
Treatment of Trochanteric Hip Fractures with Cephalomedullary Nails: Single Head Screw vs. Dual Integrated Compression Screw Systems
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Subjects
2.3. Study Variables
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Risk of Reoperation in the Follow-Up Adjusting by Cox Regression Modeling
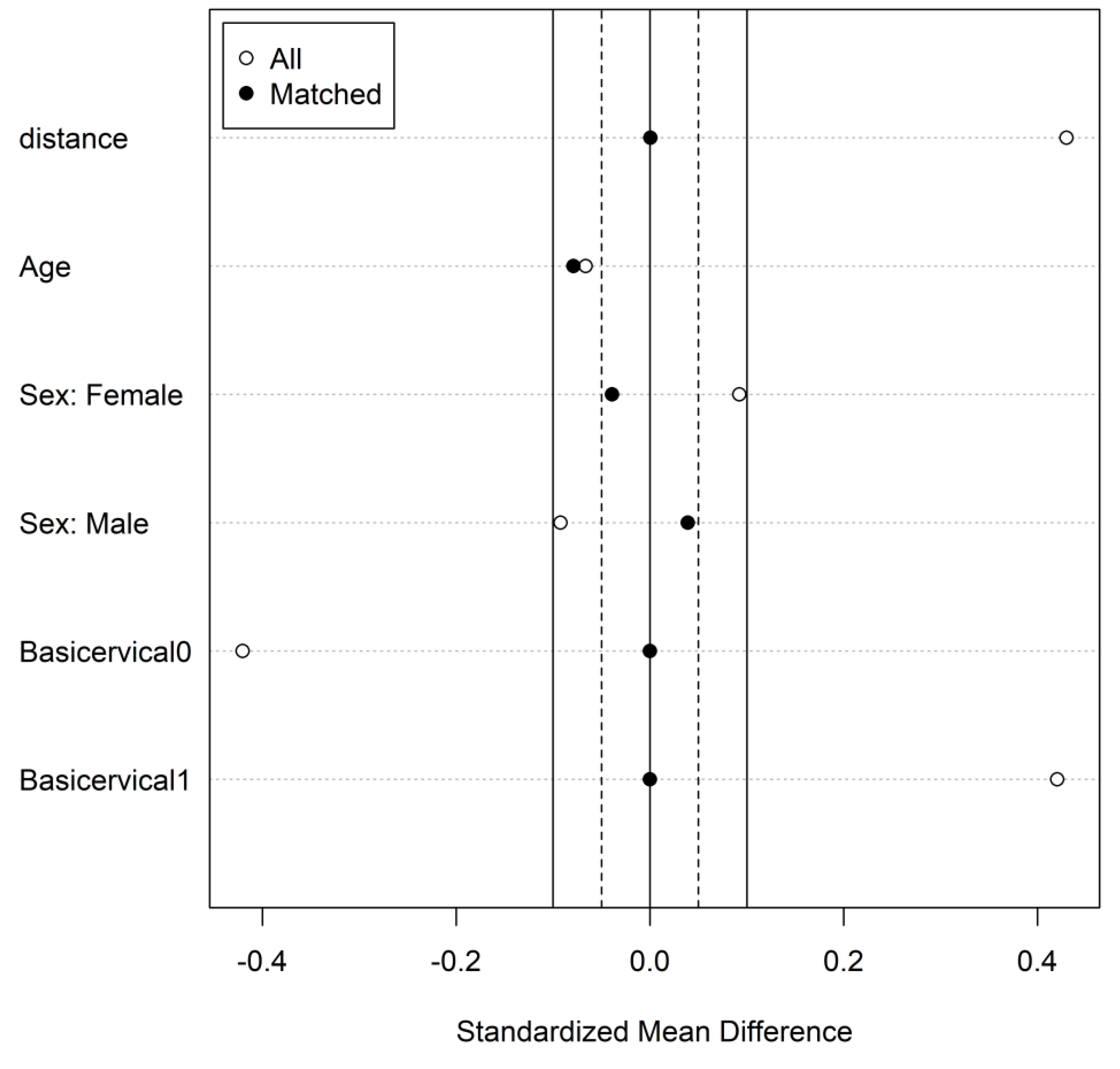
3.2. Risk of Reoperation Evaluated after Propensity Score Matching
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huette, P.; Abou-Arab, O.; Djebara, A.-E.; Terrasi, B.; Beyls, C.; Guinot, P.-G.; Havet, E.; Dupont, H.; Lorne, E.; Ntouba, A.; et al. Risk Factors and Mortality of Patients Undergoing Hip Fracture Surgery: A One-Year Follow-up Study. Sci. Rep. 2020, 10, 9607. [Google Scholar] [CrossRef] [PubMed]
- Aubrun, F. Fracture de l’extrémité Supérieure Du Fémur Du Patient Âgé: Aspect Épidémiologique, Facteurs de Risque. Ann. Fr. Ann. Anesth. Resusc. 2011, 30, e37–e39. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Handoll, H.H. Gamma and Other Cephalocondylic Intramedullary Nails versus Extramedullary Implants for Extracapsular Hip Fractures in Adults. Cochrane Database Syst. Rev. 2008, 16, CD000093. [Google Scholar] [CrossRef]
- Date, A.; Panthula, M.; Bolina, A. Comparison of Clinical and Radiological Outcomes in Intertrochanteric Fractures Treated with InterTAN Nail against Conventional Cephalomedullary Nails: A Systematic Review. Future Sci. OA 2021, 7, FSO668. [Google Scholar] [CrossRef] [PubMed]
- Santoni, B.G.; Diaz, M.A.; Stoops, T.K.; Lannon, S.; Ali, A.; Sanders, R.W. Biomechanical Investigation of an Integrated 2-Screw Cephalomedullary Nail Versus a Sliding Hip Screw in Unstable Intertrochanteric Fractures. J. Orthop. Trauma 2019, 33, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.-L.; Wang, X.; Luan, F.-J.; Xu, H.-T.; Fang, Y.; Min, J.; Luan, H.-X.; Yang, F.; Zheng, H.; He, S.-J. Proximal Femoral Nails Antirotation, Gamma Nails, and Dynamic Hip Screws for Fixation of Intertrochanteric Fractures of Femur: A Meta-Analysis. Orthop. Traumatol. Surg. Res. 2014, 100, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Queally, J.M.; Harris, E.; Handoll, H.H.; Parker, M.J. Intramedullary Nails for Extracapsular Hip Fractures in Adults. Cochrane Database Syst. Rev. 2014, 9, CD004961. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Sun, K.; Wang, X. A Randomized Prospective Comparison of InterTAN and Gamma3 for Treating Unstable Intertrochanteric Fractures. Int. J. Clin. Exp. Med. 2016, 9, 8640–8647. [Google Scholar]
