
Quality of Life and Kidney Function in Older Adults: Prospective Data of the SCOPE Study

 , ,
, ,  , , , , , , , , , and
on behalf of the SCOPE Investigators
, , , , , , , , , and
on behalf of the SCOPE Investigators
Abstract
:1. Introduction
2. Materials and Methods
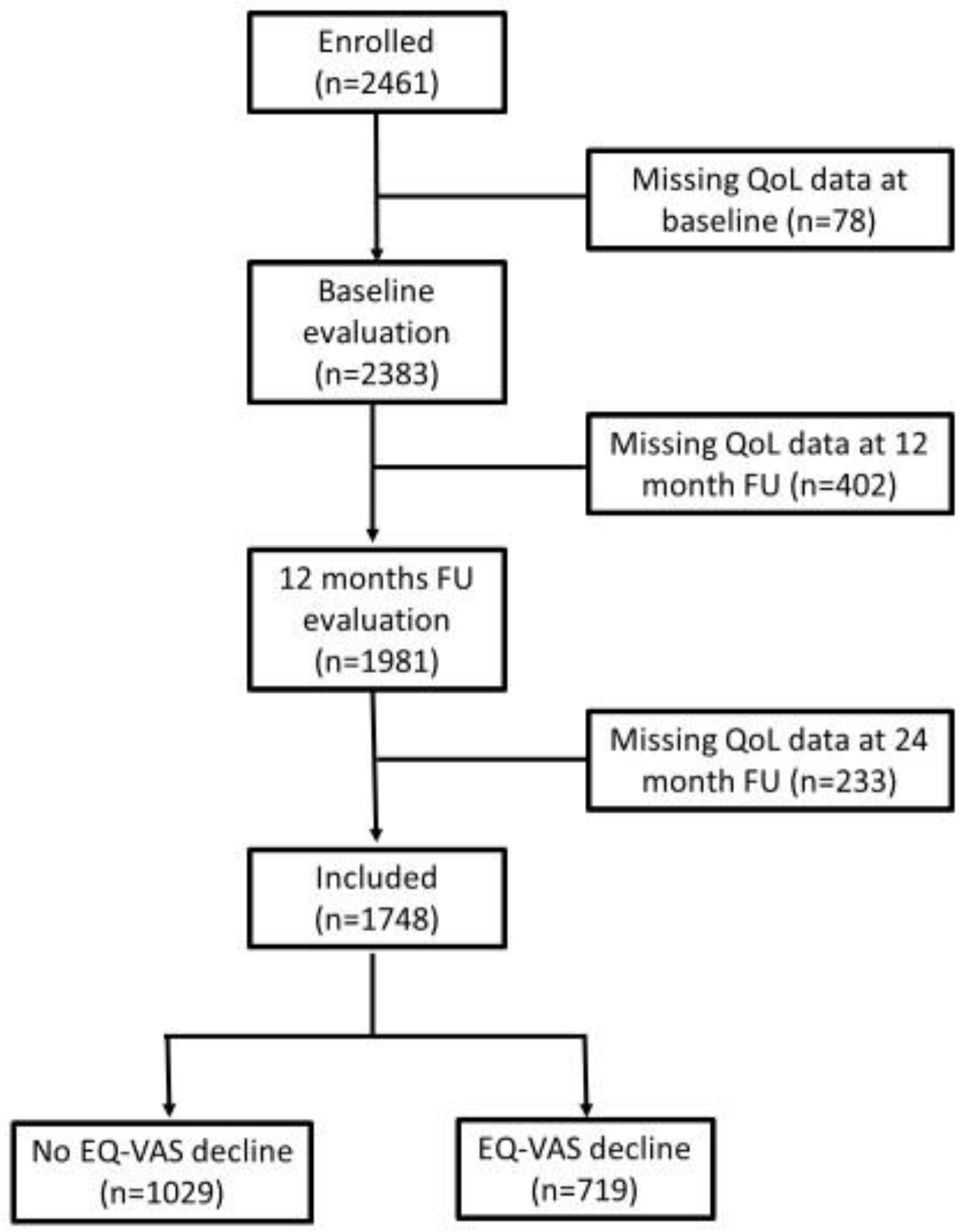
2.1. Study Design and Participants
2.2. Study Protocol and Instruments
2.3. HRQoL Assessment
2.4. HRQoL Decline Outcome
