
Maternal Preconception Glucose Homeostasis and Insulin Resistance Are Associated with Singleton and Twin Birthweight of Neonates Conceived by PCOS Women Undergoing IVF/ICSI Cycles
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethics Statement
2.2. Study Population
2.3. IVF Procedures
2.4. Biochemical Assessment
2.5. Pregnancy and Neonatal Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Baseline Reproductive and Clinical Characteristics of the Study Population
3.2. Glucose Metabolism Indicators and Neonatal Birthweight
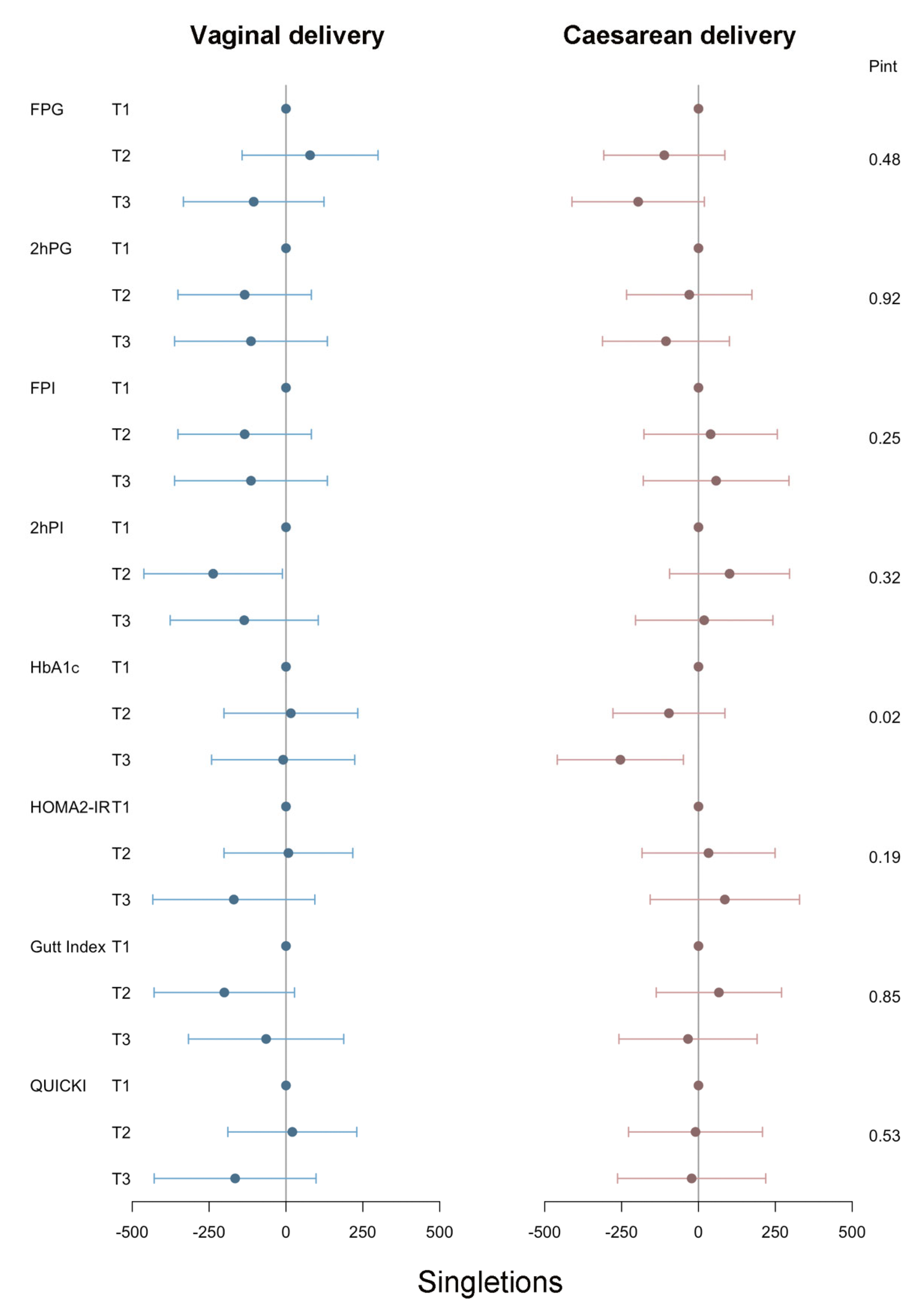
3.3. Stratified Analyses
3.4. Sensitivity Analyses
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Danaei, G.; Finucane, M.M.; Lu, Y.; Singh, G.M.; Cowan, M.J.; Paciorek, C.J.; Lin, J.K.; Farzadfar, F.; Khang, Y.-H.; Stevens, G.A.; et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet 2011, 378, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; McIntyre, H.D.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [PubMed] [Green Version]
- Wei, Y.; Xu, Q.; Yang, H.; Yang, Y.; Wang, L.; Chen, H.; Anderson, C.; Liu, X.; Song, G.; Li, Q.; et al. Preconception diabetes mellitus and adverse pregnancy outcomes in over 6.4 million women: A population-based cohort study in China. PLoS Med. 2019, 16, e1002926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajnik, C.S.; Deshmukh, U.S. Maternal nutrition, intrauterine programming and consequential risks in the offspring. Rev. Endocr. Metab. Disord. 2008, 9, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.; Chik, C. Ethnic differences in antepartum glucose values that predict postpartum dysglycemia and neonatal macrosomia. Diabetes Res. Clin. Pract. 2018, 140, 81–87. [Google Scholar] [CrossRef]
- Wang, Z.; Nagy, R.A.; Groen, H.; Cantineau, A.E.; van Oers, A.M.; van Dammen, L.; Wekker, V.; Roseboom, T.J.; Mol, B.W.; Tietge, U.J.; et al. Preconception insulin resistance and neonatal birth weight in women with obesity: Role of bile acids. Reprod. Biomed. Online 2021, 43, 931–939. [Google Scholar] [CrossRef]
- Bin Chen, B.; Du, Y.-R.; Zhu, H.; Sun, M.-L.; Wang, C.; Cheng, Y.; Pang, H.; Ding, G.; Gao, J.; Tan, Y.; et al. Maternal inheritance of glucose intolerance via oocyte TET3 insufficiency. Nature 2022, 605, 761–766. [Google Scholar] [CrossRef]
- Ye, W.; Luo, C.; Huang, J.; Li, C.; Liu, Z.; Liu, F. Gestational diabetes mellitus and adverse pregnancy outcomes: Systematic review and meta-analysis. BMJ 2022, 377, e067946. [Google Scholar] [CrossRef]
