
Impaired Global Precedence Effect in Severe Alcohol Use Disorder and Korsakoff’s Syndrome: A Pilot Exploration through a Global/Local Visual Paradigm

Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Apparatus and Procedure
2.3. Statistical Analyses
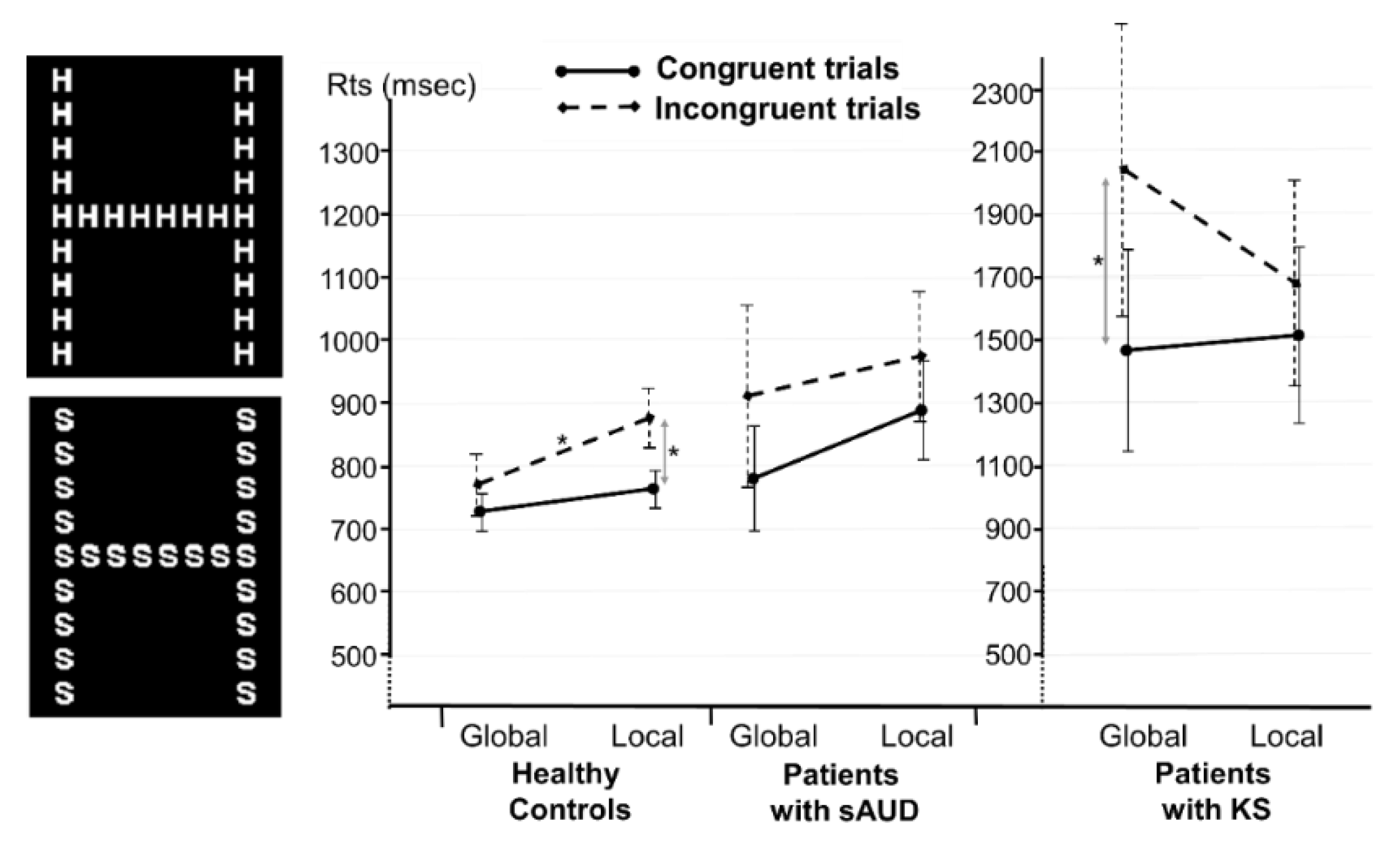
3. Results

4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Subramanya, S.B.; Subramanian, V.S.; Said, H.M. Chronic Alcohol Consumption and Intestinal Thiamin Absorption: Effects on Physiological and Molecular Parameters of the Uptake Process. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 299, G23–G31. [Google Scholar] [CrossRef] [PubMed]
- Fama, R.; Pitel, A.-L.; Sullivan, E.V. Anterograde Episodic Memory in Korsakoff Syndrome. Neuropsychol. Rev. 2012, 22, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Pitel, A.-L.; Eustache, F.; Beaunieux, H. Component Processes of Memory in Alcoholism. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 125, pp. 211–225. ISBN 978-0-444-62619-6. [Google Scholar]
- Maharasingam, M.; Macniven, J.A.B.; Mason, O.J. Executive Functioning in Chronic Alcoholism and Korsakoff Syndrome. J. Clin. Exp. Neuropsychol. 2013, 35, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Moerman-van den Brink, W.G.; van Aken, L.; Verschuur, E.M.L.; Walvoort, S.J.W.; Egger, J.I.M.; Kessels, R.P.C. Executive Dysfunction in Patients with Korsakoff’s Syndrome: A Theory-Driven Approach. Alcohol Alcohol. 2019, 54, 23–29. [Google Scholar] [CrossRef]
- Creupelandt, C.; Maurage, P.; DˈHondt, F. Visuoperceptive Impairments in Severe Alcohol Use Disorder: A Critical Review of Behavioral Studies. Neuropsychol. Rev. 2021, 31, 361–384. [Google Scholar] [CrossRef]
- Oscar-Berman, M.; Kirkley, S.M.; Gansler, D.A.; Couture, A. Comparisons of Korsakoff and Non-Korsakoff Alcoholics on Neuropsychological Tests of Prefrontal Brain Functioning. Alcohol Clin. Exp. Res. 2004, 28, 667–675. [Google Scholar] [CrossRef]
- Gollin, E.S. Developmental Studies of Visual Recognition of Incomplete Objects. Percept. Mot. Ski. 1960, 11, 289–298. [Google Scholar] [CrossRef]
- Kasse, E.; Oudman, E.; Olivier, M.; Wijnia, J.W.; Postma, A. Subtle Object Location Perception Deficits in Korsakoff’s Syndrome. J. Clin. Exp. Neuropsychol. 2019, 41, 881–887. [Google Scholar] [CrossRef]
- Navon, D. Forest before Trees: The Precedence of Global Features in Visual Perception. Cogn. Psychol. 1977, 9, 353–383. [Google Scholar] [CrossRef]
- Kimchi, R. Primacy of Wholistic Processing and Global/Local Paradigm: A Critical Review. Psychol. Bull. 1992, 112, 24–38. [Google Scholar] [CrossRef]
