
Disease Perception and Mental Health in Pregnancies with Gestational Diabetes—PsychDiab Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
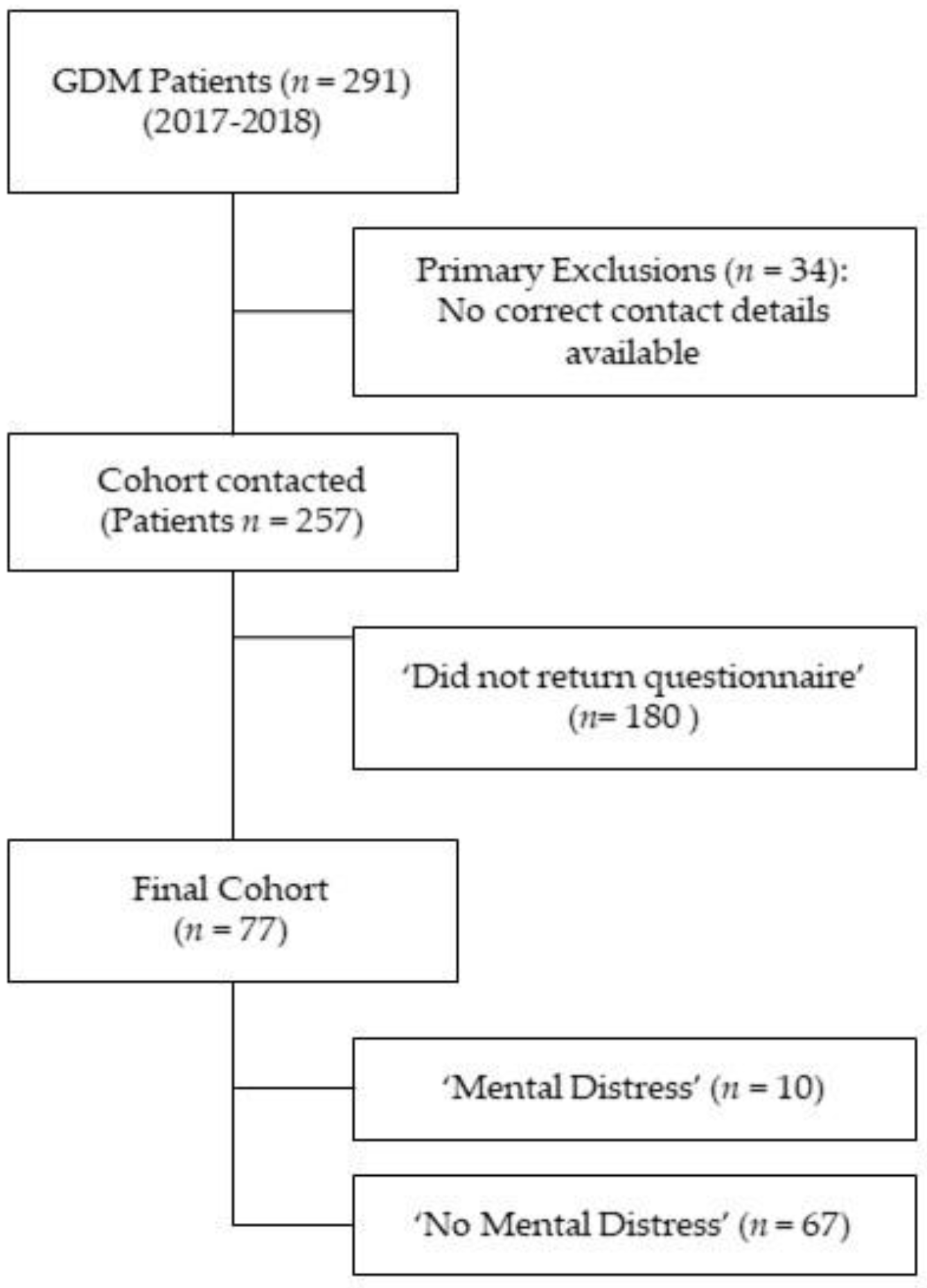
2.1. Study Population
2.2. Study Questionaire
2.3. Study Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Pregnancy and Perinatal Outcome
3.3. Association of Psychological Distress and Overall Well-Being during Pregnancy Obtained by the Psych-Diab-Questionnaire
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Non Responder (n = 180) | PsychDiab Cohort (n = 77) | p |
|---|---|---|---|
| Age in years | 32 (29–36) | 34 (30–36) | 0.056 |
| Gravidity | 2 (1–3) | 1 (1.5–3) | 0.503 |
| Parity | 1 (0–1) | 1 (0–1) | 0.554 |
| Prepregnancy BMI in kg/m2 | 26 (23–30) | 26 (23–30) | 0.938 |
| Prepregnancy BMI categories | 0.915 | ||
| <18.5 kg/m2 (underweight) | 2.1% | 1.3% | |
| 18.5–24.9 kg/m2 (normal) | 40.2% | 44.2% | |
| 25–29.9 kg/m2 (overweight) | 27.8% | 27.3% | |
| ≥30 kg/m2 (obesity) | 20.9% | 27.3% | |
| History of GDM | 16% | 20.8% | 0.374 |
| Thyroid disorders | 20.5% | 26% | 0.518 |
| Cardiovascular disorders | 11.3% | 3.9% | 0.132 |
| Psychiatric disorders | 3.6% | 5.2% | 0.511 |
| Marital status | |||
| single | 4.2% | 3.9% | 0.858 |
| married | 43.5% | 44.2% | |
| permanent relationship | 52.4% | 50.6% | |
| Unemployment | 20.1% | 6.5% | 0.008 * |
| Family History of Diabetes | 65.5% | 63.6% | 0.779 |
| HbA1c at diagnosis in mmol/mol | 31 (29–33) | 32 (29–34) | 0.907 |
| Need for Insulin | 33.7% | 41.6% | 0.262 |
| C-section | 30% | 32.3% | 0.750 |
| GA at delivery | 39 (38–40) | 39 (38–40) | 0.979 |
| Birthweight in g | 3477 (3133–3777) | 3415 (3225–3673) | 0.838 |
References
- IQTIG–Institut für Qualitätssicherung und Transparenz im Gesundheitswesen. Bundesauswertung zum Erfassungsjahr 2020. Geburtshilfe—Qualitätsindikatoren und Kennzahlen. Available online: https://iqtig.org/downloads/auswertung/2020/16n1gebh/QSKH_16n1-GEBH_2020_BUAW_V01_2021-08-10.pdf (accessed on 6 September 2022).
