruko, I.; Iida, T.; Sugano, Y.; Furuta, M.; Sekiryu, T. One-year choroidal thickness results after photodynamic therapy for central serous chorioretinopathy. Retina 2011, 31, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Takeuchi, J.; Kataoka, K.; Ota, H.; Asai, K.; Nakano, Y.; Horiguchi, E.; Taki, Y.; Ito, Y.; Terasaki, H.; et al. Effects of half-dose photodynamic therapy on chronic central serous chorioretinopathy with or without macular neovascularization assessed using optical coherence tomography angiography. Retina 2022, 42, 2346–2353. [Google Scholar] [CrossRef] [PubMed]
- Sirks, M.J.; van Dijk, E.H.C.; Rosenberg, N.; Hollak, C.E.M.; Aslanis, S.; Cheung, C.M.G.; Chowers, I.; Eandi, C.M.; Freund, K.B.; Holz, F.G.; et al. Clinical impact of the worldwide shortage of verteporfin (Visudyne®) on ophthalmic care. Acta Ophthalmol. 2022, 100, e1522–e1532. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Initial PDTGroup | 35 Patients 38 Eyes | |
| Age | 69.1 ± 11.1 years | |
| Follow-up period | 6.2 ± 2.64 years | |
| GLD | 3047 ± 1223 µm | |
| Treatment regimen for initial PDT | PDT + STTA | 29 eyes (76%) |
| PDT + STTA + anti-VEGF | 5 eyes (13%) | |
| PDT | 4 eyes (11%) | |
| Rescue PDT Group | 22 Patients 22 Eyes | |
| Age | 69.8 ± 8.7 years | |
| Follow-up period | 5.8 ± 2.7 years | |
| GLD | 3200 ± 1110 µm | |
| Previous VEGF inhibitor therapy | 7.3 ± 6.3 times | |
| Time from initial treatment | 1.6 ± 1.5 years | |
| Follow-up period after initial PDT | 4.3 ± 2.5 years | |
| Previous treatment regimen with anti-VEGF | PRN | 19 eyes (86%) |
| TAE | 2 eyes (9%) | |
| PRN switched to TAE | 1 eye (5%) | |
| Reasons for rescue PDT | Frequent recurrences | 13 eyes (59%) |
| Resistance to treatment | 5 eyes (23%) | |
| Patient request | 4 eyes (18%) | |
| Treatment regimen for rescue PDT | PDT + STTA | 14 eyes (64%) |
| PDT + STTA + anti-VEGF | 8 eyes (36%) | |
| Period | Treated Eyes | Additional Treatment and Numbers | ||
|---|---|---|---|---|
| Initial PDT group (38 eyes) | Within 1 year | 17 eyes (45%) | Anti-VEGF (12 eyes) | 2.3 ± 1.2 times |
| PDT + STTA (4 eyes) | 1.0 ± 0 times | |||
| PDT + STTA + anti-VEGF (1 eye) | 1 (PDT)/1 (anti-VEGF) times | |||
| During follow-up period (mean, 6.2 years) | 27 eyes (71%) | Anti-VEGF (21 eyes) | 7.5 ± 6.7 times | |
| PDT + STTA (3 eyes) | 1.0 ± 0 times | |||
| PDT + STTA + anti-VEGF (3 eyes) | 1.3 ± 0.5 (PDT)/18.3 ± 15.5 (anti-VEGF) times | |||
| Rescue PDT group (22 eyes) | Within 1 year | 13 eyes (59%) | Anti-VEGF (11 eyes) | 1.9 ± 1.3 times |
| PDT + STTA (0 eyes) | ||||
| PDT + STTA + anti-VEGF (2 eyes) | 1.0 ± 0 (PDT)/1.0 ± 0 (anti-VEGF) times | |||
| During follow-up period (mean, 4.3 years) | 21 eyes (95%) | Anti-VEGF (16 eyes) | 7.0 ± 6.0 times | |
| PDT + STTA (0 eyes) | ||||
| PDT + STTA + anti-VEGF (5 eyes) | 1.4 ± 0.8 (PDT)/5.8 ± 2.8 (anti-VEGF) times | |||
| rs | p | ||
|---|---|---|---|
| Time until additional treatment | −0.260 | 0.045 | |
| Anatomic findings before treatment | SRF | −0.075 a | 0.569 |
| IRF | 0.048 a | 0.714 | |
| Serous PED | 0.322 a | 0.012 | |
| SRH | −0.061 a | 0.643 | |
| HE | 0.263 a | 0.042 | |
| SHRM | 0.092 a | 0.483 | |
| GLD | 0.131 a | 0.318 | |
| Vision-threatening score | 0.273 a | 0.035 | |
| BCVA at baseline | 0.277 | 0.032 | |
| BCVA at year 1 | 0.758 | 0.000 | |
| Anatomic findings at final visit | Fibrosis | 0.286 a | 0.026 |
| Atrophy | 0.358 a | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakaeda, Y.; Kato, A.; Kuwayama, S.; Hirahara, S.; Suzuki, N.; Ogura, Y.; Nakazawa, Y.; Yasukawa, T. Long-Term Prognosis of Patients with Polypoidal Choroidal Vasculopathy Treated with Photodynamic Therapy. J. Clin. Med. 2023, 12, 4707. https://doi.org/10.3390/jcm12144707
Sakaeda Y, Kato A, Kuwayama S, Hirahara S, Suzuki N, Ogura Y, Nakazawa Y, Yasukawa T. Long-Term Prognosis of Patients with Polypoidal Choroidal Vasculopathy Treated with Photodynamic Therapy. Journal of Clinical Medicine. 2023; 12(14):4707. https://doi.org/10.3390/jcm12144707
Chicago/Turabian StyleSakaeda, Yukinori, Aki Kato, Soichiro Kuwayama, Shuichiro Hirahara, Norihiro Suzuki, Yuichiro Ogura, Yoko Nakazawa, and Tsutomu Yasukawa. 2023. "Long-Term Prognosis of Patients with Polypoidal Choroidal Vasculopathy Treated with Photodynamic Therapy" Journal of Clinical Medicine 12, no. 14: 4707. https://doi.org/10.3390/jcm12144707