- Poirel, N.; Pineau, A.; Mellet, E. What Does the Nature of the Stimuli Tell Us about the Global Precedence Effect? Acta Psychol. 2008, 127, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wegner, A.J.; Günthner, A.; Fahle, M. Visual Performance and Recovery in Recently Detoxified Alcoholics. Alcohol Alcohol. 2001, 36, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Müller-Oehring, E.M.; Schulte, T.; Fama, R.; Pfefferbaum, A.; Sullivan, E.V. Global-Local Interference Is Related to Callosal Compromise in Alcoholism: A Behavior-DTI Association Study. Alcohol Clin. Exp. Res. 2009, 33, 477–489. [Google Scholar] [CrossRef]
- Müller-Oehring, E.M.; Schulte, T.; Raassi, C.; Pfefferbaum, A.; Sullivan, E.V. Local-Global Interference Is Modulated by Age, Sex and Anterior Corpus Callosum Size. Brain Res. 2007, 1142, 189–205. [Google Scholar] [CrossRef] [PubMed]
- Kramer, J.H.; Blusewicz, M.J.; Robertson, L.C.; Preston, K. Effects of Chronic Alcoholism on Perception of Hierarchical Visual Stimuli. Alcohol Clin. Exp. Res. 1989, 13, 240–245. [Google Scholar] [CrossRef]
- Kéïta, L.; Bedoin, N.; Burack, J.; Lepore, F. Switching between Global and Local Levels: The Level Repetition Effect and Its Hemispheric Asymmetry. Front. Psychol. 2014, 5, 252. [Google Scholar]
- Poirel, N.; Krakowski, C.S.; Sayah, S.; Pineau, A.; Houdé, O.; Borst, G. Do You Want to See the Tree? Ignore the Forest: Inhibitory Control during Local Processing: A Negative Priming Study of Local-Global Processing. Exp. Psychol. 2014, 61, 205–214. [Google Scholar] [CrossRef]
- American Psychiatric Assossciation. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th ed.; American Psychiatric Publishing, Inc.:: Arlington, VA, USA, 2013; p. 947. ISBN 978-0-89042-554-1. [Google Scholar]
- Delis, D.; Kramer, J.; Kaplan, E.; Ober, B. California Verbal Learning Test (CVLT) Manual; Psychological Corp.: San Antonio, TX, USA, 1987. [Google Scholar]
- Gache, P.; Michaud, P.; Landry, U.; Accietto, C.; Arfaoui, S.; Wenger, O.; Daeppen, J.-B. The Alcohol Use Disorders Identification Test (AUDIT) as a Screening Tool for Excessive Drinking in Primary Care: Reliability and Validity of a French Version. Alcohol. Clin. Exp. Res. 2005, 29, 2001–2007. [Google Scholar] [CrossRef]
- Cushman, P.; Forbes, R.; Lemer, W.; Stewart, M. Alcohol Withdrawal Syndromes: Clinical Management with Lofexidine. Alcohol. Clin. Exp. Res. 1985, 9, 103–108. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Bar, M. The Proactive Brain: Memory for Predictions. Philos. Trans. R. Soc. B 2009, 364, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Creupelandt, C.; D’Hondt, F.; Maurage, M. Towards a Dynamic Exploration of Vision, Cognition and Emotion in Alcohol-Use Disorders. Curr. Neuropharmacol. 2019, 17, 492–506. [Google Scholar] [CrossRef] [PubMed]
