
Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Data
2.2. Clinical Management
2.3. Antibiotic Therapy
2.4. Methods for Pathogen Detection
2.5. Microbiological Assessment
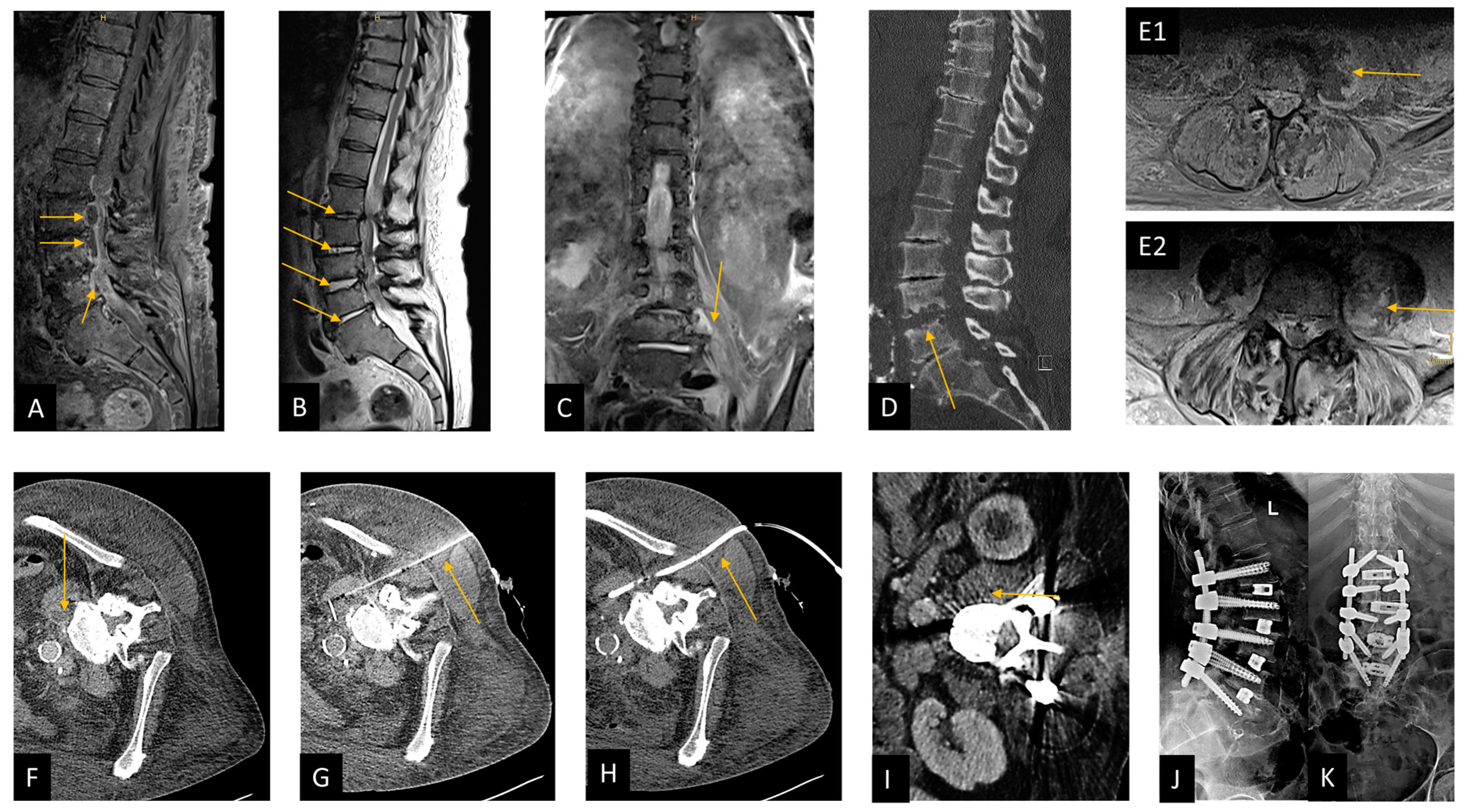
2.6. Case Presentation
2.7. Statistical Analysis
3. Results
3.1. Demographics and Baseline Characteristics
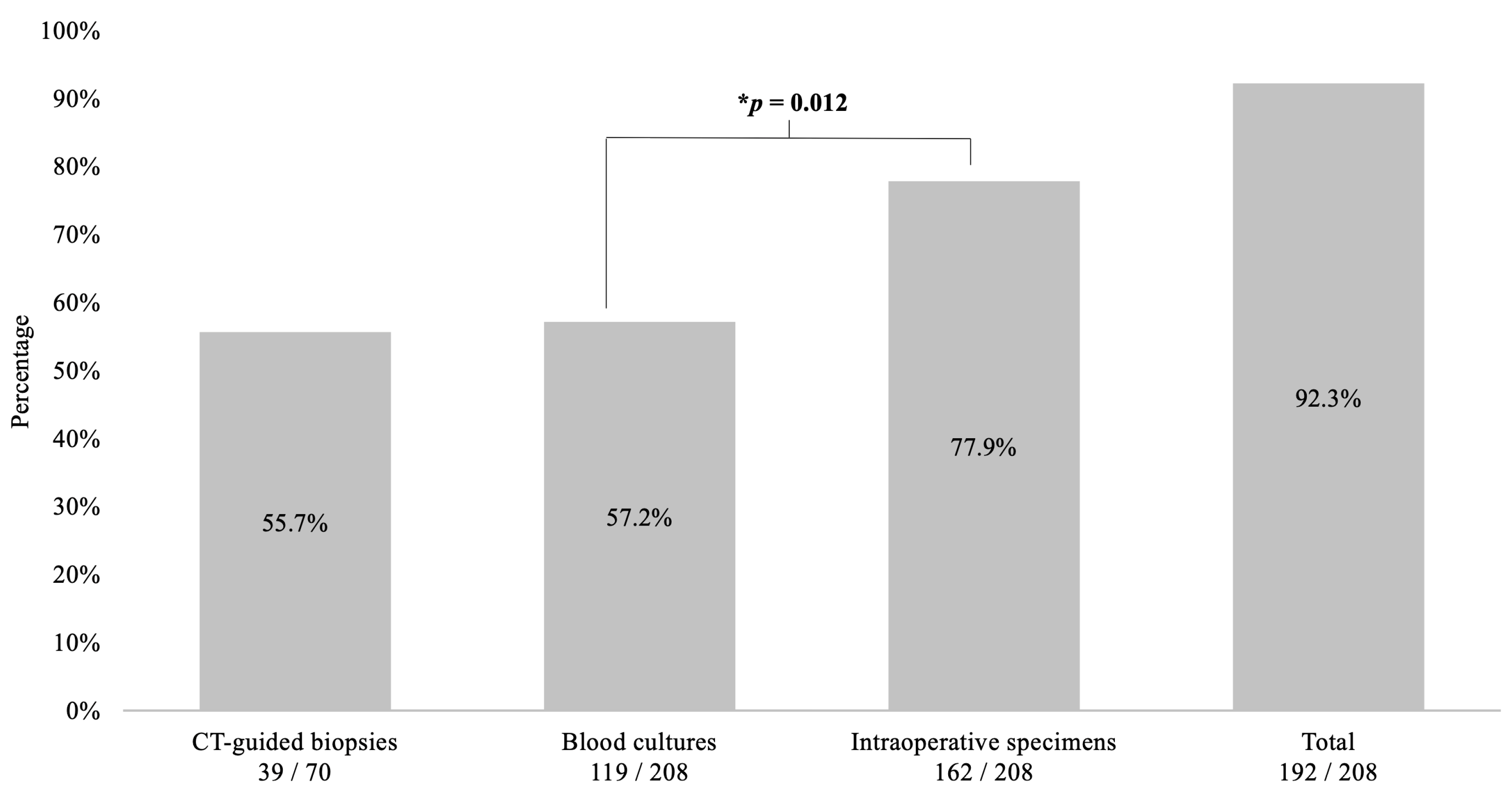
3.2. Diagnostic Sensitivity of Procedures
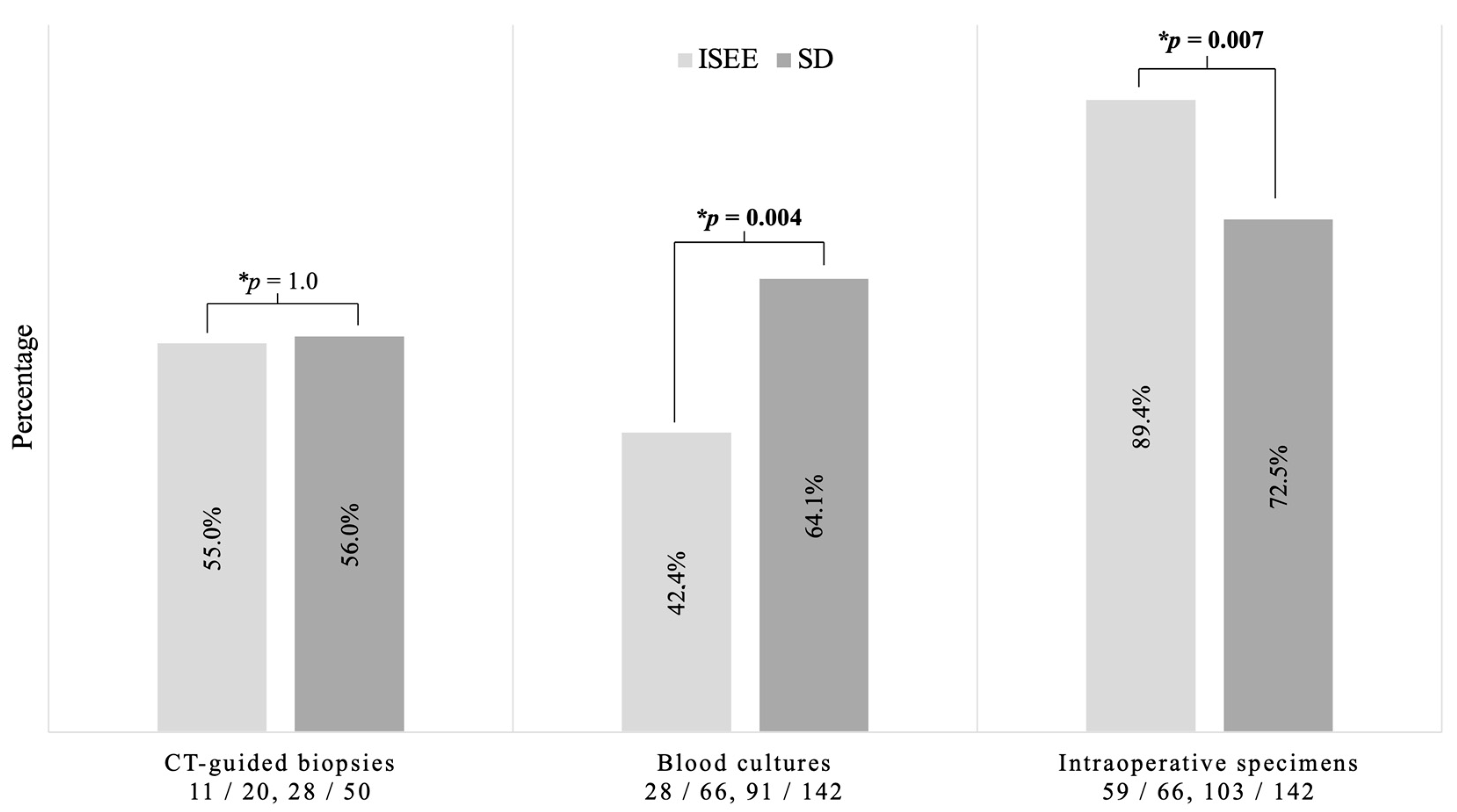
3.3. Diagnostic Sensitivity in SD and ISEE
3.4. Sensitivity under Ongoing Empiric Antibiotic Therapy
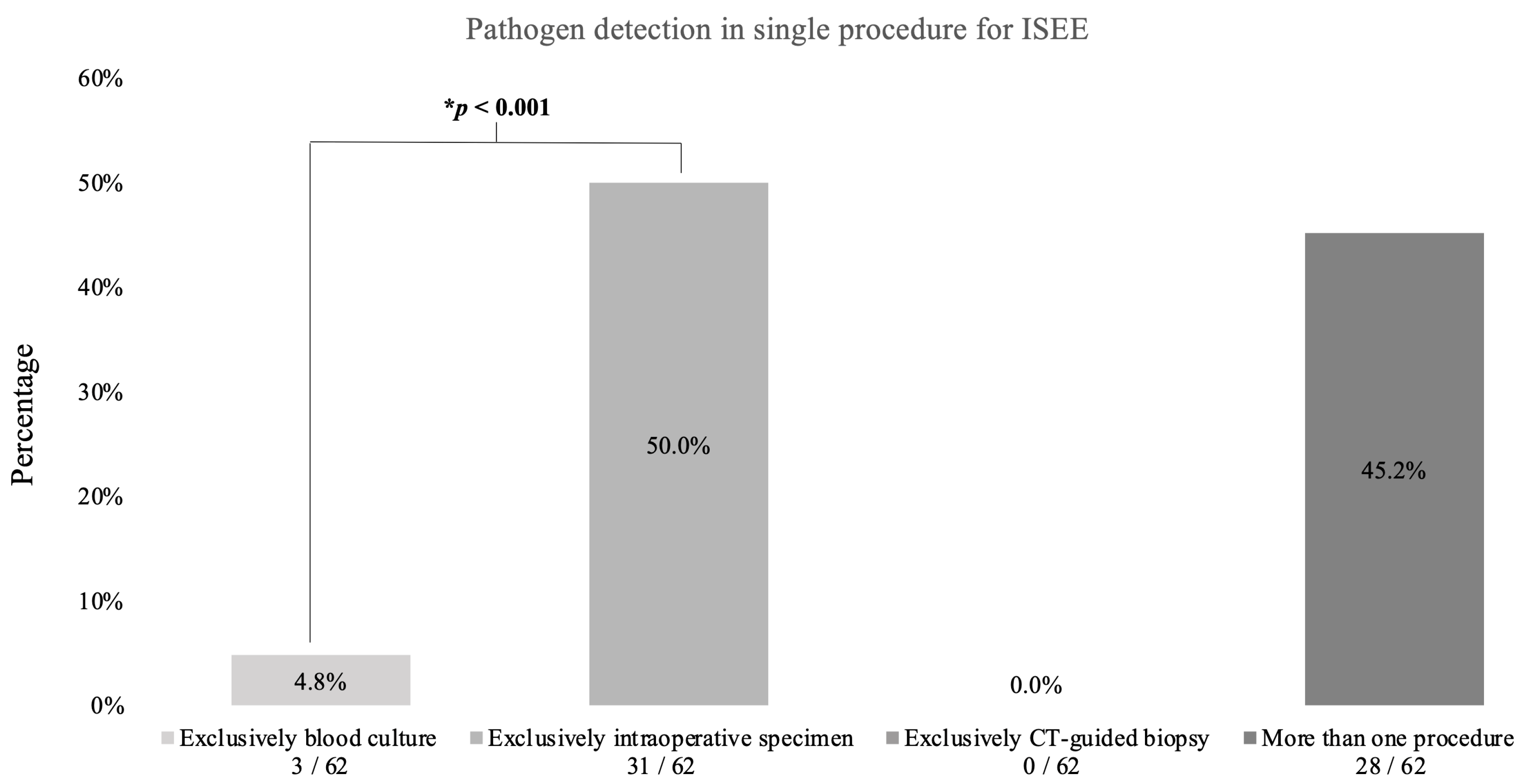
3.5. Sensitivity of Single Procedure in SD and ISEE Patient Treated with EAT or TAT
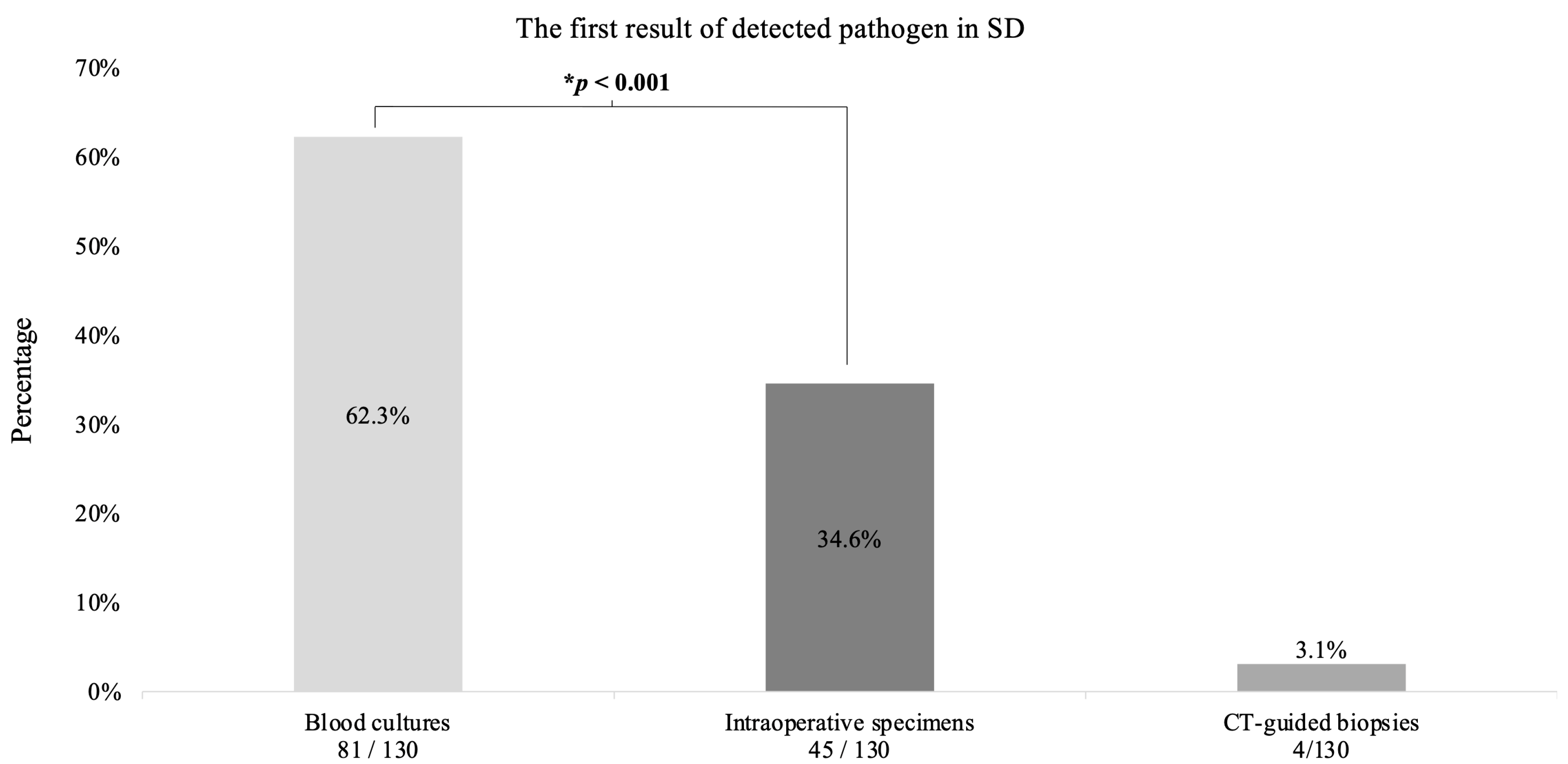
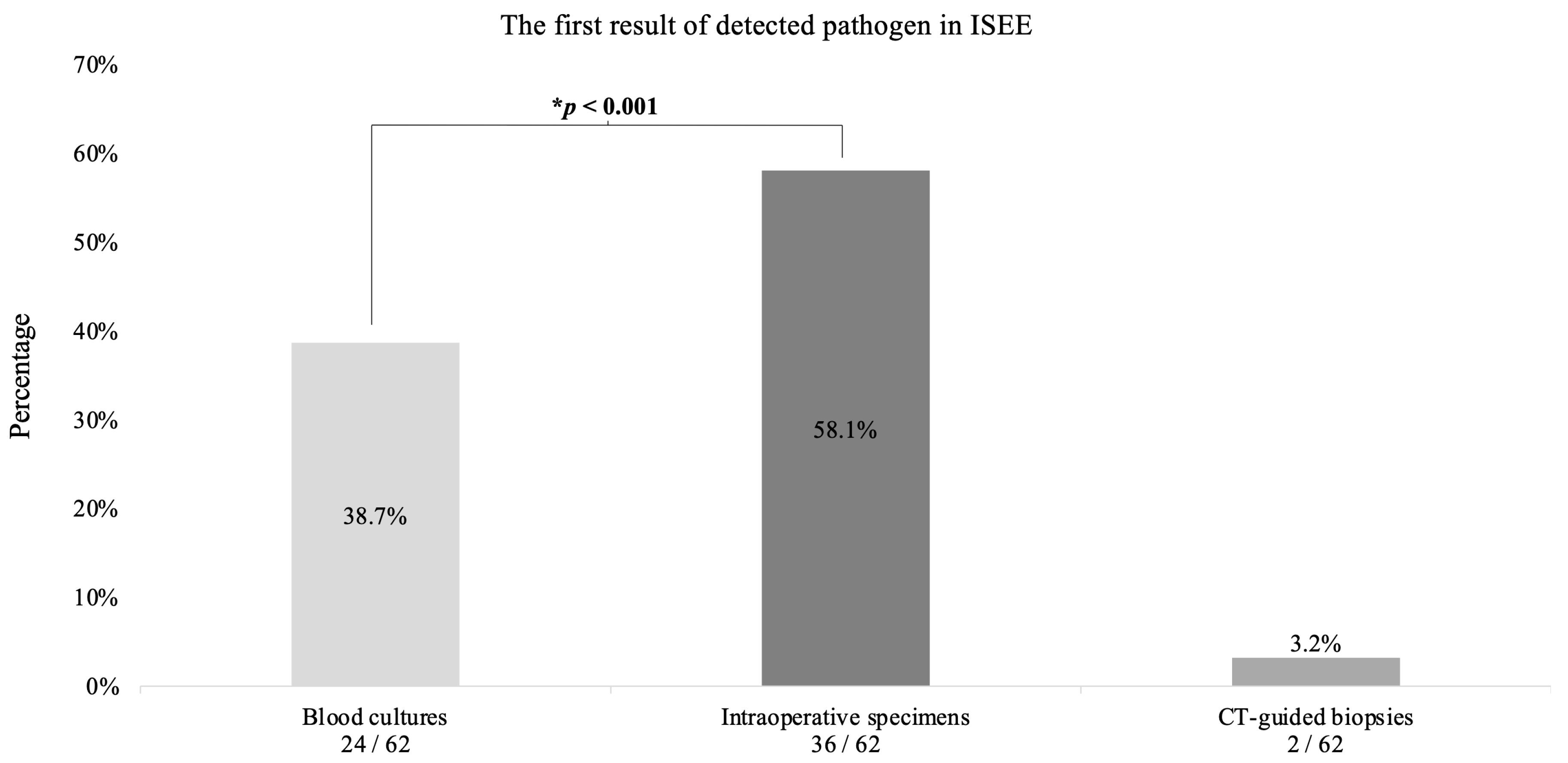
3.6. The First Result of Detected Pathogen in SD and ISEE Treated with EAT or TAT
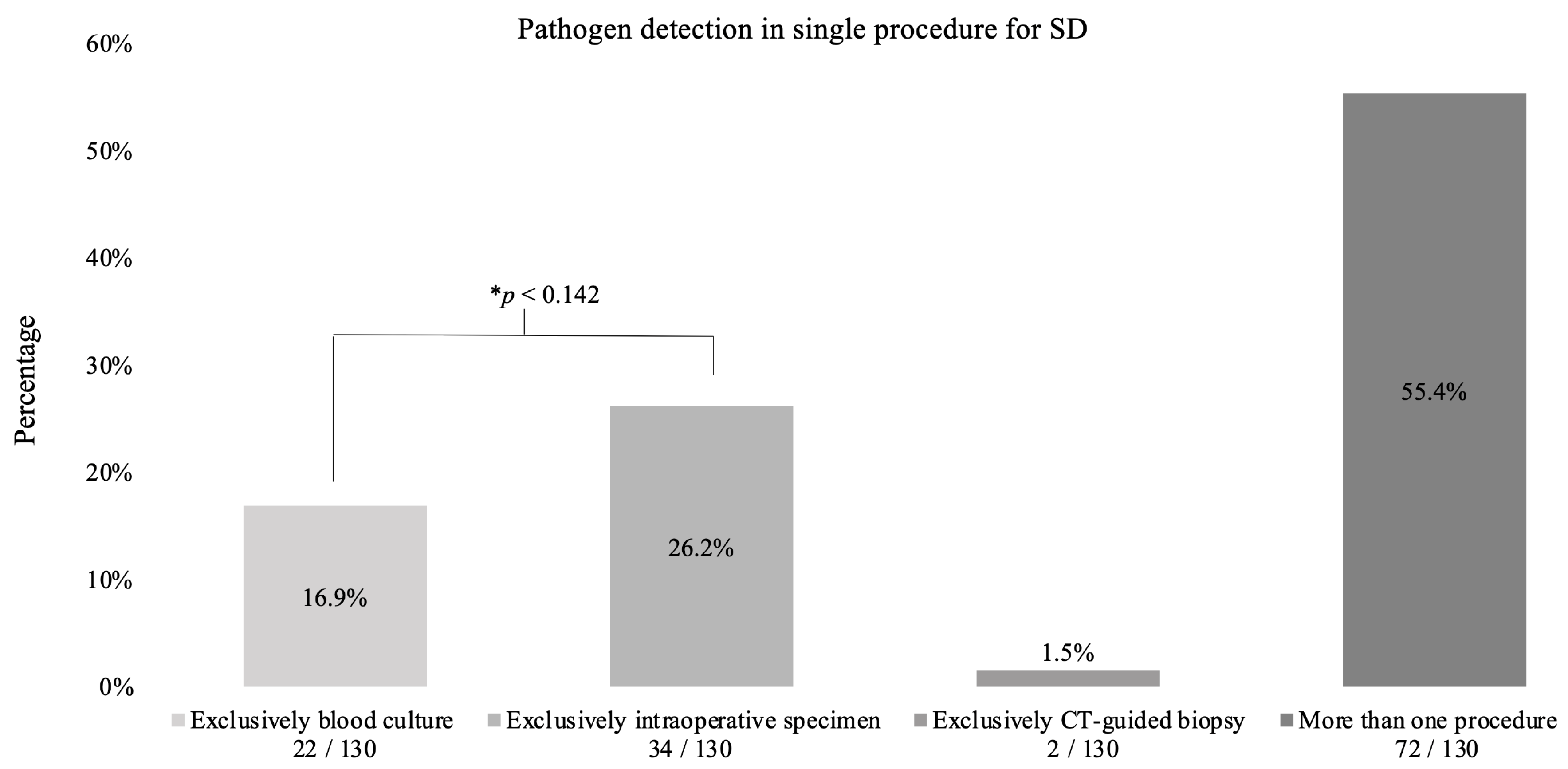
3.7. The role of Each Procedure in Pathogen Detection in Both Entities
3.7.1. Spondylodiscitis
3.7.2. Isolated Spinal Epidural Empyema
3.8. The First Result of Antibiogram and Resistogram from All Procedures
3.8.1. Spondylodiscitis
3.8.2. Isolated Spinal Epidural Empyema
4. Discussion
Limitations and Strengths of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknolegdment
Conflicts of Interest
References
- Butler, J.S.; Shelly, M.J.; Timlin, M.; Powderly, W.G.; O’Byrne, J.M. Nontuberculous pyogenic spinal infection in adults: A 12-year experience from a tertiary referral center. Spine 2006, 31, 2695–2700. [Google Scholar] [CrossRef] [PubMed]
- Frangen, T.M.; Kalicke, T.; Gottwald, M.; Andereya, S.; Andress, H.J.; Russe, O.J.; Muller, E.J.; Muhr, G.; Schinkel, C. Die operative Therapie der Spondylodiszitis. Unfallchirurg 2006, 109, 743–753. [Google Scholar] [CrossRef]