- Berger-Groch, J.; Rupprecht, M.; Schoepper, S.; Schroeder, M.; Rueger, J.M.; Hoffmann, M. Five-Year Outcome Analysis of Intertrochanteric Femur Fractures: A Prospective Randomized Trial Comparing a 2-Screw and a Single-Screw Cephalomedullary Nail. J. Orthop. Trauma 2016, 30, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhang, K.; Jia, Y.; Yu, B.; Feng, W. InterTan Nail Versus Proximal Femoral Nail Antirotation-Asia in the Treatment of Unstable Trochanteric Fractures. Orthopedics 2013, 36, 182. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Xu, B.; Liang, G.; Zeng, X.; Zeng, D.; Chen, D.; Ge, Z.; Yu, W.; Zhang, X. Optimizing Stability in AO/OTA 31-A2 Intertrochanteric Fracture Fixation in Older Patients with Osteoporosis. J. Int. Med. Res. 2018, 46, 1767–1778. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhu, X.; Pei, G.; Zeng, X.; Zhang, N.; Xu, P.; Chen, D.; Yu, W.; Zhang, X. A Retrospective Analysis of the InterTan Nail and Proximal Femoral Nail Anti-Rotation in the Treatment of Intertrochanteric Fractures in Elderly Patients with Osteoporosis: A Minimum Follow-up of 3 Years. J. Orthop. Surg. Res. 2017, 12, 147. [Google Scholar] [CrossRef] [PubMed]
- Ülkü, T.K.; Tok, O.; Seyhan, M.; Gereli, A.; Kaya, A. Comparison of Third Generation Proximal Femoral Nails in Treatment of Reverse Oblique Intertrochanteric Fractures. Bezmialem Sci. 2019, 7, 271–275. [Google Scholar] [CrossRef]
- Ricci, M.J.; McAndrew, C.M.; Miller, A.N.; Kamath, G.; Ricci, W.M. Are Two-Part Intertrochanteric Femur Fractures Stable and Does Stability Depend on Fixation Method? J. Orthop. Trauma 2019, 33, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, J.; Ji, G. Comparison of Clinical Outcomes with Proximal Femoral Nail Anti-Rotation versus InterTAN Nail for Intertrochanteric Femoral Fractures: A Meta-Analysis. J. Orthop. Surg. Res. 2020, 15, 500. [Google Scholar] [CrossRef] [PubMed]
