
Defining the Role of Anaortic Coronary Artery Bypass Grafting

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:
Author Contributions
Funding
Conflicts of Interest
References
- Ramponi, F.; Seco, M.; Edelman, J.B.; Sherrah, A.G.; Bannon, P.G.; Brereton, R.J.; Wilson, M.K.; Vallely, M.P. Dual inflow, total-arterial, anaortic, off-pump coronary artery bypass grafting: How to do it. Ann. Cardiothorac. Surg. 2018, 7, 552–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallely, M.P.; Seco, M.; Ramponi, F.; Puskas, J.D. Total-arterial, anaortic, off-pump coronary artery surgery: Why, when, and how. JTCVS Tech. 2021, 10, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Ramponi, F.; Seco, M.; Brereton, R.J.; Gaudino, M.F.; Puskas, J.D.; Calafiore, A.M.; Vallely, M.P. Toward stroke-free coronary surgery: The role of the anaortic off-pump bypass technique. J. Card. Surg. 2021, 36, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
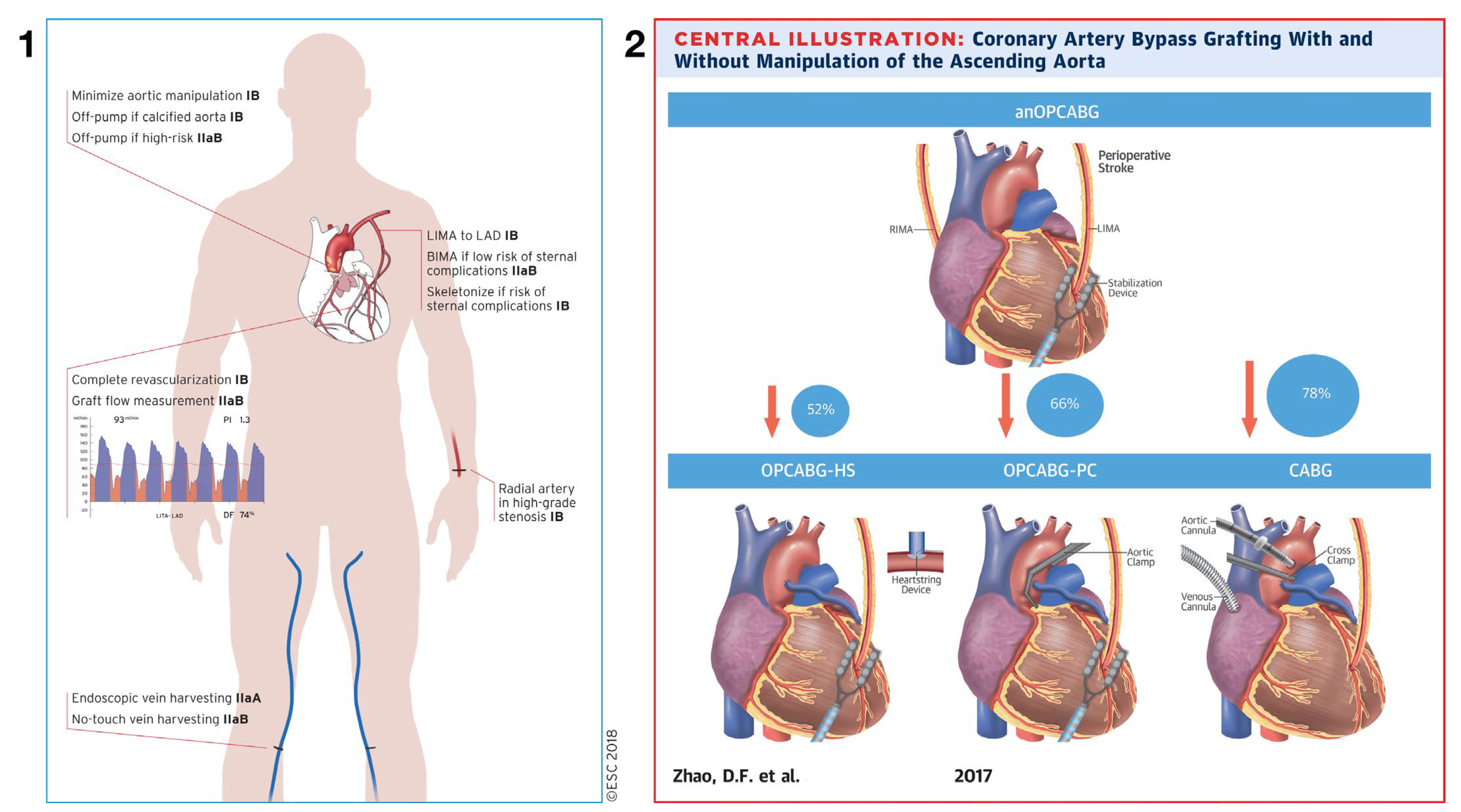
- Zhao, D.F.; Edelman, J.J.; Seco, M.; Bannon, P.G.; Wilson, M.K.; Byrom, M.J.; Thourani, V.; Lamy, A.; Taggart, D.P.; Puskas, J.D.; et al. Coronary Artery Bypass Grafting with and Without Manipulation of the Ascending Aorta: A Network Meta-Analysis. J. Am. Coll. Cardiol. 2017, 69, 924–936. [Google Scholar] [CrossRef] [PubMed]
- Chavanon, O.; Carrier, M.; Cartier, R.; Hébert, Y.; Pellerin, M.; Pagé, P.; Perrault, L.P. Increased incidence of acute ascending aortic dissection with off-pump aortocoronary bypass surgery? Ann. Thorac. Surg. 2001, 71, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Gaudino, M.; Benesch, C.; Bakaeen, F.; DeAnda, A.; Fremes, S.E.; Glance, L.; Messe, S.R.; Pandey, A.; Rong, L.Q.; American Heart Association Council on Cardiovascular Surgery and Anesthesia; et al. Considerations for Reduction of Risk of Perioperative Stroke in Adult Patients Undergoing Cardiac and Thoracic Aortic Operations: A Scientific Statement from the American Heart Association. Circulation 2020, 142, e193–e209. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Browne, A.; Spence, J.; Power, P.; Copland, I.; Mian, R.; Gagnon, S.; Kennedy, S.; Sharma, M.; Lamy, A. Perioperative covert stroke in patients undergoing coronary artery bypass graft surgery. JTCVS Open 2020, 4, 1–11. [Google Scholar] [CrossRef]