- Bruyer, R.; Scailquin, J.C.; Samson, D. Aging and the Locus of the Global Precedence Effect: A Short Review and New Empirical Data. Exp. Aging Res. 2003, 29, 237–268. [Google Scholar] [CrossRef] [PubMed]
- Winskel, H.; Kim, T.H.; Cho, J.R. The global precedence effect in English and Korean native speakers with Roman, Korean Hangul and Thai compound letters. Acta Psychol. 2018, 187, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Bouvet, L.; Rousset, S.; Valdois, S.; Donnadieu, S. Global Precedence Effect in Audition and Vision: Evidence for Similar Cognitive Styles across Modalities. Acta Psychol. 2011, 138, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Rando, K.; Hong, K.I.; Bhagwagar, Z.; Li, C.S.R.; Bergquist, K.; Guarnaccia, J.; Sinha, R. Association of Frontal and Posterior Cortical Gray Matter Volume with Time to Alcohol Relapse: A Prospective Study. Am. J. Psychiatry 2011, 168, 183–192. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.J.; Wong, T.Y. Alcohol and Eye Diseases. Surv. Ophthalmol. 2008, 53, 512–525. [Google Scholar] [CrossRef]
- Marco, E.J.; Hinkley, L.B.; Hill, S.S.; Nagarajan, S.S. Sensory Processing in Autism: A Review of Neurophysiologic Findings. Pediatr. Res. 2011, 69, 48–54. [Google Scholar] [CrossRef]
- Mottron, L.; Dawson, M.; Soulieres, I.; Hubert, B.; Burack, J.A. Enhanced Perceptual Functioning in Autism: An Update, and Eight Principles of Autistic Perception. J. Autism Dev. Disord. 2006, 36, 27–43. [Google Scholar] [CrossRef]
- Poirel, N.; Brazo, P.; Turbelin, M.-R.; Lecardeur, L.; Simon, G.; Houdé, O.; Pineau, A.; Dollfus, S. Meaningfulness and Global-Local Processing in Schizophrenia. Neuropsychologia 2010, 48, 3062–3068. [Google Scholar] [CrossRef]
- Brion, M.; Pitel, A.L.; Beaunieux, H.; Maurage, P. Revisiting the Continuum Hypothesis: Toward an In-Depth Exploration of Executive Functions in Korsakoff Syndrome. Front. Hum. Neurosci. 2014, 8, 498. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.R.; Halligan, P.W.; Marshall, J.C.; Frith, C.D.; Frackowiak, R.S.; Dolan, R.J. Where in the Brain does Visual Attention Select the Forest and the Trees? Nature 1996, 382, 626–628. [Google Scholar] [CrossRef] [PubMed]
- Poirel, N.; Simon, G.; Cassotti, M.; Leroux, G.; Perchey, G.; Lanoë, C.; Lubin, A.; Turbelin, M.R.; Rossi, S.; Pineau, A.; et al. The Shift from Local to Global Visual Processing in 6-year-old Children is Associated with Grey Matter Loss. PLoS ONE 2011, 6, e20879. [Google Scholar] [CrossRef] [PubMed]
- Pitel, A.-L.; Chételat, G.; Le Berre, A.P.; Desgranges, B.; Eustache, F.; Beaunieux, H. Macrostructural Abnormalities in Korsakoff Syndrome Compared with Uncomplicated Alcoholism. Neurology 2012, 78, 1330–1333. [Google Scholar] [CrossRef]