- Nherera, L.; Trueman, P.; Horner, A.; Watson, T.; Johnstone, A.J. Comparison of a Twin Interlocking Derotation and Compression Screw Cephalomedullary Nail (InterTAN) with a Single Screw Derotation Cephalomedullary Nail (Proximal Femoral Nail Antirotation): A Systematic Review and Meta-Analysis for Intertrochanteric Fractures. J. Orthop. Surg. Res. 2018, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Quartley, M.; Chloros, G.; Papakostidis, K.; Saunders, C.; Giannoudis, P.V. Stabilisation of AO OTA 31-A Unstable Proximal Femoral Fractures: Does the Choice of Intramedullary Nail Affect the Incidence of Post-Operative Complications? A Systematic Literature Review and Meta-Analysis. Injury 2022, 53, 827–840. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Pelpola, K.; Ball, M.; Ong, A.; Myint, P.K. Pre-Operative Indicators for Mortality Following Hip Fracture Surgery: A Systematic Review and Meta-Analysis. Age Ageing 2014, 43, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Chehade, M.J.; Carbone, T.; Awwad, D.; Taylor, A.; Wildenauer, C.; Ramasamy, B.; McGee, M. Influence of Fracture Stability on Early Patient Mortality and Reoperation After Pertrochanteric and Intertrochanteric Hip Fractures. J. Orthop. Trauma. 2015, 29, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Panteli, M.; Vun, J.S.H.; West, R.M.; Howard, A.; Pountos, I.; Giannoudis, P.V. Subtrochanteric Femoral Fractures and Intramedullary Nailing Complications: A Comparison of Two Implants. J. Orthop. Traumatol. 2022, 23, 27. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 387) | Gamma3 (n = 262) | InterTAN (n = 125) | p-Value | |
|---|---|---|---|---|
| Age, mean (SD) | 81.6 (11.3) | 81.9 (10.7) | 81.1 (12.5) | 0.524 |
| Gender, Female, n (%) | 287 (74.2%) | 191 (72.9%) | 96 (76.8%) | 0.487 |
| Laterality, right side, n (%) | 213 (55.0%) | 140 (53.4%) | 73 (58.4%) | 0.419 |
| Type of fracture, n (%) | <0.001 | |||
| Intertrochanteric | 240 (62%) | 170 (64.9%) | 70 (56%) | 0.116 |
| Persubtrochanteric | 52 (13.4%) | 36 (13.7%) | 16 (12.8%) | 0.925 |
| Basicervical | 51 (13.2%) | 19 (7.3%) | 32 (25.6%) | <0.001 |
| Subtrochanteric | 44 (11.4%) | 37 (14.1%) | 7 (5.6%) | 0.022 |
| Total (n = 387) | Gamma3 (n = 262) | InterTAN (n = 125) | p-Value | |
|---|---|---|---|---|
| Median of follow up (P25–P75) | 1.1 (0.5–1.8) | 1.0 (0.5–1.8) | 1.2 (0.6–1.7) | 0.82 |