- Gaudino, M.; Rahouma, M.; Di Mauro, M.; Yanagawa, B.; Abouarab, A.; Demetres, M.; Di Franco, A.; Arisha, M.J.; Ibrahim, D.A.; Baudo, M.; et al. Early Versus Delayed Stroke After Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012447. [Google Scholar] [CrossRef]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Paolasso, E.; Straka, Z.; Piegas, L.S.; Akar, A.R.; Jain, A.R.; et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N. Engl. J. Med. 2012, 366, 1489–1497. [Google Scholar] [CrossRef] [Green Version]
- Szwed, K.; Pawliszak, W.; Szwed, M.; Tomaszewska, M.; Anisimowicz, L.; Borkowska, A. Reducing delirium and cognitive dysfunction after off-pump coronary bypass: A randomized trial. J. Thorac. Cardiovasc. Surg. 2021, 161, 1275–1282. [Google Scholar] [CrossRef]
- Vallely, M.P.; Yan, T.D.; Edelman, J.J.; Hayman, M.; Brereton, R.J.; Ross, D.E. Anaortic, total-arterial, off-pump coronary artery bypass surgery: How to do it. Heart Lung Circ. 2010, 19, 555–560. [Google Scholar] [CrossRef]
- Suzuki, T.; Asai, T.; Nota, H.; Kuroyanagi, S.; Kinoshita, T.; Takashima, N.; Hayakawa, M. Early and long-term patency of in situ skeletonized gastroepiploic artery after off-pump coronary artery bypass graft surgery. Ann. Thorac. Surg. 2013, 96, 90–95. [Google Scholar] [CrossRef]
- Shimahara, Y.; Fukushima, S.; Kawamoto, N.; Tadokoro, N.; Nakai, M.; Kobayashi, J.; Fujita, T. Additional survival benefit of bilateral in situ internal thoracic artery grafting with composite radial artery graft in total arterial off-pump coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef]
- Royse, A.G.; Brennan, A.P.; Ou-Young, J.; Pawanis, Z.; Canty, D.J.; Royse, C.F. 21-Year Survival of Left Internal Mammary Artery-Radial Artery-Y Graft. J. Am. Coll. Cardiol. 2018, 72, 1332–1340. [Google Scholar] [CrossRef]