- Tsiodras, S.; Falagas, M.E. Clinical assessment and medical treatment of spine infections. Clin. Orthop. Relat. Res. 2006, 444, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Herren, C.; Jung, N.; Pishnamaz, M.; Breuninger, M.; Siewe, J.; Sobottke, R. Spondylodiscitis: Diagnosis and Treatment Options. Dtsch. Arztebl. Int. 2017, 114, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Zarghooni, K.; Rollinghoff, M.; Sobottke, R.; Eysel, P. Treatment of spondylodiscitis. Int. Orthop. 2012, 36, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Rosc-Bereza, K.; Arkuszewski, M.; Ciach-Wysocka, E.; Boczarska-Jedynak, M. Spinal epidural abscess: Common symptoms of an emergency condition. A case report. Neuroradiol. J. 2013, 26, 464–468. [Google Scholar] [CrossRef]
- Quack, V.; Hermann, I.; Rath, B.; Dietrich, K.; Spreckelsen, C.; Luring, C.; Arbab, D.; Mueller, C.A.; Shousha, M.; Clusmann, H.; et al. Current treatment strategies for spondylodiscitis in surgical clinics in Germany. Z. Orthop. Unfall 2014, 152, 577–583. [Google Scholar] [CrossRef]
- Rustemi, O.; Raneri, F.; Alvaro, L.; Gazzola, L.; Beggio, G.; Rossetto, L.; Cervellini, P. Single-approach vertebral osteosynthesis in the treatment of spinal osteolysis by spondylodiscitis. Neurosurg. Focus. 2019, 46, E9. [Google Scholar] [CrossRef]
- Decker, S.; Schroder, B.M.; Stubig, T.; Sehmisch, S. Common infectious challenges of the thoracic and lumbar spine: Spondylodiscitis and postoperative wound infection. Unfallchirurg 2022, 125, 33–40. [Google Scholar] [CrossRef]
- Cunha, B.A. Osteomyelitis in elderly patients. Clin. Infect. Dis. 2002, 35, 287–293. [Google Scholar] [CrossRef]
- Nagashima, H.; Tanishima, S.; Tanida, A. Diagnosis and management of spinal infections. J. Orthop. Sci. 2018, 23, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Nolla, J.M.; Ariza, J.; Gomez-Vaquero, C.; Fiter, J.; Bermejo, J.; Valverde, J.; Escofet, D.R.; Gudiol, F. Spontaneous pyogenic vertebral osteomyelitis in nondrug users. Semin. Arthritis Rheum. 2002, 31, 271–278. [Google Scholar] [CrossRef]