- Maillard, A.; Laniepce, A.; Cabé, N.; Boudehent, C.; Chételat, G.; Urso, L.; Eustache, F.; Vabret, F.; Segobin, S.; Pitel, A.L. Temporal Cognitive and Brain Changes in Korsakoff Syndrome. Neurology 2021, 96, e1987–e1998. [Google Scholar] [CrossRef] [PubMed]
- Schulte, T.; Müller-Oehring, E.M. Contribution of Callosal Connections to the Interhemispheric Integration of Visuomotor and Cognitive Processes. Neuropsychol. Rev. 2010, 20, 174–190. [Google Scholar] [CrossRef]
- Kimchi, R.; Amishav, R.; Sulitzeanu-Kenan, A. Gender Differences in Global-Local Perception? Evidence from Orientation and Shape Judgments. Acta Psychol. 2009, 130, 64–71. [Google Scholar] [CrossRef]
- Bouhassoun, S.; Poirel, N.; Hamlin, N.; Doucet, G.E. The Forest, the Trees, and the Leaves across Adulthood: Age-Related Changes on a Visual Search Task Containing Three-Level Hierarchical Stimuli. Atten. Percept. Psychophys. 2022, 84, 1004–1015. [Google Scholar] [CrossRef]
- Gerlach, C.; Poirel, N. Navon’s Classical Paradigm Concerning Local and Global Processing Relates Systematically to Visual Object Classification Performance. Sci. Rep. 2018, 8, 324. [Google Scholar] [CrossRef]

{kind=link}
| Healthy Controls N = 41 | Patients with sAUD N = 16 | Patients with KS N = 7 | |
|---|---|---|---|
| Age * | 46.00 ± 11.91 | 47.40 ± 11.35 | 56.60 ± 4.65 |
| Gender * | 27 M/14 W | 16 M/0 W | 0 M/7 W |
| Education (in years) | 11.40 ± 1.76 | 11.80 ± 2.51 | 10.70 ± 1.38 |
| AUDIT score | <7 for men | 26.38 ± 7.22 | Not available |
| <6 for women | |||
| Daily alcohol consumption | <1 | 15.09 ± 6.74 | Not available |
| Abstinence duration | - | 7.38 ± 2.60 | About 10 years 1 |
| CVLT | |||
| Trail 5 | - | - | 6.71 ± 2.89 |
| Short-term free recall | - | - | 1.43 ± 1.27 |
| Long-term free recall | - | - | 1.57 ± 1.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitel, A.L.; Laniepce, A.; Boudehent, C.; Poirel, N. Impaired Global Precedence Effect in Severe Alcohol Use Disorder and Korsakoff’s Syndrome: A Pilot Exploration through a Global/Local Visual Paradigm. J. Clin. Med. 2023, 12, 3655. https://doi.org/10.3390/jcm12113655
Pitel AL, Laniepce A, Boudehent C, Poirel N. Impaired Global Precedence Effect in Severe Alcohol Use Disorder and Korsakoff’s Syndrome: A Pilot Exploration through a Global/Local Visual Paradigm. Journal of Clinical Medicine. 2023; 12(11):3655. https://doi.org/10.3390/jcm12113655
Chicago/Turabian StylePitel, Anne Lise, Alice Laniepce, Céline Boudehent, and Nicolas Poirel. 2023. "Impaired Global Precedence Effect in Severe Alcohol Use Disorder and Korsakoff’s Syndrome: A Pilot Exploration through a Global/Local Visual Paradigm" Journal of Clinical Medicine 12, no. 11: 3655. https://doi.org/10.3390/jcm12113655