- Taggart, D.P.; Altman, D.G.; Gray, A.M.; Lees, B.; Gerry, S.; Benedetto, U.; Flather, M. ART Investigators. Randomized Trial of Bilateral versus Single Internal-Thoracic- Artery Grafts. N. Engl. J. Med. 2016, 375, 2540–2549. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.Y.; Seco, M.; Harris, S.R.; Koullouros, M.; Ramponi, F.; Wilson, M.; Bannon, P.G.; Vallely, M.P. Bilateral Versus Single Internal Mammary Artery Use in Coronary Artery Bypass Grafting: A Propensity Matched Analysis. Heart Lung Circ. 2019, 28, 807–813. [Google Scholar] [CrossRef]
- Dai, C.; Lu, Z.; Zhu, H.; Xue, S.; Lian, F. Bilateral internal mammary artery grafting and risk of sternal wound infection: Evidence from observational studies. Ann. Thorac. Surg. 2013, 95, 1938–1945. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, K.B. Saphenous Vein Versus Right Internal Thoracic Artery as a Y-Composite Graft: Ten-Year Angiographic and Long-Term Clinical Results of the SAVE RITA Trial. Circulation 2021, 144, 1186–1188. [Google Scholar] [CrossRef]
- Yanagawa, B.; Verma, S.; Jüni, P.; Tam, D.Y.; Mazine, A.; Puskas, J.D.; Friedrich, J.O. A systematic review and meta-analysis of in situ versus composite bilateral internal thoracic artery grafting. J. Thorac. Cardiovasc. Surg. 2017, 153, 1108–1116.e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, J.; Royse, C.; Siderakis, C.; Srivastav, N.; Royse, A. Long-term observational angiographic patency and perfect patency of radial artery compared with saphenous vein or internal mammary artery in coronary bypass surgery. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Sandner, S.; Di Giammarco, G.; Di Franco, A.; Arai, H.; Asai, T.; Bakaeen, F.; Doenst, T.; Fremes, S.E.; Glineur, D.; et al. The Use of Intraoperative Transit Time Flow Measurement for Coronary Artery Bypass Surgery: Systematic Review of the Evidence and Expert Opinion Statements. Circulation 2021, 144, 1160–1171. [Google Scholar] [CrossRef] [PubMed]
- Hardisky, D.; Vijayakumar, A.; Whitson, B.A.; Lilly, S.M.; Boudoulas, K.D.; Vallely, M.P. Concomitant anaortic OPCAB and transfemoral TAVR for high-risk patients: A case series. J. Card. Surg. 2022, 37, 3935–3942. [Google Scholar] [CrossRef] [PubMed]