2.5. Kidney Function Evaluation
2.6. CKD Progression Outcome
2.7. Physical and Mental Functions Decline Outcomes
2.8. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
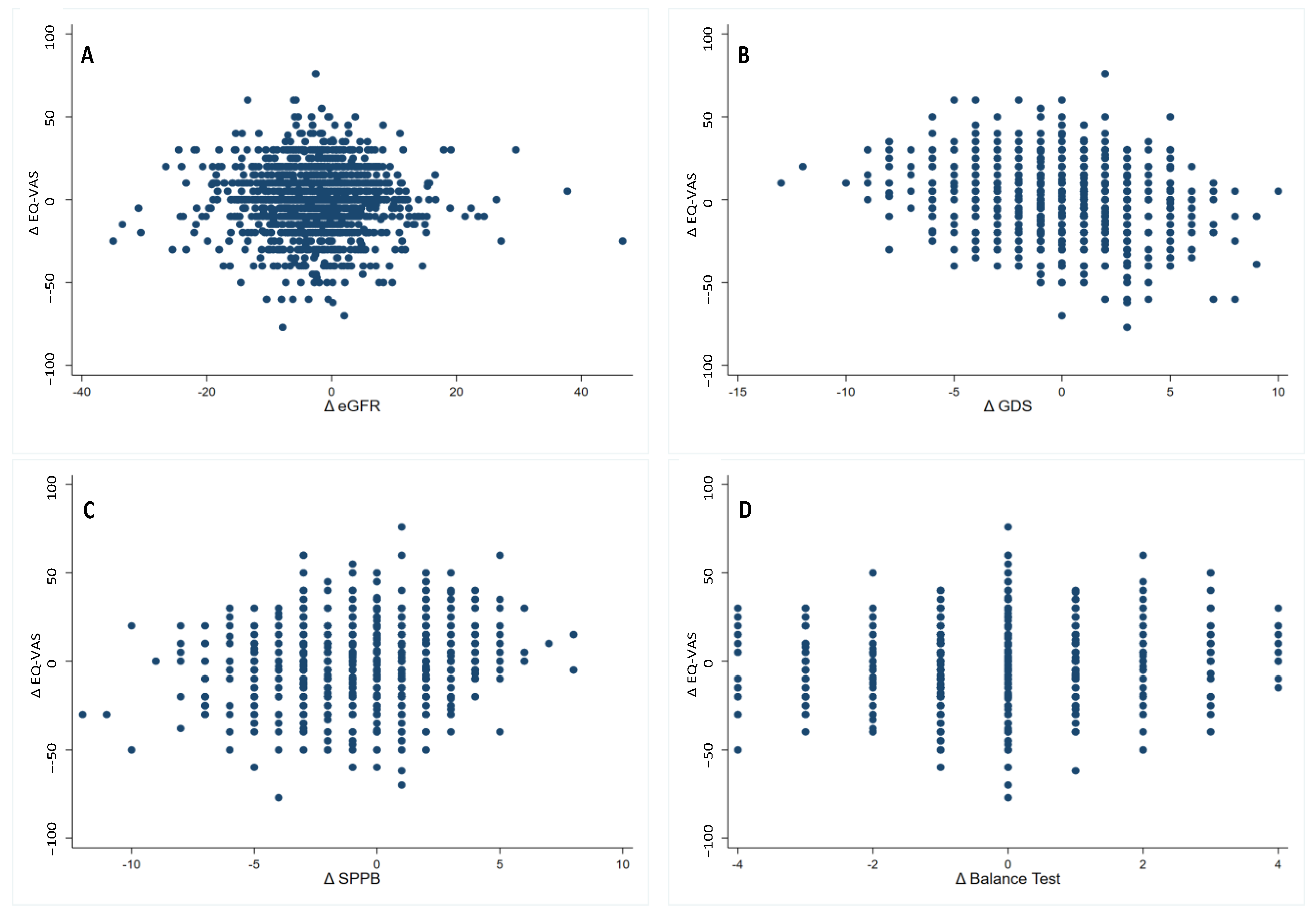
3.2. Associations between Δ EQ-VAS, Δ eGFR, and Other Health-Related Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
- Italian National Research Center on Aging (INRCA), Italy, #2015 0522 IN, 17 January 2016.