- Nickerson, E.K.; Sinha, R. Vertebral osteomyelitis in adults: An update. Br. Med. Bull. 2016, 117, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Pingel, A. Spondylodiscitis. Z. Orthop. Unfall 2021, 159, 687–703. [Google Scholar] [CrossRef] [PubMed]
- Fleege, C.; Wichelhaus, T.A.; Rauschmann, M. Systemic and local antibiotic therapy of conservative and operative treatment of spondylodiscitis. Orthopade 2012, 41, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Mylona, E.; Samarkos, M.; Kakalou, E.; Fanourgiakis, P.; Skoutelis, A. Pyogenic vertebral osteomyelitis: A systematic review of clinical characteristics. Semin. Arthritis Rheum. 2009, 39, 10–17. [Google Scholar] [CrossRef]
- McHenry, M.C.; Easley, K.A.; Locker, G.A. Vertebral osteomyelitis: Long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin. Infect. Dis. 2002, 34, 1342–1350. [Google Scholar] [CrossRef]
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M., 3rd; Petermann, G.W.; et al. Executive Summary: 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin. Infect. Dis. 2015, 61, 859–863. [Google Scholar] [CrossRef]
- Chandnani, V.P.; Beltran, J.; Morris, C.S.; Khalil, S.N.; Mueller, C.F.; Burk, J.M.; Bennett, W.F.; Shaffer, P.B.; Vasila, M.S.; Reese, J.; et al. Acute experimental osteomyelitis and abscesses: Detection with MR imaging versus CT. Radiology 1990, 174, 233–236. [Google Scholar] [CrossRef]
- Parikh, R.; Mathai, A.; Parikh, S.; Chandra Sekhar, G.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian. J. Ophthalmol. 2008, 56, 45–50. [Google Scholar] [CrossRef]
- Bernard, L.; Dinh, A.; Ghout, I.; Simo, D.; Zeller, V.; Issartel, B.; Le Moing, V.; Belmatoug, N.; Lesprit, P.; Bru, J.P.; et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: An open-label, non-inferiority, randomised, controlled trial. Lancet 2015, 385, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Fragio Gil, J.J.; Gonzalez Mazario, R.; Salavert Lleti, M.; Roman Ivorra, J.A. Vertebral osteomyelitis: Clinical, microbiological and radiological characteristics of 116 patients. Med. Clin. 2020, 155, 335–339. [Google Scholar] [CrossRef]