- Ramponi, F.; Seco, M.; Bannon, P.G.; Kritharides, L.; Qasabian, R.; Wilson, M.K.; Vallely, M.P. Synchronous carotid endarterectomy and anaortic off-pump coronary artery bypass surgery. Heart Lung Circ. 2023, 32, 645–651. [Google Scholar] [CrossRef]
- Ramponi, F.; Vallely, M.P. Concomitant coronary and carotid artery disease: Systematic review and network meta-analysis of available surgical treatments. In Proceedings of the STS Coronary Meeting, Ottawa, ON, Canada, 4–5 June 2022. Oral communication. [Google Scholar]
- Kerendi, F.; Morris, C.D.; Puskas, J.D. Off-pump coronary bypass surgery for high-risk patients: Only in expert centers? Curr. Opin. Cardiol. 2008, 23, 573–578. [Google Scholar] [CrossRef]
- Badhwar, V.; Vemulapalli, S.; Mack, M.A.; Gillinov, A.M.; Chikwe, J.; Dearani, J.A.; Grau-Sepulveda, M.V.; Habib, R.; Rankin, J.S.; Jacobs, J.P.; et al. Volume-Outcome Association of Mitral Valve Surgery in the United States. JAMA Cardiol. 2020, 5, 1092–1101. [Google Scholar] [CrossRef]
- Puskas, J.D.; Gaudino, M.; Taggart, D.P. Experience Is Crucial in Off-Pump Coronary Artery Bypass Grafting. Circulation 2019, 139, 1872–1875. [Google Scholar] [CrossRef]
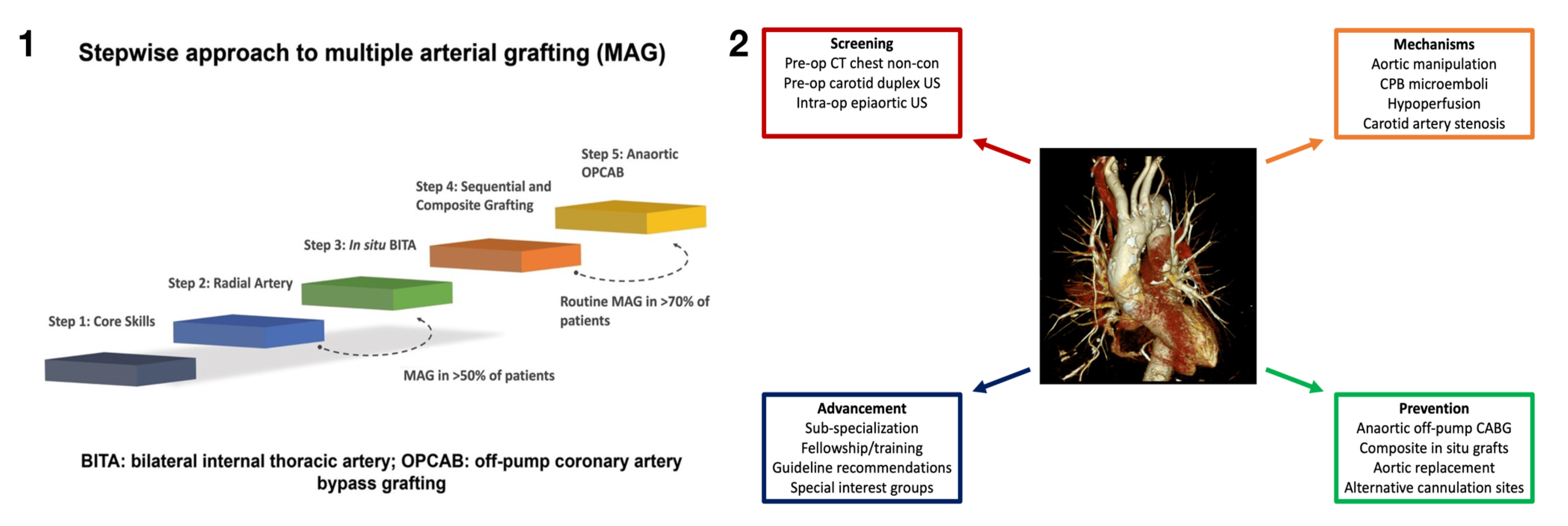
- Gaudino, M.F.; Sandner, S.; Bonalumi, G.; Lawton, J.S.; Fremes, S.E. Coronary Task Force of the European Association for Cardio-Thoracic Surgery. How to build a multi-arterial coronary artery bypass programme: A stepwise approach. Eur. J. Cardiothorac. Surg. 2020, 58, 1111–1117. [Google Scholar] [CrossRef]
- Rosati, C.M.; Torregrossa, G.; Balkhy, H.H.; Puskas, J.D. Dedicated training in advanced coronary surgery: Need and opportunity. J. Thorac. Cardiovasc. Surg. 2021, 161, 2130–2134. [Google Scholar] [CrossRef]
- Royse, A.; Pawanis, Z.; Canty, D.; Ou-Young, J.; Eccleston, D.; Ajani, A.; Reid, C.M.; Bellomo, R.; Royse, C. The effect on survival from the use of a saphenous vein graft during coronary bypass surgery: A large cohort study. Eur. J. Cardiothorac. Surg. 2018, 54, 1093–1100. [Google Scholar] [CrossRef]
- Buxton, B.F.; Hayward, P.A. The art of arterial revascularization-total arterial revascularization in patients with triple vessel coronary artery disease. Ann. Cardiothorac. Surg. 2013, 2, 543–551. [Google Scholar]