- University of Lodz, Poland, #RNN/314/15/KE, 17 November 2015.
- Medizinische Universität Graz, Austria, #28–314 ex 15/16, 5 August 2016.
- Erasmus Medical Center Rotterdam, The Netherland, #MEC-2016-036—#NL56039.078.15, v.4, 7 March 2016.
- Hospital Clínico San Carlos, Madrid, Spain, # 15/532-E_BC, 16 September 2016.
- Bellvitge University Hospital Barcellona, Spain, #PR204/15, 29 January 2016.
- Friedrich-Alexander University Erlangen-Nürnberg, Germany, #340_15B, 21 January 2016.
- Helsinki committee in Maccabi Healthcare Services, Bait Ba-lev, Bat Yam, Israel, #45/2016, 24 July 2016.
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurella, M.; Chertow, G.M.; Fried, L.F.; Cummings, S.R.; Harris, T.; Simonsick, E.; Satterfield, S.; Ayonayon, H.; Yaffe, K. Chronic kidney disease and cognitive impairment in the elderly: The health, aging, and body composition study. J. Am. Soc. Nephrol. 2005, 16, 2127–2133. [Google Scholar] [CrossRef] [Green Version]
- Lattanzio, F.; Corsonello, A.; Abbatecola, A.M.; Volpato, S.; Pedone, C.; Pranno, L.; Laino, I.; Garasto, S.; Corica, F.; Passarino, G.; et al. Relationship between renal function and physical performance in elderly hospitalized patients. Rejuvenation Res. 2012, 15, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Pedone, C.; Corsonello, A.; Bandinelli, S.; Pizzarelli, F.; Ferrucci, L.; Incalzi, R.A. Relationship between renal function and functional decline: Role of the estimating equation. J. Am. Med. Dir. Assoc. 2012, 13, e11–e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duenhas, M.R.; Draibe, S.A.; Avesani, C.M.; Sesso, R.; Cuppari, L. Influence of renal function on spontaneous dietary intake and on nutritional status of chronic renal insufficiency patients. Eur. J. Clin. Nutr. 2003, 57, 1473–1478. [Google Scholar] [CrossRef] [Green Version]
- Foley, R.N.; Wang, C.; Ishani, A.; Collins, A.J.; Murray, A.M. Kidney function and sarcopenia in the United States general population: NHANES III. Am. J. Nephrol. 2007, 27, 279–286. [Google Scholar] [CrossRef]
- Fried, L.F.; Lee, J.S.; Shlipak, M.; Chertow, G.M.; Green, C.; Ding, J.; Harris, T.; Newman, A.B. Chronic kidney disease and functional limitation in older people: Health, aging and body composition study. J. Am. Geriatr. Soc. 2006, 54, 750–756. [Google Scholar] [CrossRef]
- Roshanravan, B.; Khatri, M.; Robinson-Cohen, C.; Levin, G.; Patel, K.V.; de Boer, I.H.; Seliger, S.; Ruzinski, J.; Himmelfarb, J.; Kestenbaum, B. A prospective study of frailty in nephrology-referred patients with CKD. Am. J. Kidney Dis. 2012, 60, 912–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, P.; Vasa, P.; Brenner, D.; Iglar, K.; McFarlane, P.; Morrison, H.; Badawi, A. Prevalence estimates of chronic kidney disease in Canada: Results of a nationally representative survey. CMAJ 2013, 185, E417–E423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, T.R.; Choi, H.S.; Kim, C.S.; Bae, E.H.; Oh, Y.K.; Kim, Y.-S.; Choi, K.H.; Kim, S.W.; Ma, S.K. Association between health related quality of life and progression of chronic kidney disease. Sci. Rep. 2019, 9, 19595. [Google Scholar] [CrossRef] [Green Version]
- Chadban, S.J.; Briganti, E.M.; Kerr, P.G.; Dunstan, D.W.; Welborn, T.A.; Zimmet, P.Z.; Atkins, R.C. Prevalence of kidney damage in Australian adults: The AusDiab kidney study. J. Am. Soc. Nephrol. 2003, 7, S131–S138. [Google Scholar] [CrossRef] [Green Version]
- Hunsicker, L.G. The consequences and costs of chronic kidney disease before ESRD. J. Am. Soc. Nephrol. 2004, 15, 1363–1364. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Jo, M.W.; Go, D.S.; Ryu, D.R.; Park, J. Economic burden of chronic kidney disease in Korea using national sample cohort. J. Nephrol. 2017, 30, 787–793. [Google Scholar] [CrossRef]