- Kehrer, M.; Pedersen, C.; Jensen, T.G.; Hallas, J.; Lassen, A.T. Increased short- and long-term mortality among patients with infectious spondylodiscitis compared with a reference population. Spine J. 2015, 15, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Pola, E.; Taccari, F.; Autore, G.; Giovannenze, F.; Pambianco, V.; Cauda, R.; Maccauro, G.; Fantoni, M. Multidisciplinary management of pyogenic spondylodiscitis: Epidemiological and clinical features, prognostic factors and long-term outcomes in 207 patients. Eur. Spine J. 2018, 27, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Widdrington, J.D.; Emmerson, I.; Cullinan, M.; Narayanan, M.; Klejnow, E.; Watson, A.; Ong, E.L.C.; Schmid, M.L.; Price, D.A.; Schwab, U.; et al. Pyogenic Spondylodiscitis: Risk Factors for Adverse Clinical Outcome in Routine Clinical Practice. Med. Sci. 2018, 6, 96. [Google Scholar] [CrossRef] [PubMed]
- Bateman, J.L.; Pevzner, M.M. Spinal osteomyelitis: A review of 10 years’ experience. Orthopedics 1995, 18, 561–565. [Google Scholar] [CrossRef]
- Carragee, E.J. Pyogenic vertebral osteomyelitis. J. Bone Joint Surg. Am. 1997, 79, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Colmenero, J.D.; Jimenez-Mejias, M.E.; Sanchez-Lora, F.J.; Reguera, J.M.; Palomino-Nicas, J.; Martos, F.; Garcia de las Heras, J.; Pachon, J. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: A descriptive and comparative study of 219 cases. Ann. Rheum. Dis. 1997, 56, 709–715. [Google Scholar] [CrossRef]
- Hadjipavlou, A.G.; Mader, J.T.; Necessary, J.T.; Muffoletto, A.J. Hematogenous pyogenic spinal infections and their surgical management. Spine 2000, 25, 1668–1679. [Google Scholar] [CrossRef]
- Ledermann, H.P.; Schweitzer, M.E.; Morrison, W.B.; Carrino, J.A. MR imaging findings in spinal infections: Rules or myths? Radiology 2003, 228, 506–514. [Google Scholar] [CrossRef]