- Taggart, D.P. How I deploy arterial grafts. Ann. Cardiothorac. Surg. 2018, 7, 690–697. [Google Scholar] [CrossRef] [Green Version]
- Seco, M.; Ramponi, F.; Brereton, R.J.; Bigelow, G.A.; Ganapathi, A.M.; Vallely, M.P. Anaortic, off-pump coronary artery bypass using multiple arterial grafts: Surgical technique. Vessel Plus 2021, 5, 18. [Google Scholar] [CrossRef]
- Mascia, G.; Crotti, L.; Groppelli, A.; Canepa, M.; Merlo, A.C.; Benenati, S.; Di Donna, P.; Della Bona, R.; Soranna, D.; Zambon, A.; et al. Syncope in hypertrophic cardiomyopathy (part I): An updated systematic review and meta-analysis. Int. J. Cardiol. 2022, 357, 88–94. [Google Scholar] [CrossRef]
- Balkhy, H.H.; Nisivaco, S.; Kitahara, H.; Torregrossa, G.; Patel, B.; Grady, K.; Coleman, C. Robotic off-pump totally endoscopic coronary artery bypass in the current era: Report of 544 patients. Eur. J. Cardiothorac. Surg. 2022, 61, 439–446. [Google Scholar] [CrossRef]
- Balkhy, H.H.; Nisivaco, S.; Kitahara, H.; AbuTaleb, A.; Nathan, S.; Hamzat, I. Robotic advanced hybrid coronary revascularization: Outcomes with two internal thoracicartery grafts and stents. JTCVS Tech. 2022, 16, 76–88. [Google Scholar] [CrossRef]
- Hannan, E.L.; Wu, Y.; Cozzens, K.; Sundt, I.I.I.T.M.; Girardi, L.; Chikwe, J.; Wechsler, A.; Smith, C.R.; Gold, J.P.; Lahey, S.J.; et al. Hybrid Coronary Revascularization Versus Conventional Coronary Artery Bypass Surgery: Utilization and Comparative Outcomes. Circ. Cardiovasc. Interv. 2020, 13, e009386. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramponi, F.; Seco, M.; Vallely, M.P. Defining the Role of Anaortic Coronary Artery Bypass Grafting. J. Clin. Med. 2023, 12, 4697. https://doi.org/10.3390/jcm12144697
Ramponi F, Seco M, Vallely MP. Defining the Role of Anaortic Coronary Artery Bypass Grafting. Journal of Clinical Medicine. 2023; 12(14):4697. https://doi.org/10.3390/jcm12144697
Chicago/Turabian StyleRamponi, Fabio, Michael Seco, and Michael P. Vallely. 2023. "Defining the Role of Anaortic Coronary Artery Bypass Grafting" Journal of Clinical Medicine 12, no. 14: 4697. https://doi.org/10.3390/jcm12144697