- Joham, A.E.; Norman, R.J.; Stener-Victorin, E.; Legro, R.S.; Franks, S.; Moran, L.J.; Boyle, J.; Teede, H.J. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022, 10, 668–680. [Google Scholar] [CrossRef]
- Wang, C.; Wu, W.; Yang, H.; Ye, Z.; Zhao, Y.; Liu, J.; Mu, L. Mendelian randomization analyses for PCOS: Evidence, opportunities, and challenges. Trends Genet. 2022, 38, 468–482. [Google Scholar] [CrossRef]
- Bjercke, S.; Dale, P.O.; Tanbo, T.; Storeng, R.; Ertzeid, G.; Åbyholm, T. Impact of insulin resistance on pregnancy complications and outcome in women with polycystic ovary syndrome. Gynecol. Obstet. Investig. 2002, 54, 94–98. [Google Scholar] [CrossRef]
- Scholl, T.O.; Chen, X.; Gaughan, C.; Smith, W.K. Influence of maternal glucose level on ethnic differences in birth weight and pregnancy outcome. Am. J. Epidemiol. 2002, 156, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Zhang, H.; Dong, L.; Yu, S.; Guo, Z.; Hsu-Hage, B.H.-H. The effect of glucose levels on fetal birth weight: A study of Chinese gravidas in Tianjin, China. J. Diabetes Complicat. 2004, 18, 37–41. [Google Scholar] [CrossRef]
- Beksac, M.S.; Tanacan, A.; Hakli, D.A.; Ozyuncu, O. Use of the 50-g glucose challenge test to predict excess delivery weight. Int. J. Gynecol. Obstet. 2018, 142, 61–65. [Google Scholar] [CrossRef]
- Chivese, T.; Haynes, M.C.; van Zyl, H.; Kyriacos, U.; Levitt, N.S.; Norris, S.A. The influence of maternal blood glucose during pregnancy on weight outcomes at birth and preschool age in offspring exposed to hyperglycemia first detected during pregnancy, in a South African cohort. PLoS ONE 2021, 16, e0258894. [Google Scholar] [CrossRef]
- Weedon, M.N.; Clark, V.J.; Qian, Y.; Ben-Shlomo, Y.; Timpson, N.; Ebrahim, S.; Lawlor, D.A.; Pembrey, M.E.; Ring, S.; Wilkin, T.J.; et al. A common haplotype of the glucokinase gene alters fasting glucose and birth weight: Association in six studies and population-genetics analyses. Am. J. Hum. Genet. 2006, 79, 991–1001. [Google Scholar] [CrossRef] [Green Version]
- Alves, L.N.R.; Pereira, M.; dos Santos, J.A.; Santos, E.D.V.W.D.; de Carvalho, G.Q.; Santana, J.D.M.; Tavares, E.A.; Fernandes, M.D.B.; dos Santos, D.B.; Louro, I.D. Investigation of maternal polymorphisms in genes related to glucose homeostasis and the influence on birth weight: A cohort study. J. Pediatr. 2022, 98, 296–302. [Google Scholar] [CrossRef]
- Widness, J.A.; Schwartz, H.C.; Thompson, D.; King, K.C.; Kahn, C.B.; Oh, W.; Schwartz, R. Glycohemoglobin (HbAIc): A predictor of birth weight in infants of diabetic mothers. J. Pediatr. 1978, 92, 8–12. [Google Scholar] [CrossRef]