- Nather, A.; David, V.; Hee, H.T.; Thambiah, J. Pyogenic vertebral osteomyelitis: A review of 14 cases. J. Orthop. Surg. 2005, 13, 240–244. [Google Scholar] [CrossRef]
- Osenbach, R.K.; Hitchon, P.W.; Menezes, A.H. Diagnosis and management of pyogenic vertebral osteomyelitis in adults. Surg. Neurol. 1990, 33, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Patzakis, M.J.; Rao, S.; Wilkins, J.; Moore, T.M.; Harvey, P.J. Analysis of 61 cases of vertebral osteomyelitis. Clin. Orthop. Relat. Res. 1991, 264, 178–183. [Google Scholar] [CrossRef]
- Stangenberg, M.; Mende, K.C.; Mohme, M.; Kratzig, T.; Viezens, L.; Both, A.; Rohde, H.; Dreimann, M. Influence of microbiological diagnosis on the clinical course of spondylodiscitis. Infection 2021, 49, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Torda, A.J.; Gottlieb, T.; Bradbury, R. Pyogenic vertebral osteomyelitis: Analysis of 20 cases and review. Clin. Infect. Dis. 1995, 20, 320–328. [Google Scholar] [CrossRef]
- Zarrouk, V.; Feydy, A.; Salles, F.; Dufour, V.; Guigui, P.; Redondo, A.; Fantin, B. Imaging does not predict the clinical outcome of bacterial vertebral osteomyelitis. Rheumatology 2007, 46, 292–295. [Google Scholar] [CrossRef]
- Vettivel, J.; Bortz, C.; Passias, P.G.; Baker, J.F. Pyogenic Vertebral Column Osteomyelitis in Adults: Analysis of Risk Factors for 30-Day and 1-Year Mortality in a Single Center Cohort Study. Asian Spine J. 2019, 13, 608–614. [Google Scholar] [CrossRef]
- Heuer, A.; Strahl, A.; Viezens, L.; Koepke, L.G.; Stangenberg, M.; Dreimann, M. The Hamburg Spondylodiscitis Assessment Score (HSAS) for Immediate Evaluation of Mortality Risk on Hospital Admission. J. Clin. Med. 2022, 11, 660. [Google Scholar] [CrossRef]