- Evans, M.K.; O’Brien, B. Gestational diabetes: The meaning of an at-risk pregnancy. Qual. Health Res. 2005, 15, 66–81. [Google Scholar] [CrossRef] [PubMed]
- Mautner, E.; Dorfer, M. Diabetes mellitus in pregnancy--a mental strain? Gynakol. Geburtshilfliche Rundsch. 2009, 49, 244–248. [Google Scholar] [CrossRef]
- Draffin, C.; Alderdice, F.A.; McCance, D.R.; Maresh, M.; Harper, R.; McSorley, O.; Holmes, V.A. Exploring the needs, concerns and knowledge of women diagnosed with gestational diabetes: A qualitative study. Midwifery 2016, 40, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, D.; Carrozzino, D.; Fraticelli, F.; Fulcheri, M.; Vitacolonna, E. Quality of Life in Women with Gestational Diabetes Mellitus: A Systematic Review. J. Diabetes Res. 2017, 2017, 7058082. [Google Scholar] [CrossRef] [PubMed]
- Dalfra, M.G.; Nicolucci, A.; Bisson, T.; Bonsembiante, B.; Lapolla, A. Quality of life in pregnancy and post-partum: A study in diabetic patients. Qual. Life Res. 2012, 21, 291–298. [Google Scholar] [CrossRef]
- Danyliv, A.; Gillespie, P.; O’Neill, C.; Noctor, E.; O’Dea, A.; Tierney, M.; McGuire, B.E.; Glynn, L.G.; Dunne, F.P. Health related quality of life two to five years after gestational diabetes mellitus: Cross-sectional comparative study in the ATLANTIC DIP cohort. BMC Pregnancy Childbirth 2015, 15, 274. [Google Scholar] [CrossRef]
- Hinkle, S.N.; Buck Louis, G.M.; Rawal, S.; Zhu, Y.; Albert, P.S.; Zhang, C. A longitudinal study of depression and gestational diabetes in pregnancy and the postpartum period. Diabetologia 2016, 59, 2594–2602. [Google Scholar] [CrossRef]
- WHO. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. Available online: https://apps.who.int/iris/bitstream/handle/10665/85975/WHO_NMH_MND_13.2_eng.pdf?sequence=1 (accessed on 6 September 2022).