- Artzi-Medvedik, R.; Kob, R.; Fabbietti, P.; Lattanzio, F.; Corsonello, A.; Melzer, Y.; Roller-Wirnsberger, R.; Wirnsberger, G.; Mattace-Raso, F.; Tap, L.; et al. SCOPE investigators. Impaired kidney function is associated with lower quality of life among community-dwelling older adults: The screening for CKD among older people across Europe (SCOPE) study. BMC Geriatr. 2020, 20, 340. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis 2002, 39, S1–S266. [Google Scholar]
- Centers of Disease Control and Prevention. Health-Related Quality of Life (HRQoL). Available online: https://www.cdc.gov/hrqol/index.htm#:~:text=Related%20Pages,and%20mental%20health%20over%20time (accessed on 14 December 2022).
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J. Am. Soc. Nephrol. 2001, 12, 2797–2806. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.A.; Bragg-Gresham, J.L.; Satayathum, S.; McCullough, K.; Pifer, T.; Goodkin, D.A.; Mapes, D.L.; Young, E.W.; Wolfe, R.A.; Held, P.J.; et al. Worldwide Dialysis Outcomes and Practice Patterns Study Committee. Health-related quality of life and associated outcomes among hemodialysis patients of different ethnicities in the United States: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2003, 41, 605–615. [Google Scholar] [CrossRef]
- Perl, J.; Karaboyas, A.; Morgenstern, H.; Sen, A.; Rayner, H.C.; Vanholder, R.C.; Combe, C.; Hasegawa, T.; Finkelstein, F.O.; Lopes, A.A.; et al. Association between changes in quality of life and mortality in hemodialysis patients: Results from the DOPPS. Nephrol. Dial. Transplant. 2017, 32, 521–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picariello, F.; Moss-Morris, R.; Macdougall, I.C.; Chilcot, A.J. The role of psychological factors in fatigue among end-stage kidney disease patients: A critical review. Clin. Kidney J. 2017, 10, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Ju, A.; Unruh, M.L.; Davison, S.N.; Dapueto, J.; Dew, M.A.; Fluck, R.; Germain, M.; Jassal, S.V.; Obrador, G.; O’donoghue, D.; et al. Patient-reported outcome measures for fatigue in patients on hemodialysis: A systematic review. Am. J. Kidney Dis. 2018, 71, 327–343. [Google Scholar] [CrossRef]
- Perlman, R.L.; Finkelstein, F.O.; Liu, L.; Roys, E.; Kiser, M.; Eisele, G.; Burrows-Hudson, S.; Messana, J.M.; Levin, N.; Rajagopalan, S.; et al. Quality of life in chronic kidney disease (CKD): A cross-sectional analysis in the Renal Research Institute-CKD study. Am. J. Kidney Dis. 2005, 45, 658–666. [Google Scholar] [CrossRef]
- Kalender, B.; Ozdemir, A.C.; Dervisoglu, E.; Ozdemir, O. Quality of life in chronic kidney disease: Effects of treatment modality, depression, malnutrition and inflammation. Int. J. Clin. Pract. 2007, 61, 569–576. [Google Scholar] [CrossRef]
- Rosansky, S.J. Renal function trajectory is more important than chronic kidney disease stage for managing patients with chronic kidney disease. Am. J. Nephrol. 2012, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yapa, H.E.; Purtell, L.; Chambers, S.; Bonner, A. The relationship between chronic kidney disease, symptoms and health-related quality of life: A systematic review. J. Ren. Care 2020, 46, 74–84. [Google Scholar] [CrossRef]
- Fukuhara, S.; Yamazaki, S.; Marumo, F.; Akiba, T.; Akizawa, T.; Fujimi, S.; Haruki, S.; Kawaguchi, Y.; Nihei, H.; Shoji, T.; et al. Health-related quality of life of predialysis patients with chronic renal failure. Nephron. Clin. Pract. 2007, 105, c1–c8. [Google Scholar] [CrossRef]