- Yamashita, H.; Yasuhi, I.; Fukuda, M.; Kugishima, Y.; Yamauchi, Y.; Kuzume, A.; Hashimoto, T.; Sugimi, S.; Umezaki, Y.; Suga, S.; et al. The association between maternal insulin resistance in mid-pregnancy and neonatal birthweight in uncomplicated pregnancies. Endocr. J. 2014, 61, 1019–1024. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.M.; Green, E.S.; Tan, T.C.Y.; Gonzalez, M.B.; Rumbold, A.R.; Hull, M.L.; Norman, R.J.; Packer, N.H.; Robertson, S.A.; Thompson, J.G. Periconception onset diabetes is associated with embryopathy and fetal growth retardation, reproductive tract hyperglycosylation and impaired immune adaptation to pregnancy. Sci. Rep. 2018, 8, 2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Committee on Obstetric Practice American Institute of Ultrasound in Medicine Society for Maternal–Fetal Medicine. Committee Opinion No 700: Methods for Estimating the Due Date. Obstet. Gynecol. 2017, 129, e150–e154. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Gao, H.; Chi, H.; Zeng, L.; Xiao, W.; Wang, Y.; Li, R.; Liu, P.; Wang, C.; Tian, Q.; et al. Effect of Levothyroxine on Miscarriage among Women with Normal Thyroid Function and Thyroid Autoimmunity Undergoing In Vitro Fertilization and Embryo Transfer: A Randomized Clinical Trial. JAMA 2017, 318, 2190–2198. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Gutt, M.; Davis, C.L.; Spitzer, S.B.; Llabre, M.M.; Kumar, M.; Czarnecki, E.M.; Schneiderman, N.; Skyler, J.S.; Marks, J.B. Validation of the insulin sensitivity index (ISI (0, 120)): Comparison with other measures. Diabetes Res. Clin. Pract. 2000, 47, 177–184. [Google Scholar] [CrossRef]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef]
- Zong, X.; Wang, H.; Yang, L.; Guo, Y.; Zhao, M.; Magnussen, C.G.; Xi, B. Maternal Pre-pregnancy Body Mass Index Categories and Infant Birth Outcomes: A Population-Based Study of 9 Million Mother–Infant Pairs. Front. Nutr. 2022, 9, 789833. [Google Scholar] [CrossRef]
- Greenland, S. Modeling and variable selection in epidemiologic analysis. Am. J. Public Health 1989, 79, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Farrar, D.; Simmonds, M.; Bryant, M.; Sheldon, T.A.; Tuffnell, D.; Golder, S.; Dunne, F.; Lawlor, D.A. Hyperglycaemia and risk of adverse perinatal outcomes: Systematic review and meta-analysis. BMJ 2016, 354, i4694. [Google Scholar] [CrossRef] [Green Version]