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- Deutsche Diabetes Gesellschaft; Deutsche Gesellschaft für Gynäkologie und Geburtshilfe. S3-Leitlinie Gestationsdiabetes Mellitus (GDM), Diagnostik, Therapie und Nachsorge. Available online: https://www.awmf.org/uploads/tx_szleitlinien/057-008l_S3_Gestationsdiabetes-mellitus-GDM-Diagnostik-Therapie-Nachsorge_2019-06.pdf (accessed on 6 September 2022).
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90: An outpatient psychiatric rating scale--preliminary report. Psychopharmacol. Bull. 1973, 9, 13–28. [Google Scholar]
- Medicine, I.O.; Council, N.R. Weight Gain during Pregnancy: Reexamining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- WHO. Body Mass Index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 15 December 2020).
- Voigt, M.; Rochow, N.; Schneider, K.T.; Hagenah, H.P.; Scholz, R.; Hesse, V.; Wittwer-Backofen, U.; Straube, S.; Olbertz, D. New percentile values for the anthropometric dimensions of singleton neonates: Analysis of perinatal survey data of 2007-2011 from all 16 states of Germany. Z. Geburtshilfe Neonatol. 2014, 218, 210–217. [Google Scholar] [CrossRef]
- Hayashi, A.; Oguchi, H.; Kozawa, Y.; Ban, Y.; Shinoda, J.; Suganuma, N. Factors associated with symptoms of depression among pregnant women with gestational diabetes mellitus in Japan. Drug. Discov. Ther. 2020, 14, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Jarvie, R. Lived experiences of women with co-existing BMI>/=30 and Gestational Diabetes Mellitus. Midwifery 2017, 49, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Craig, L.; Sims, R.; Glasziou, P.; Thomas, R. Women’s experiences of a diagnosis of gestational diabetes mellitus: A systematic review. BMC Pregnancy Childbirth 2020, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Muhwava, L.S.; Murphy, K.; Zarowsky, C.; Levitt, N. Perspectives on the psychological and emotional burden of having gestational diabetes amongst low-income women in Cape Town, South Africa. BMC Womens Health 2020, 20, 231. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Ching, S.M.; Hoo, F.K.; Ramachandran, V.; Chong, S.C.; Tusimin, M.; Mohd Nordin, N. Prevalence and factors associated with depressive, anxiety and stress symptoms among women with gestational diabetes mellitus in tertiary care centres in Malaysia: A cross-sectional study. BMC Pregnancy Childbirth 2019, 19, 367. [Google Scholar] [CrossRef] [PubMed]
- Pace, R.; Rahme, E.; Da Costa, D.; Dasgupta, K. Association between gestational diabetes mellitus and depression in parents: A retrospective cohort study. Clin. Epidemiol. 2018, 10, 1827–1838. [Google Scholar] [CrossRef] [PubMed]
- Dame, P.; Cherubini, K.; Goveia, P.; Pena, G.; Galliano, L.; Facanha, C.; Nunes, M.A. Depressive Symptoms in Women with Gestational Diabetes Mellitus: The LINDA-Brazil Study. J. Diabetes Res. 2017, 2017, 7341893. [Google Scholar] [CrossRef]
- Kragelund Nielsen, K.; Vildekilde, T.; Kapur, A.; Damm, P.; Seshiah, V.; Bygbjerg, I.C. “If I Don’t Eat Enough, I Won’t Be Healthy”. Women’s Experiences with Gestational Diabetes Mellitus Treatment in Rural and Urban South India. Int. J. Environ. Res. Public. Health 2020, 17, 62. [Google Scholar] [CrossRef]