- Porter, A.; Fischer, M.J.; Wang, X.; Brooks, D.; Bruce, M.; Charleston, J.; Cleveland, W.H.; Dowie, D.; Faulkner, M.; Gassman, J.; et al. AASK Study Group. Quality of life and outcomes in African Americans with CKD. J. Am. Soc. Nephrol. 2014, 25, 1849–1855. [Google Scholar] [CrossRef] [Green Version]
- Porter, A.C.; Lash, J.P.; Xie, D.; Pan, Q.; DeLuca, J.; Kanthety, R.; Kusek, J.W.; Lora, C.M.; Nessel, L.; Ricardo, A.C.; et al. CRIC Study Investigators. Predictors and outcomes of health-related quality of life in adults with CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.-C.; Hung, C.-C.; Hwang, S.-J.; Wang, S.-L.; Hsiao, S.-M.; Lin, M.-Y.; Kung, L.-F.; Hsiao, P.-N.; Chen, H.-C. Quality of life predicts risks of end-stage renal disease and mortality in patients with chronic kidney disease. Nephrol. Dial. Transplant. 2010, 25, 1621–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corsonello, A.; on behalf of SCOPE investigators; Tap, L.; Roller-Wirnsberger, R.; Wirnsberger, G.; Zoccali, C.; Kostka, T.; Guligowska, A.; Mattace-Raso, F.; Gil, P.; et al. SCOPE investigators. Design and methodology of the screening for CKD among older patients across Europe (SCOPE) study: A multicenter cohort observational study. BMC Nephrol. 2018, 19, 260. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.T.; Staskin, D.R.; Kaplan, S.A.; MacDiarmid, S.A.; Newman, D.K.; Ohl, D.A. A practical guide to the evaluation and treatment of male lower urinary tract symptoms in the primary care setting. Int. J. Clin. Pract. 2007, 61, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Conwell, Y.; Forbes, N.T.; Cox, C.; Caine, E.D. Validation of a measure of physical illness burden at autopsy: The Cumulative Illness Rating Scale. J. Am. Geriatr. Soc. 1993, 41, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Lesher, E.L.; Berryhill, J.S. Validation of the Geriatric Depression Scale--Short Form among inpatients. J. Clin. Psychol. 1994, 50, 256–260. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Research Foundation. EQ-5D-5L User Guide. 2019. Available online: https://euroqol.org/publications/user-guides (accessed on 14 December 2022).
- Schaeffner, E.S.; Ebert, N.; Delanaye, P.; Frei, U.; Gaedeke, J.; Jakob, O.; Kuhlmann, M.K.; Schuchardt, M.; Tölle, M.; Ziebig, R.; et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann. Intern. Med. 2012, 157, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Shardlow, A.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Chronic kidney disease in primary care: Outcomes after five years in a prospective cohort study. PLoS Med. 2016, 13, e1002128. [Google Scholar] [CrossRef] [Green Version]
- Wyld, M.; Morton, R.L.; Hayen, A.; Howard, K.; Webster, A.C. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLoS Med. 2012, 9, e1001307. [Google Scholar] [CrossRef]
- Krishnan, A.; Teixeira-Pinto, A.; Lim, W.H.; Howard, K.; Chapman, J.R.; Castells, A.; Roger, S.D.; Bourke, M.J.; Macaskill, P.; Williams, G.; et al. Health-related quality of life in people across the spectrum of CKD. Kidney Int. Rep. 2020, 5, 2264–2274. [Google Scholar] [CrossRef]
- Fraser, S.D.; Barker, J.; Roderick, P.J.; Yuen, H.M.; Shardlow, A.; E Morris, J.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Health-related quality of life, functional impairment and comorbidity in people with mild-to-moderate chronic kidney disease: A cross-sectional study. BMJ Open 2020, 10, e040286. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Multimorbidity: Clinical Assessment and Management (NG56). 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 16 December 2022).