- Dashe, J.S.; Nathan, L.; McIntire, D.D.; Leveno, K.J. Correlation between amniotic fluid glucose concentration and amniotic fluid volume in pregnancy complicated by diabetes. Am. J. Obstet. Gynecol. 2000, 182, 901–904. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhao, R.; Lyu, Y.; Shi, H.; Ye, W.; Tan, Y.; Li, R.; Xu, Y. Serum and Amniotic Fluid Metabolic Profile Changes in Response to Gestational Diabetes Mellitus and the Association with Maternal–Fetal Outcomes. Nutrients 2021, 13, 3644. [Google Scholar] [CrossRef]
- Xu, Z.-M.; Wu, L.-F. Correlation between amniotic fluid glucose concentration and amniotic fluid volume and neonatal birth weight in pregnancy complicated by gestational diabetes mellitus. Zhonghua Fu Chan Ke Za Zhi 2006, 41, 724–748. [Google Scholar]
- Tuuli, M.G.; Stout, M.J.; Macones, G.A.; Cahill, A.G.; Temming, L.A. Maternal and Perinatal Outcomes in Women with Insulin Resistance. Am. J. Perinatol. 2016, 33, 776–780. [Google Scholar] [CrossRef] [Green Version]
- Bi, J.; Ji, C.; Wu, Y.; Wu, M.; Liu, Y.; Song, L.; Khatiwada, S.U.; Yang, S.; Li, B.; Wang, Y.; et al. Association Between Maternal Normal Range HbA1c Values and Adverse Birth Outcomes. J. Clin. Endocrinol. Metab. 2020, 105, e2185–e2191. [Google Scholar] [CrossRef]
- Weedon, M.N.; Frayling, T.M.; Shields, B.; Knight, B.; Turner, T.; Metcalf, B.S.; Voss, L.; Wilkin, T.J.; McCarthy, A.; Ben-Shlomo, Y.; et al. Genetic regulation of birth weight and fasting glucose by a common polymorphism in the islet cell promoter of the glucokinase gene. Diabetes 2005, 54, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Kakoly, N.S.; Earnest, A.; Teede, H.J.; Moran, L.J.; Joham, A.E. The Impact of Obesity on the Incidence of Type 2 Diabetes Among Women with Polycystic Ovary Syndrome. Diabetes Care 2019, 42, 560–567. [Google Scholar] [CrossRef] [Green Version]
- Zhu, T.; Cui, J.; Goodarzi, M.O. Polycystic Ovary Syndrome and Risk of Type 2 Diabetes, Coronary Heart Disease, and Stroke. Diabetes 2021, 70, 627–637. [Google Scholar] [CrossRef]
- Zhao, H.; Zhao, Y.; Ren, Y.; Li, M.; Li, T.; Li, R.; Yu, Y.; Qiao, J. Epigenetic regulation of an adverse metabolic phenotype in polycystic ovary syndrome: The impact of the leukocyte methylation of PPARGC1A promoter. Fertil. Steril. 2017, 107, 467–474.e5. [Google Scholar] [CrossRef] [Green Version]
- Ruth, K.S.; Day, F.; Tyrrell, J.; Thompson, D.J.; Wood, A.R.; Mahajan, A.; Beaumont, R.N.; Wittemans, L.; Martin, S.; Busch, A.S.; et al. Using human genetics to understand the disease impacts of testosterone in men and women. Nat. Med. 2020, 26, 252–258. [Google Scholar] [CrossRef]