- Hasan, G.A.; Raheem, H.Q.; Qutub, A.; Wais, Y.B.; Katran, M.H.; Shetty, G.M. Management of Pyogenic Spondylodiscitis Following Nonspinal Surgeries: A Tertiary Care Center Experience. Int. J. Spine Surg. 2021, 15, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Pigrau, C.; Almirante, B.; Flores, X.; Falco, V.; Rodriguez, D.; Gasser, I.; Villanueva, C.; Pahissa, A. Spontaneous pyogenic vertebral osteomyelitis and endocarditis: Incidence, risk factors, and outcome. Am. J. Med. 2005, 118, 1287. [Google Scholar] [CrossRef]
- Braun, A.; Germann, T.; Wunnemann, F.; Weber, M.A.; Schiltenwolf, M.; Akbar, M.; Burkholder, I.; Kauczor, H.U.; Rehnitz, C. Impact of MRI, CT, and Clinical Characteristics on Microbial Pathogen Detection Using CT-Guided Biopsy for Suspected Spondylodiscitis. J. Clin. Med. 2019, 9, 32. [Google Scholar] [CrossRef]
- Michel, S.C.; Pfirrmann, C.W.; Boos, N.; Hodler, J. CT-guided core biopsy of subchondral bone and intervertebral space in suspected spondylodiskitis. AJR Am. J. Roentgenol. 2006, 186, 977–980. [Google Scholar] [CrossRef] [PubMed]
- Rieneck, K.; Hansen, S.E.; Karle, A.; Gutschik, E. Microbiologically verified diagnosis of infectious spondylitis using CT-guided fine needle biopsy. APMIS 1996, 104, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Spieth, P.M.; Kubasch, A.S.; Penzlin, A.I.; Illigens, B.M.; Barlinn, K.; Siepmann, T. Randomized controlled trials—A matter of design. Neuropsychiatr. Dis Treat. 2016, 12, 1341–1349. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | N = 208 | Percentage |
|---|---|---|
| Male | 136 | 65.4% |
| Female | 72 | 34.6% |
| Age | 68 [23–90] y * | - |
| Spondylodiscitis | 142 | 68.3% |
| Isolated spinal epidural empyema | 66 | 31.7% |
| Surgery | 208 | 100% |
| Blood cultures | 208 | 100% |
| Psoas abscess | 128 | 61.5% |
| CT-guided biopsy of Psoas | 70/128 | 54.7% |
| Known causative pathogens | 192 | 92.3% |
| Unknown causative pathogens | 16 | 7.7% |
| Pyogenic spinal infection | 187/192 | 97.4% |
| Non-pyogenic spinal infection | 5/192 | 2.6% |
| Gram-positive pathogens | 162/187 | 86.6% |
| Gram-negative pathogens | 25/187 | 13.4% |
| Empiric antibiotic therapy | 140 | 67.3% |