- World Health Organization. World Health Assembly, 69. Multisectoral Action for a Life Course Approach to Healthy Ageing: Draft Global Strategy and Plan of Action on Ageing and Health: Report by the Secretariat. 2016. Available online: https://apps.who.int/iris/handle/10665/252671 (accessed on 16 December 2022).



{kind=link}
{kind=link}
| Total | No EQ-VAS Decline | EQ-VAS Decline | p-Value | |
|---|---|---|---|---|
| N = 1748 | N = 1029 | N = 719 | ||
| Baseline Assessment | ||||
| Sex, female n(%) | 969(55.4%) | 547(53.2%) | 422(58.7%) | 0.022 |
| Age, mean ± SD | 79.9 ± 3.9 | 79.9 ± 3.9 | 80.0 ± 3.9 | 0.631 |
| Education (years), mean ± SD | 11.5 ± 4.9 | 11.3 ± 5.0 | 11.7 ± 4.9 | 0.026 |
| Marital status, widow n(%) | 553(31.6%) | 312(30.3%) | 241(33.5%) | 0.157 |
| BMI, mean ± SD | 27.7 ± 4.3 | 27.4 ± 4.2 | 28.0 ± 4.4 | 0.011 |
| MMSE, mean ± SD | 28.1 ± 2.5 | 28.2 ± 2.5 | 27.9 ± 2.6 | 0.001 |
| Diabetes mellitus, n(%) | 398(22.8%) | 227(22.1%) | 171(23.8%) | 0.398 |
| Hypertension, n(%) | 1314(75.2%) | 770(74.8%) | 544(75.7%) | 0.692 |
| Stroke, n(%) | 94(5.4%) | 61(5.9%) | 33(4.6%) | 0.222 |
| Hip fracture, n(%) | 74(4.2%) | 50(4.9%) | 24(3.3%) | 0.120 |
| COPD, n(%) | 203(11.6%) | 110(10.7%) | 93(12.9%) | 0.149 |
| Osteoporosis, n(%) | 534(30.5%) | 317(30.8%) | 217(30.2%) | 0.780 |
| Parkinson’s disease, n(%) | 26(1.5%) | 16(1.6%) | 10(1.4%) | 0.780 |
| Anemia, n(%) | 296(16.9%) | 169(16.4%) | 127(17.7%) | 0.299 |
| LUTS, n(%) | 493(28.2%) | 273(26.5%) | 220(30.6%) | 0.116 |
| Falls history, n(%) | 521(29.8%) | 313(30.4%) | 208(28.9%) | 0.503 |
| CKD, n(%) | 1111(63.6%) | 664(64.5%) | 447(62.2%) | 0.154 |
| eGFR (mL/min/1.73 m2), mean ± SD | 54.6 ± 14.1 | 54.6 ± 14.1 | 54.7 ± 14.1 | 0.605 |
| CIRS-G score, mean ± SD | 8.3 ± 4.5 | 8.2 ± 4.5 | 8.3 ± 4.4 | 0.624 |
| 5+ prescribed medications, n(%) | 1123(64.2%) | 631(61.3%) | 492(68.4%) | 0.004 |
| GDS-SF score, mean ± SD | 2.5 ± 2.6 | 2.4 ± 2.7 | 2.8 ± 2.4 | 0.000 |
| EQ-5D, mean ± SD | 7.9 ± 3.0 | 7.8 ± 3.1 | 8.0 ± 2.8 | 0.003 |
| EQ-VAS, mean ± SD | 72.0 ± 17.2 | 70.3 ± 18.4 | 74.5 ± 15.0 | 0.000 |
| SPPB score, mean ± SD | 9.0 ± 2.8 | 9.0 ± 2.8 | 9.1 ± 2.6 | 0.836 |
| Balance test, mean ± SD | 3.3 ± 1.1 | 3.2 ± 1.1 | 3.3 ± 1.0 | 0.141 |
| Gait speed test, mean ± SD | 3.3 ± 1.0 | 3.3 ± 1.0 | 3.3 ± 0.9 | 0.671 |
| Chair stand test, mean ± SD | 2.7 ± 1.2 | 2.7 ± 1.2 | 2.6 ± 1.2 | 0.227 |
| Grip strength test, mean ± SD | 25.1 ± 10.1 | 25.7 ± 10.2 | 24.1 ± 9.7 | 0.002 |
| After a two-year follow-up period | ||||