- Gilbert, L.; Gross, J.; Lanzi, S.; Quansah, D.Y.; Puder, J.; Horsch, A. How diet, physical activity and psychosocial well-being interact in women with gestational diabetes mellitus: An integrative review. BMC Pregnancy Childbirth 2019, 19, 60. [Google Scholar] [CrossRef]
- Ansarzadeh, S.; Salehi, L.; Mahmoodi, Z.; Mohammadbeigi, A. Factors affecting the quality of life in women with gestational diabetes mellitus: A path analysis model. Health Qual. Life Outcomes 2020, 18, 31. [Google Scholar] [CrossRef]
- Faal Siahkal, S.; Javadifar, N.; Najafian, M.; Iravani, M.; Zakerkish, M.; Heshmati, R. The psychosocial challenges associated with gestational diabetes mellitus: A systematic review of qualitative studies. Prim. Care Diabetes 2022, 16, 11–26. [Google Scholar] [CrossRef]
- Lee, K.W.; Ching, S.M.; Hoo, F.K.; Ramachandran, V.; Chong, S.C.; Tusimin, M.; Ang, F.E.; Mohd Nordin, N.; Devaraj, N.K. Factors associated with poor-to-moderate quality of life among pregnant women with gestational diabetes mellitus: A cross-sectional study in Malaysia. Qual. Life Res. 2020, 29, 2725–2736. [Google Scholar] [CrossRef] [PubMed]
- Figueroa Gray, M.; Hsu, C.; Kiel, L.; Dublin, S. “It’s a Very Big Burden on Me”: Women’s Experiences Using Insulin for Gestational Diabetes. Matern. Child. Health J. 2017, 21, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Pantzartzis, K.A.; Manolopoulos, P.P.; Paschou, S.A.; Kazakos, K.; Kotsa, K.; Goulis, D.G. Gestational diabetes mellitus and quality of life during the third trimester of pregnancy. Qual. Life Res. 2019, 28, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- Martis, R.; Brown, J.; Crowther, C.A. Views and Experiences of New Zealand Women with Gestational Diabetes in Achieving Glycaemic Control Targets: The Views Study. J. Diabetes Res. 2017, 2017, 2190812. [Google Scholar] [CrossRef] [PubMed]
- Hussain, Z.; Yusoff, Z.M.; Sulaiman, S.A. A study exploring the association of attitude and treatment satisfaction with glycaemic level among gestational diabetes mellitus patients. Prim. Care Diabetes 2015, 9, 275–282. [Google Scholar] [CrossRef]


| Variable | Total Cohort (n = 77) | No Mental Distress (n = 67; 87%) | Mental Distress (n = 10; 13%) | p |
|---|---|---|---|---|
| Age in years | 34 (30–36) | 33 (30–36) | 36 (33.5–38.25) | 0.092 |
| Gravidity | 1 (1.5–3) | 2 (2–3) | 2 (1–3) | 0.159 |
| Parity | 1 (0–1) | 1 (0–1) | 1 (0–1.25) | 0.437 |
| Prepregnancy weight in kg | 72.0 (61.5–87.5) | 71 (60–84) | 82 (71–91) | 0.071 |
| Prepregnancy BMI in kg/m2 | 26 (23–30) | 25 (23–30) | 29 (25–34) | 0.049 * |
| Prepregnancy BMI categories | 0.275 | |||
| <18.5 kg/m2 (underweight) | 1.3% | 1.5% | - | |
| 18.5–24.9 kg/m2 (normal) | 44.2% | 47.8% | 20% | |
| 25–29.9 kg/m2 (overweight) | 27.3% | 26.9% | 30% | |
| ≥30 kg/m2 (obesity) | 27.3% | 23.9% | 50% | |
| History of GDM | 20.8% | 22.4% | 10% | 0.678 |
| Thyroid disorders | 26% | 23.9% | 40% | 0.275 |
| Cardiovascular disorders | 3.9% | 4.5% | - | 1 |
| Psychiatric disorders | 5.2% | 6% | - | 1 |
| Marital status | 0.254 | |||
| single | 3.9% | 4.5% | - | |
| married | 44.2% | 47.8% | 2 (20%) | |
| permanent relationship | 50.6% | 46.3% | 8 (80%) | |
| unknown | 1.3% | 1.5% | - | |