| Targeted antibiotic therapy | 68 | 32.7% |
| Duration of intravenous antibiotics | 4 [3–6] w * | - |
| Duration of antibiotics | 8 [6–12] w * | - |
| Death | 12 | 5.8% |
| Infection Subgroup | All Three Procedures | Blood Cultures | Intraoperative Specimens | CT-Guided Biopsies |
|---|---|---|---|---|
| SD with TAT | 53/53 (100%) | 35/53 (66.0%) | 43/53 (81.1%) | 11/22 (50%) |
| SD with ongoing EAT | 77/89 (86.5%) | 56/89 (62.9%) | 60/89 (67.4%) | 17/28 (66.7%) |
| p-value * | 0.004 | 0.722 | 0.084 | 0.568 |
| ISEE with TAT | 15/15 (100%) | 7/15 (46.7%) | 13/15 (86.7%) | 4/5 (80%) |
| ISEE with ongoing EAT | 47/51 (92.2%) | 21/51 (41.2%) | 46/51 (90.2%) | 7/15 (46.7%) |
| p-value * | 0.567 | 0.771 | 0.653 | 0.319 |
| Procedure of Pathogen Detection | TAT | EAT | ||||
|---|---|---|---|---|---|---|
| SD | ISEE | p-Value * | SD | ISEE | p-Value * | |
| Exclusively blood culture | 8/53 (15.1) | 2/15 (13.3) | 1.0 | 14/89 (18.2%) | 1/51 (2.1%) | 0.010 |
| Exclusively intraoperative specimens | 15/53 (28.3) | 7/15 (46.7%) | 0.218 | 19/89 (24.7%) | 24/51 (51.1%) | 0.002 |
| Exclusively CT-guided Biopsy | 0/53 (0.0%) | 0/15 (0.0%) | --- | 2/89 (2.6%) | 0/51 (0.0%) | 0.534 |
| More than one procedure | 30/53 (56.6%) | 6/15 (40.0%) | 0.380 | 42/89 (54.5%) | 22/51 (46.8%) | 0.725 |
| Unknown pathogens | 0 | 0 | 12 | 4 | ||
| Procedure of First Pathogen Detection | TAT | EAT | ||||
|---|---|---|---|---|---|---|
| SD | ISEE | p-Value * | SD | ISEE | p-Value * | |
| Blood culture | 31/53 (58.5%) | 6/15 (40%) | 0.340 | 50/89 (64.9%) | 18/51 (38.3%) | 0.008 |
| Intraoperative specimens | 21/53 (39.6%) | 8/1 (53.3%) | 24/89 (31.2%) | 28/51 (59.6%) | ||
| CT-guided Biopsy | 1/53 (1.9%) | 1/15 (6.7%) | 3/89 (3.9%) | 1/51 (2.1%) | ||
| Unknown pathogens | 0 | 0 | 12 | 4 | ||
| Author | Blood Culture | Image-Guided Biopsy | Intraoperative Specimen |
|---|---|---|---|
| Vettivel et al. [37] | 37 (48.7%) | 30/40 (75%) * | |