| CKD progression, n(%) | 284(16.3%) | 166(16.1%) | 118(16.4%) | 0.190 |
| Δ eGFR (mL/min/1.73 m2), mean ± SD | −0.1 ± 18.2 | 7.8 ± 14.4 | −11.4 ± 17.0 | 0.360 |
| Δ GDS-SF score, mean ± SD | −0.1 ± 2.5 | −0.2 ± 2.5 | +0.1 ± 2.4 | 0.046 |
| Δ SPPB score, mean ± SD | −0.6 ± 2.3 | −0.5 ± 2.2 | −0.8 ± 2.4 | 0.075 |
| Δ Balance, mean ± SD | −0.1 ± 1.2 | −0.1 ± 1.2 | −0.2 ± 1.2 | 0.029 |
| Δ Gait speed, mean ± SD | −0.2 ± 1.0 | −0.1 ± 0.9 | −0.3 ± 1.0 | 0.034 |
| Δ Chair stand, mean ± SD | −0.1 ± 1.1 | −0.1 ± 1.1 | −0.1 ± 1.2 | 0.512 |
| Δ Grip strength, mean ± SD | −1.1 ± 5.5 | −1.0 ± 4.9 | −1.2 ± 6.2 | 0.837 |
| Independent Variable | Δ eGFR | Δ GDS-SF | Δ SPPB Total Score | Δ SPPB Balance | Δ SPPB Gait | Δ Sit to Stand | Δ Hand Grip |
|---|---|---|---|---|---|---|---|
| Model 1. Only independent variable | 1.01 (0.99–1.02) | 1.06 (1.02–1.10) | 0.95 (0.91–0.99) | 0.92 (0.85–0.99) | 0.89 (0.81–0.99) | 1.03 (0.93–1.13) | 0.99 (0.97–1.01) |
| Model 2. Model 1 adjusted for age and sex | 1.01 (0.99–1.02) | 1.06 (1.02–1.11) | 0.94 (0.91–0.99) | 0.92 (0.85–0.99) | 0.89 (0.80–0.98) | 1.02 (0.92–1.12) | 0.99 (0.97–1.01) |
| Model 3. Model 2 adjusted for educational level, EQ-VAS at baseline, MMSE at baseline, BMI at baseline, GDS-SF at baseline, grip strength at baseline, more than five prescribed medications at baseline | 1.01 (0.99–1.02) | 1.14 (1.09–1.20) | 0.95 (0.91–0.99) | 0.92 (0.84–1.00) | 0.88 (0.78–0.98) | 1.03 (0.93–1.14) | 0.98 (0.96–1.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artzi-Medvedik, R.; Kob, R.; Di Rosa, M.; Lattanzio, F.; Corsonello, A.; Yehoshua, I.; Roller-Wirnsberger, R.E.; Wirnsberger, G.H.; Mattace-Raso, F.U.S.; Tap, L.; et al. Quality of Life and Kidney Function in Older Adults: Prospective Data of the SCOPE Study. J. Clin. Med. 2023, 12, 3959. https://doi.org/10.3390/jcm12123959
Artzi-Medvedik R, Kob R, Di Rosa M, Lattanzio F, Corsonello A, Yehoshua I, Roller-Wirnsberger RE, Wirnsberger GH, Mattace-Raso FUS, Tap L, et al. Quality of Life and Kidney Function in Older Adults: Prospective Data of the SCOPE Study. Journal of Clinical Medicine. 2023; 12(12):3959. https://doi.org/10.3390/jcm12123959
Chicago/Turabian StyleArtzi-Medvedik, Rada, Robert Kob, Mirko Di Rosa, Fabrizia Lattanzio, Andrea Corsonello, Ilan Yehoshua, Regina E. Roller-Wirnsberger, Gerhard H. Wirnsberger, Francesco U. S. Mattace-Raso, Lisanne Tap, and et al. 2023. "Quality of Life and Kidney Function in Older Adults: Prospective Data of the SCOPE Study" Journal of Clinical Medicine 12, no. 12: 3959. https://doi.org/10.3390/jcm12123959