| Reoperations in the follow-up period after surgery, n (%) | 17 & (4.4%) | 6 (2.3%) | 11 & (8.8%) | 0.008 |
| Reoperation required, rates at 1.5 Years Following Surgery *, % | 5.8% | 1.9% | 13.3% | 0.009 |
| Any complication, rates at 1.5 Years Following Surgery, n (%) | 18 (4.7%) | 6 (2.3%) | 12 (9.6%) | 0.003 |
| Cut-out | 8 (2.1%) | 2 (0.8%) | 6 (4.8%) | 0.016 |
| Peri-implant fracture | 6 (1.6%) | 2 (0.8%) | 4 (3.2%) | 0.089 |
| Nail Tear | 3 (0.8%) | 1 (0.4%) | 2 (1.6%) | 0.245 |
| Infection | 1 (0.3%) | 1 (0.4%) | 0 | >0.99 |
| Second reoperation in the follow-up period after surgery, n (%) | 2 (0.5%) | 1 (0.4%) | 1 (0.8%) | 0.54 |
| Exitus Rates at 1.5 Year Following Surgery *, % | 26.9% | 26.4% | 27.8% | 0.79 |
| Model 1: Not Including Type of Nail | Model 2: Including Type of Nail | |||
|---|---|---|---|---|
| HR [95% CI] | p-Value | HR [95% CI] | p-Value | |
| InterTAN vs. Gamma3 nail | - | - | 3.6 [1.3–10.5] | 0.017 |
| Basicervical fracture | 2.3 [0.82–6.7] | 0.11 | 1.4 [0.47–4.3] | 0.54 |
| Age | 0.99 [0.95–1.03] | 0.70 | 1.0 [0.96–1.04] | 0.94 |
| Men | 1.3 [0.41–4.1] | 0.66 | 1.4 [0.43–4.4] | 0.58 |
| McFadden pseudo-R2 | 0.017 | 0.052 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Méndez-Ojeda, M.M.; Herrera-Rodríguez, A.; Álvarez-Benito, N.; González-Pacheco, H.; García-Bello, M.A.; Álvarez-de la Cruz, J.; Pais-Brito, J.L. Treatment of Trochanteric Hip Fractures with Cephalomedullary Nails: Single Head Screw vs. Dual Integrated Compression Screw Systems. J. Clin. Med. 2023, 12, 3411. https://doi.org/10.3390/jcm12103411
Méndez-Ojeda MM, Herrera-Rodríguez A, Álvarez-Benito N, González-Pacheco H, García-Bello MA, Álvarez-de la Cruz J, Pais-Brito JL. Treatment of Trochanteric Hip Fractures with Cephalomedullary Nails: Single Head Screw vs. Dual Integrated Compression Screw Systems. Journal of Clinical Medicine. 2023; 12(10):3411. https://doi.org/10.3390/jcm12103411
Chicago/Turabian StyleMéndez-Ojeda, Marye M., Alejandro Herrera-Rodríguez, Nuria Álvarez-Benito, Himar González-Pacheco, Miguel A. García-Bello, Javier Álvarez-de la Cruz, and José L. Pais-Brito. 2023. "Treatment of Trochanteric Hip Fractures with Cephalomedullary Nails: Single Head Screw vs. Dual Integrated Compression Screw Systems" Journal of Clinical Medicine 12, no. 10: 3411. https://doi.org/10.3390/jcm12103411