- Baillargeon, J.-P.; Carpentier, A. Role of insulin in the hyperandrogenemia of lean women with polycystic ovary syndrome and normal insulin sensitivity. Fertil. Steril. 2007, 88, 886–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: An update on mechanisms and implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.; Gathercole, L.; Capper, F.; Arlt, W.; Tomlinson, J. Effect of insulin on AKR1C3 expression in female adipose tissue: In-vivo and in-vitro study of adipose androgen generation in polycystic ovary syndrome. Lancet 2015, 385 (Suppl. 1), S16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.; Yun, C.; Sun, L.; Xia, J.; Wu, Q.; Wang, Y.; Wang, L.; Zhang, Y.; Liang, X.; Wang, L.; et al. Gut microbiota–bile acid–interleukin-22 axis orchestrates polycystic ovary syndrome. Nat. Med. 2019, 25, 1225–1233. [Google Scholar] [CrossRef]
- Yang, Y.-L.; Zhou, W.-W.; Wu, S.; Tang, W.-L.; Wang, Z.-W.; Zhou, Z.-Y.; Li, Z.-W.; Huang, Q.-F.; He, Y.; Zhou, H.-W. Intestinal Flora is a Key Factor in Insulin Resistance and Contributes to the Development of Polycystic Ovary Syndrome. Endocrinology 2021, 162, bqab118. [Google Scholar] [CrossRef]
- Ou, X.-H.; Li, S.; Wang, Z.-B.; Li, M.; Quan, S.; Xing, F.; Guo, L.; Chao, S.-B.; Chen, Z.; Liang, X.-W.; et al. Maternal insulin resistance causes oxidative stress and mitochondrial dysfunction in mouse oocytes. Hum. Reprod. 2012, 27, 2130–2145. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.-H.; Qian, W.-P.; Qi, S.-T.; Ge, Z.-J.; Min, L.-J.; Zhu, X.-L.; Huang, X.; Liu, J.-P.; Ouyang, Y.-C.; Hou, Y.; et al. Maternal diabetes causes abnormal dynamic changes of endoplasmic reticulum during mouse oocyte maturation and early embryo development. Reprod. Biol. Endocrinol. 2013, 11, 31. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Jing, Y.; Dong, M.-Z.; Fan, L.-H.; Li, Q.-N.; Wang, Z.-B.; Hou, Y.; Schatten, H.; Zhang, C.-L.; Sun, Q.-Y. Type 1 diabetes affects zona pellucida and genome methylation in oocytes and granulosa cells. Mol. Cell. Endocrinol. 2020, 500, 110627. [Google Scholar] [CrossRef]
- Li, L.; Wu, C.-S.; Hou, G.-M.; Dong, M.-Z.; Wang, Z.-B.; Hou, Y.; Schatten, H.; Zhang, G.-R.; Sun, Q.-Y. Type 2 diabetes increases oocyte mtDNA mutations which are eliminated in the offspring by bottleneck effect. Reprod. Biol. Endocrinol. 2018, 16, 110. [Google Scholar] [CrossRef]
- Jiang, G.; Zhang, G.; An, T.; He, Z.; Kang, L.; Yang, X.; Gu, Y.; Zhang, D.; Wang, Y.; Gao, S. Effect of Type I Diabetes on the Proteome of Mouse Oocytes. Cell. Physiol. Biochem. 2016, 39, 2320–2330. [Google Scholar] [CrossRef]