| Unemployment | 6.5% | 7.5% | - | 0.467 |
| Family History of Diabetes | 63.6% | 62.7% | 7 (70%) | 0.656 |
| HbA1c at diagnosis in mmol/mol | 32.2 (29.0–34.4) | 31.15 (27.9–34.4) | 32.2 (30.9–36.1) | 0.171 |
| 75 g ogTT (in mmol/L) | ||||
| Fasting | 5.3 (5.1–5.6) | 5.3 (5.1–5.7) | 5.1 (4.65–5.4) | 0.074 |
| 1 h | 9.7 (8.15–10.7) | 9.6 (8–10.7) | 10.1 (9.3–11) | 0.365 |
| 2 h | 7.5 (6.35–8.85) | 7.45 (6.3–8.8) | 8.1 (7.1–9.15) | 0.224 |
| SCL-90-R T-Scores | ||||
| Somatization (SOM) | 54 (45–59) | 51(43–59) | 64 (59–74) | <0.001 * |
| Obsessive Compulsive (OC) | 53 (43–60) | 50 (43–56) | 67 (63–71) | <0.001 * |
| Interpersonal Sensitivity (IS) | 45 (42–55) | 45 (39–51) | 65 (62–70) | <0.001 * |
| Depression (DEP) | 54 (44–60) | 51 (43–58) | 67 (64–72) | <0.001 * |
| Anxiety (ANX) | 50 (39–59) | 46 (39–56) | 66 (61–80) | <0.001 * |
| Hostility (HOS) | 52 (48–58) | 52 (48–56) | 63 (58–69) | <0.001 * |
| Phobic Anxiety (PHOB) | 44 (43–56) | 43 (43–53) | 67 (59–74) | <0.001 * |
| Paranoid Ideation (PAR) | 48 (40–54) | 40 (40–51) | 69 (63–70) | <0.001 * |
| Psychoticism (PSY) | 43 (43–56) | 43 (43–54) | 65 (60–67) | <0.001 * |
| Global Severity Index (GSI) | 52 (43–58) | 50 (41–56) | 66 (65–72) | <0.001 * |
| Positive Symptom Distress Index (PSDI) | 58 (50–64) | 55 (40–61) | 65 (64–71) | <0.001 * |
| Positive Symptom Total (PST) | 50 (42–56) | 49 (42–53) | 64 (59–67) | <0.001 * |
| Variable | Total Cohort (n = 77) | No Mental Distress (n = 67; 87%) | Mental Distress (n = 10; 13%) | p |
|---|---|---|---|---|
| Hba1c at delivery in mmol/mol | 34.4 (31.1–35.5) | 33.33 (30.6–35.5) | 34.95 (33.03–35.78) | 0.305 |
| Need for Insulin | 41.6% | 40.3% | 50% | 0.733 |
| Treatment methods | 0.14 | |||
| Diet | 58.4% | 59.7% | 50% | |
| Bolus | 1.3% | 1.5% | - | |
| Basal | 29.9% | 31.3% | 20% | |
| Basal and bolus | 10.4% | 7.5% | 30% | |
| Max. Insulin IU/kg | 0.30 (0.19–0.4) | 0.28 (0.18–0.4) | 0.36 (0.2–0.44) | 0.579 |
| Max. number of injections | 1 (1–2.75) | 1 (1–2) | 2 (1.5–4) | 0.201 |
| GWG in kg | 12 (9–16.5) | 12 (8.1–16.2) | 11.3 (9.2–18.1) | 0.939 |
| Pregnancy complications | 13.3% | 15.2% | - | 0.306 |
| Pre-eclampsia/PIH/HELLP | 1.8% | 2% | - | 1 |
| IOL | 41.9% | 42.9% | 33.3% | 1 |
| C-section | 32.3% | 33.9% | 16.7% | 0.654 |
| Birth weight | 3415 (3225–3672) | 3402 (3226–3670) | 3472 (3097–3705) | 0.991 |
| GA at delivery | 39 (38–40) | 39 (38–40) | 38 (38–39) | 0.031 * |
| SGA | 1.6% | 1.8% | - | 1 |
| LGA | 9.8% | 10.9% | - | 1 |
| 5 min APGAR | 9 (9–10) | 9 (9–10) | 9.5 (8.8–10) | 0.454 |
| pH | 7.27 (7.2–7.32) | 7.27 (7.20–7.32) | 7.27 (7.20–7.32) | 0.931 |
| NICU admission | 8.2% | 7.3% | 16.7% | 0.415 |
| hyperbilirubinemia | 35.4% | 36.4% | 25% | 1 |
| hypoglycemia | 14.8% | 14.3% | 20% | 0.567 |
| Respiratory distress | 4.9% | 5.5% | 0 | 1 |
| Variable | Total Cohort (n = 77) | No Mental Distress (n = 67; 87%) | Mental Distress (n = 10; 13%) | p |
|---|---|---|---|---|
| I felt comfortable during pregnancy. | 7 (4–9) | 7 (5–9) | 4.5 (1.5–7.3) | 0.030 * |
| I felt well informed. | 8 (7–10) | 9 (7–10) | 6 (3–10) | 0.133 |
| I felt well cared for during pregnancy. | 9 (8–10) | 9 (8–10) | 7.5 (3–10) | 0.130 |
| The regular ultrasound checks gave me peace of mind. | 10 (8.5–10) | 10 (9–10) | 10 (5.75–10) | 0.458 |