| Heuer et al. [38] | 145/307 (47%) | 213/307 (64%) * | |
| Widdrington et al. [25] | 40/78 (51%) | 21/29 (72%) | 25/38 (66%) |
| Hasan et al. [39] | 17/40 (42.5%) | 33/40 (82.5%) | NR |
| Stangenberg et al. [34] | 97/182 (53.3%) | NR | 134/202 (66.3%) |
| Nolla et al. [12] | 46/64 (63.4%) | 11/21 (52%) | 15/20 (75%) |
| Colmenero et al. [28] | 52/152 (34.2%) | NR | NR |
| Pigrau et al. [40] | 71/91 (78%) | NR | NR |
| McHenry et al. [17] | 156/255 (61.2%) | 86/124 (69.4%) | 88/113 (77.9%) |
| Patzakis et al. [33] | 13/26 (50%) | NR | NR |
| Zarrouk et al. [36] | 14/29 (48.3%) | 11/15 (73.4%) | NR |
| Carragee et al. [27] | 66/111 (59.5%) | NR | NR |
| Ledermann et al. [30] | 25/41 (61%) | NR | NR |
| Bateman et al. [26] | 23/52 (44.2%) | NR | 24/32 (75%) |
| Torda et al. [35] | 10/16 (62.5%) | NR | NR |
| Osenbach et al. [32] | 12/40 (30%) | NR | NR |
| Hadjipavlou et al. [29] | NR | 19/26 (73.1%) | 25/40 (62.5%) |
| Nather et al. [31] | 5/9 (55.6%) | NR | 14/16 (87.5%) |
| Current study | 119/208 (57%) | 39/70 (56%) | 162/208 (78%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hijazi, M.M.; Siepmann, T.; Disch, A.C.; Platz, U.; Juratli, T.A.; Eyüpoglu, I.Y.; Podlesek, D. Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment. J. Clin. Med. 2023, 12, 3693. https://doi.org/10.3390/jcm12113693
Hijazi MM, Siepmann T, Disch AC, Platz U, Juratli TA, Eyüpoglu IY, Podlesek D. Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment. Journal of Clinical Medicine. 2023; 12(11):3693. https://doi.org/10.3390/jcm12113693
Chicago/Turabian StyleHijazi, Mido Max, Timo Siepmann, Alexander Carl Disch, Uwe Platz, Tareq A. Juratli, Ilker Y. Eyüpoglu, and Dino Podlesek. 2023. "Diagnostic Sensitivity of Blood Culture, Intraoperative Specimen, and Computed Tomography-Guided Biopsy in Patients with Spondylodiscitis and Isolated Spinal Epidural Empyema Requiring Surgical Treatment" Journal of Clinical Medicine 12, no. 11: 3693. https://doi.org/10.3390/jcm12113693