- Ma, J.-Y.; Li, M.; Ge, Z.-J.; Luo, Y.; Ou, X.-H.; Song, S.; Tian, D.; Yang, J.; Zhang, B.; Ou-Yang, Y.-C.; et al. Whole transcriptome analysis of the effects of type i diabetes on mouse oocytes. PLoS ONE 2012, 7, e41981. [Google Scholar] [CrossRef]
- Ratchford, A.M.; Chang, A.S.; Chi, M.M.-Y.; Sheridan, R.; Moley, K.H. Maternal diabetes adversely affects AMP-activated protein kinase activity and cellular metabolism in murine oocytes. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E1198–E1206. [Google Scholar] [CrossRef]
- Colton, S.A.; Pieper, G.M.; Downs, S.M. Altered meiotic regulation in oocytes from diabetic mice. Biol. Reprod. 2002, 67, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Frolova, A.I.; Purcell, S.; Adastra, K.; Schoeller, E.; Chi, M.M.; Schedl, T.; Moley, K.H. Mitochondrial dysfunction and apoptosis in cumulus cells of type i diabetic mice. PLoS ONE 2010, 5, e15901. [Google Scholar] [CrossRef] [Green Version]
- Xin, Y.; Jin, Y.; Ge, J.; Huang, Z.; Han, L.; Li, C.; Wang, D.; Zhu, S.; Wang, Q. Involvement of SIRT3-GSK3β deacetylation pathway in the effects of maternal diabetes on oocyte meiosis. Cell Prolif. 2021, 54, e12940. [Google Scholar] [CrossRef]
- Nafiye, Y.; Sevtap, K.; Muammer, D.; Emre, O.; Senol, K.; Leyla, M. The effect of serum and intrafollicular insulin resistance parameters and homocysteine levels of nonobese, nonhyperandrogenemic polycystic ovary syndrome patients on in vitro fertilization outcome. Fertil. Steril. 2010, 93, 1864–1869. [Google Scholar] [CrossRef]
- He, Y.; Lu, Y.; Zhu, Q.; Wang, Y.; Lindheim, S.R.; Qi, J.; Li, X.; Ding, Y.; Shi, Y.; Wei, D.; et al. Influence of metabolic syndrome on female fertility and in vitro fertilization outcomes in PCOS women. Am. J. Obstet. Gynecol. 2019, 221, 138.e1–138.e12. [Google Scholar] [CrossRef]
- Wang, W.; Tang, X.; Jiang, Q.; Niu, Y.; Wang, Z.; Wei, D. Risk factors for clinical pregnancy loss after IVF in women with PCOS. Reprod. Biomed. Online 2022, 46, 107–114. [Google Scholar] [CrossRef]
- Chen, L.; Chen, X.-W.; Huang, X.; Song, B.-L.; Wang, Y.; Wang, Y. Regulation of glucose and lipid metabolism in health and disease. Sci. China Life Sci. 2019, 62, 1420–1458. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, K.; Hao, X.; Chen, L.; Liu, Z.; Wang, C. Causal Graph Among Serum Lipids and Glycemic Traits: A Mendelian Randomization Study. Diabetes 2022, 71, 1818–1826. [Google Scholar] [CrossRef]