| All my questions about GDM were answered satisfactorily during pregnancy. | 8 (5.5–9.5) | 9 (7–10) | 6 (3–10) | 0.097 |
| During pregnancy, I reached my target blood glucose levels. | 8 (5–9) | 8 (5–9) | 7.5 (3.8–8.3) | 0.501 |
| The reactions in my environment to the diagnosis of GDM surprised me positively. | 4.5 (0–7) | 5 (1.8–7.3) | 0 (0–1.5) | 0.003 * |
| The change in diet was easy for me. | 5 (4–8) | 7 (4–8) | 3.5 (0.8–5.8) | 0.037 * |
| The change in diet was good for me. | 8 (5–9) | 8 (5–9) | 5 (2.8–9.3) | 0.190 |
| I exercised more after being diagnosed with GDM. | 5 (2–8) | 5 (2–8) | 2.5 (1.5–5) | 0.093 |
| The conscious exercise during pregnancy was good for me. | 7 (4–9) | 8 (4–9) | 5 (4.3–6.5) | 0.146 |
| I maintained the lifestyle changes I started during pregnancy after the delivery. | 5 (2–7) | 5 (3–7) | 3 (0.8–5) | 0.054 |
| I was burdened by the diagnosis of GDM. | 7 (3.5–9) | 6 (3–9) | 8 (6.8–10) | 0.048 * |
| I felt burdened by the reactions in my environment to the diagnosis of GDM. | 1 (0–3) | 1 (0–3) | 1 (0–6.8) | 0.708 |
| I was afraid of high values when measuring blood glucose. | 7 (4–8.5) | 6 (4–8) | 9 (6.3–10) | 0.022 * |
| I was afraid of high blood glucose levels when eating. | 8 (2–9) | 7 (2–8) | 10 (8–10) | 0.002 * |
| I was worried that high blood glucose levels would put my child’s health at risk. | 8 (4.5–10) | 8 (3–9) | 10 (8.8–10) | 0.005 * |
| I found it uncomfortable to document and show high blood glucose levels. | 6 (2–8) | 6 (2–8) | 8.5 (5.6–10) | 0.051 |
| I worried about my own health after being diagnosed with GDM. | 6 (3.5–8) | 5 (3–8) | 7 (3.8–10) | 0.313 |
| I worried about my child’s health after being diagnosed with GDM. | 8 (5–10) | 7 (4–10) | 10 (7.8–10) | 0.017 * |
| I was more afraid of giving birth because of the diagnosis of GDM. | 1 (0–2.5) | 1 (0–2) | 2 (0–7.5) | 0.399 |
| I felt restricted in my everyday life by the diagnosis of GDM. | 8 (6.5–10) | 7 (5–10) | 8.5 (6.8–9.3) | 0.370 |
| I felt restricted in my everyday life by the need for regular blood glucose checks. | 8 (6.5–10) | 8 (5–10) | 8.5 (7.8–10) | 0.230 |
| I felt restricted in my everyday life because of the need to inject insulin. | 9 (4.5–10) | 9 (3–9) | 10 (6.5–10) | 0.295 |
| I felt restricted because of the need to watch what I eat. | 7 (5–9) | 7 (4–9) | 8 (6.5–10) | 0.229 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rieß, C.; Heimann, Y.; Schleußner, E.; Groten, T.; Weschenfelder, F. Disease Perception and Mental Health in Pregnancies with Gestational Diabetes—PsychDiab Pilot Study. J. Clin. Med. 2023, 12, 3358. https://doi.org/10.3390/jcm12103358
Rieß C, Heimann Y, Schleußner E, Groten T, Weschenfelder F. Disease Perception and Mental Health in Pregnancies with Gestational Diabetes—PsychDiab Pilot Study. Journal of Clinical Medicine. 2023; 12(10):3358. https://doi.org/10.3390/jcm12103358
Chicago/Turabian StyleRieß, Claudia, Yvonne Heimann, Ekkehard Schleußner, Tanja Groten, and Friederike Weschenfelder. 2023. "Disease Perception and Mental Health in Pregnancies with Gestational Diabetes—PsychDiab Pilot Study" Journal of Clinical Medicine 12, no. 10: 3358. https://doi.org/10.3390/jcm12103358