- Abascal-Saiz, A.; Fuente-Luelmo, E.; Haro, M.; de la Calle, M.; Ramos-Álvarez, M.P.; Perdomo, G.; Bartha, J.L. Placental Compartmentalization of Lipid Metabolism: Implications for Singleton and Twin Pregnancies. Reprod. Sci. 2021, 28, 1150–1160. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Singletons | Twins | P a | |
|---|---|---|---|---|
| N = 190 | N = 79 | |||
| Age, years | 31 (28–33) | 30 (28–32) | 0.21 | |
| Preconceptional BMI, kg/m2 | 25.1 (22.1–28.5) | 24.6 (22.3–27.8) | 0.95 | |
| AFC, n | 17 (13–22) | 17 (13–24) | 0.37 | |
| AMH, ng/mL | 5.5 (3.6–7.8) | 5.6 (3.6–9.3) | 0.52 | |
| Duration of infertility, years | 3 (2–5) | 3 (2–5) | 0.53 | |
| FPG, mmol/L | 4.9 (4.6–5.2) | 4.8 (4.5–5.1) | 0.44 | |
| 2hPG, mmol/L | 6.7 (5.6–8) | 6.6 (5.7–7.8) | 0.84 | |
| FPI, uIU/ml | 11.7 (8.1–17.2) | 11.9 (7.6–16.4) | 0.64 | |
| 2hPI, uIU/ml | 66.9 (41.8–113.8) | 67.8 (39.1–123.7) | 0.98 | |
| HbA1c, % | 5.4 (5.2–5.7) | 5.4 (5.3–5.6) | 0.68 | |
| HOMA2-IR | 1.3 (0.9–1.9) | 1.3 (0.8–1.8) | 0.74 | |
| Gutt index | 65.9 (54.1–85.4) | 66.7 (52.6, 81.9) | 0.98 | |
| QUICKI | 0.33 (0.31–0.35) | 0.33 (0.31–0.35) | 0.39 | |
| Infertility type | Primary | 143 (75.3%) | 65 (82.3%) | 0.21 |
| Secondary | 47 (24.7%) | 14 (17.7%) | ||
| Ovulation induction protocol | Stimulation cycle | 182 (95.8%) | 77 (97.5%) | 0.73 |
| Minimal-stimulation cycle | 8 (4.2%) | 2 (2.5%) | ||
| Ovarian stimulation regimen | GnRH antagonist | 148 (77.9%) | 59 (74.7%) | 0.32 |
| Long GnRHa | 41 (21.6%) | 18 (22.8%) | ||
| Others b | 1 (0.5%) | 2 (2.5%) | ||
| Insemination technique | IVF | 147 (77.4%) | 58 (73.4%) | 0.49 |
| ICSI | 43 (22.6%) | 21 (26.6%) | ||
| Timing of embryo transfer | Day 3 | 180 (94.7%) | 79 (100.0%) | 0.11 |
| Day 5 | 7 (3.7%) | 0 (0.0%) | ||
| Day 6 | 3 (1.6%) | 0 (0.0%) | ||
| Transferred embryo number, n | 1 | 24 (12.6%) | 0 (0.0%) | <0.01 |
| 2 | 166 (87.4%) | 79 (100.0%) | ||
| Gestational age, weeks | <37 | 25 (13.2%) | 43 (54.4%) | <0.001 |
| 37–42 | 165 (86.8%) | 36 (45.6%) | ||
| Delivery mode | Vaginal delivery | 90 (47.4%) | 9 (11.4%) | <0.001 |
| Caesarean | 100 (52.6%) | 70 (88.6%) | ||
| Neonatal sex | Male | 98 (51.6%) | 120 (75.9%) | <0.001 |
| Female | 71 (48.4%) | 59 (24.1%) | ||
| Birthweight, g | <2500 | 13 (6.8%) | 78 (49.4%) | <0.001 |
| 2500–4000 | 167 (87.9%) | 80 (50.6%) | ||
| ≥4000 | 10 (5.3%) | 0 (0.0%) | ||
| Glucose Metabolism Indicators | β (95% CI) | |
|---|---|---|
| Singletons b | Twins c | |
| N = 190 | N = 79 | |
| FPG | ||
| T1 | Ref. | Ref. |
| T2 | –60.30 (–204.38, 83.75) | –34.86 (–183.44, 113.70) |
| T3 | –161.30 (–316.02, –6.52) | –48.13 (–193.74, 97.50) |
| p for trend | 0.04 | 0.49 |
| 2hPG | ||
| T1 | Ref. | Ref. |
| T2 | –105.10 (–252.17, 42.00) | 113.31 (–27.58, 254.20) |
| T3 | –139.80 (–297.65, 18.10) | –68.91 (–224.15, 86.30) |
| p for trend | 0.08 | 0.44 |
| FPI | ||
| T1 | Ref. | Ref. |
| T2 | 22.40 (–131.24, 176.00) | –13.46 (–177.19, 150.30) |
| T3 | –70.40 (–242.50, 101.70) | –74.70 (–228.99, 79.60) |
| p for trend | 0.42 | 0.35 |
| 2hPI | ||
| T1 | Ref. | Ref. |
| T2 | –74.00 (–220.76, 72.80) | 113.05 (–24.87, 251.00) |
| T3 | –64.60 (–228.57, 99.40) | 71.46 (–76.82, 219.70) |
| p for trend | 0.41 | 0.30 |
| HbA1c | ||
| T1 | Ref. | Ref. |
| T2 | –50.90 (–191.54, 89.70) | 2.10 (–129.80, 134.00) |
| T3 | –165.60 (–318.76, –12.40) | 181.39 (8.60, 354.20) |
| p for trend | 0.04 | 0.07 |
| HOMA2-IR | ||
| T1 | Ref. | Ref. |
| T2 | 2.39 (–150.00, 154.70) | –67.49 (–230.66, 95.70) |
| T3 | –49.02 (–228.00, 130.10) | –22.90 (–177.09, 131.30) |
| p for trend | 0.58 | 0.71 |
| Gutt Index | ||
| T3 | Ref. | Ref. |
| T2 | –89.99 (–241.56, 61.60) | 126.38 (–15.69, 268.50) |
| T1 | –89.46 (–257.52, 78.60) | –56.93 (–200.07, 86.20) |
| p for trend | 0.28 | 0.58 |
| QUICKI | ||
| T3 | Ref. | Ref. |
| T2 | –2.73 (–154.94, 149.50) | –35.11 (–208.07, 137.80) |
| T1 | –102.39 (–280.11, 75.30) | –69.03 (–221.26, 83.20) |
| p for trend | 0.27 | 0.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, H.; Guo, Y.; Chen, L.; Shi, H.; Huang, N.; Chi, H.; Yang, R.; Long, X.; Qiao, J. Maternal Preconception Glucose Homeostasis and Insulin Resistance Are Associated with Singleton and Twin Birthweight of Neonates Conceived by PCOS Women Undergoing IVF/ICSI Cycles. J. Clin. Med. 2023, 12, 3863. https://doi.org/10.3390/jcm12113863
Jiang H, Guo Y, Chen L, Shi H, Huang N, Chi H, Yang R, Long X, Qiao J. Maternal Preconception Glucose Homeostasis and Insulin Resistance Are Associated with Singleton and Twin Birthweight of Neonates Conceived by PCOS Women Undergoing IVF/ICSI Cycles. Journal of Clinical Medicine. 2023; 12(11):3863. https://doi.org/10.3390/jcm12113863
Chicago/Turabian StyleJiang, Huahua, Yaxin Guo, Lixue Chen, Huifeng Shi, Ning Huang, Hongbin Chi, Rui Yang, Xiaoyu Long, and Jie Qiao. 2023. "Maternal Preconception Glucose Homeostasis and Insulin Resistance Are Associated with Singleton and Twin Birthweight of Neonates Conceived by PCOS Women Undergoing IVF/ICSI Cycles" Journal of Clinical Medicine 12, no. 11: 3863. https://doi.org/10.3390/jcm12113863