
Ankle Doppler for Cuffless Ankle Brachial Index Estimation and Peripheral Artery Disease Diagnosis Independent of Diabetes
 , ,
, , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Measurement of Standard ABPI
2.2. Doppler Waveform Analysis
2.3. Reference Duplex Vascular Ultrasound of Lower Extremity Arteries and CT Angiography
2.4. Statistical Analyses
3. Results
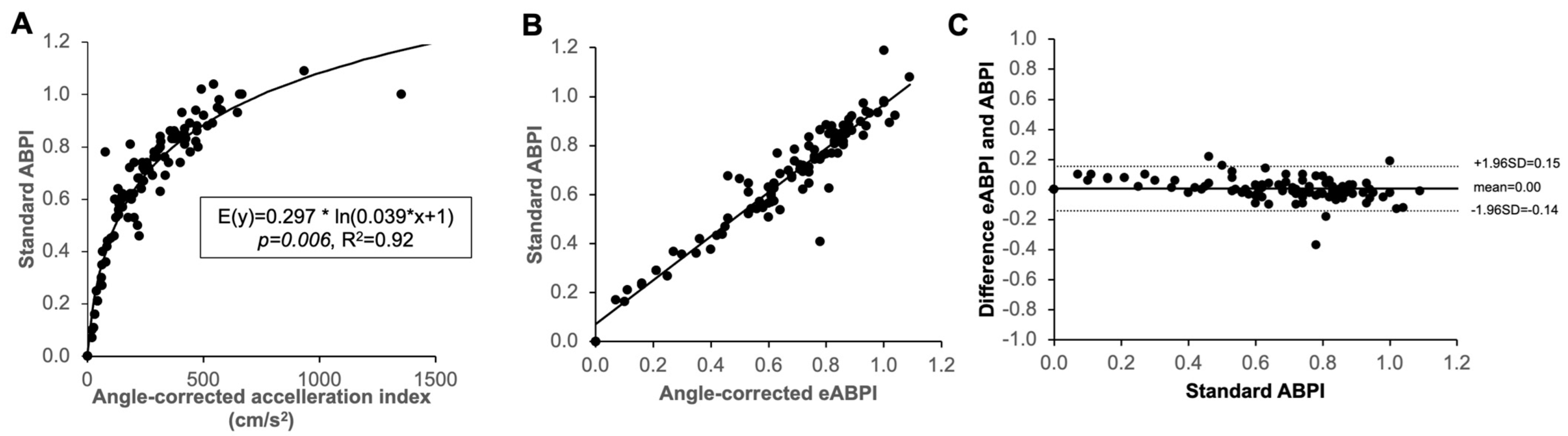
3.1. Association of Handheld Doppler Wave Form Characteristics with Standard ABPI
3.2. Validation of ABPI Estimation with Handheld Doppler
3.3. Establishment of Equation to Calculate eABPI from Angle Corrected Duplex Doppler AccI at the Ankle
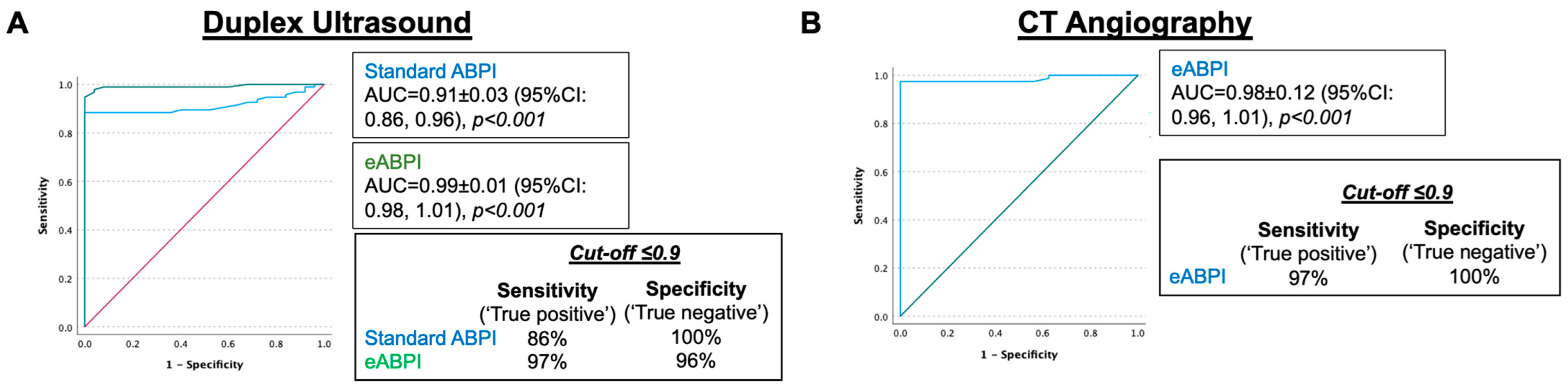
3.4. eABPI Performs Better Than Standard Doppler ABPI to Diagnose PAD Independent of Diabetes
4. Discussion
4.1. Limitations
4.2. Clinical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinecke, H.; Unrath, M.; Freisinger, E.; Bunzemeier, H.; Meyborg, M.; Luders, F.; Gebauer, K.; Roeder, N.; Berger, K.; Malyar, N.M. Peripheral arterial disease and critical limb ischaemia: Still poor outcomes and lack of guideline adherence. Eur. Heart J. 2015, 36, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehm, C.; Schuster, A.; Allenberg, J.R.; Darius, H.; Haberl, R.; Lange, S.; Pittrow, D.; von Stritzky, B.; Tepohl, G.; Trampisch, H.J. High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: Cross-sectional study. Atherosclerosis 2004, 172, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Stoberock, K.; Kaschwich, M.; Nicolay, S.S.; Mahmoud, N.; Heidemann, F.; Rieß, H.C.; Debus, E.S.; Behrendt, C.-A. The interrelationship between diabetes mellitus and peripheral arterial disease—A systematic review. Vasa 2021, 50, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.J.; Sharrett, A.R.; Chambless, L.E.; Rosamond, W.D.; Nieto, F.J.; Sheps, D.S.; Dobs, A.; Evans, G.W.; Heiss, G. Associations of ankle-brachial index with clinical coronary heart disease, stroke and preclinical carotid and popliteal atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. Atherosclerosis 1997, 131, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Belch, J.J.F.; Brodmann, M.; Baumgartner, I.; Binder, C.J.; Casula, M.; Heiss, C.; Kahan, T.; Parini, P.; Poredos, P.; Catapano, A.L.; et al. Lipid-lowering and anti-thrombotic therapy in patients with peripheral arterial disease. Vasa 2021, 50, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Belch, J.J.F.; Baumgartner, I.; Giovas, P.; Hoffmann, U. Morbidity and mortality associated with atherosclerotic peripheral artery disease: A systematic review. Atherosclerosis 2020, 293, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Frank, U.; Nikol, S.; Belch, J.; Boc, V.; Brodmann, M.; Carpentier, P.H.; Chraim, A.; Canning, C.; Dimakakos, E.; Gottsater, A.; et al. ESVM Guideline on peripheral arterial disease. Vasa 2019, 48, 1–79. [Google Scholar] [CrossRef] [Green Version]
- NICE. Peripheral Arterial Disease: Diagnosis and Management [A] Evidence Review for Determining Diagnosis and Severity of PAD in People with Diabetes. Available online: https://www.nice.org.uk/guidance/cg147/evidence/evidence-review-a-determining-diagnosis-and-severity-of-peripheral-arterial-disease-in-people-with-diabetes-pdf-4776839533 (accessed on 1 November 2022).
- Herraiz-Adillo, A.; Cavero-Redondo, I.; Alvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Solera-Martinez, M. The accuracy of toe brachial index and ankle brachial index in the diagnosis of lower limb peripheral arterial disease: A systematic review and meta-analysis. Atherosclerosis 2020, 315, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Sharma, A.M.; Scissons, R.; Dawson, D.; Eberhardt, R.T.; Gerhard-Herman, M.; Hughes, J.P.; Knight, S.; Marie Kupinski, A.; Mahe, G.; et al. Interpretation of peripheral arterial and venous Doppler waveforms: A consensus statement from the Society for Vascular Medicine and Society for Vascular Ultrasound. Vasc. Med. 2020, 25, 484–506. [Google Scholar] [CrossRef] [PubMed]
- Trihan, J.E.; Mahe, G.; Croquette, M.; Coutant, V.; Thollot, C.; Guillaumat, J.; Laneelle, D. Accuracy of Acceleration Time of Distal Arteries to Diagnose Severe Peripheral Arterial Disease. Front. Cardiovasc. Med. 2021, 8, 744354. [Google Scholar] [CrossRef] [PubMed]
- Lanzer, P.; Boehm, M.; Sorribas, V.; Thiriet, M.; Janzen, J.; Zeller, T.; St Hilaire, C.; Shanahan, C. Medial vascular calcification revisited: Review and perspectives. Eur. Heart J. 2014, 35, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Olinic, D.M.; Belch, J.J.F.; Brodmann, M.; Mazzolai, L.; Stanek, A.; Madaric, J.; Krentz, A.; Schlager, O.; Lichtenberg, M.; et al. Management of chronic peripheral artery disease patients with indication for endovascular revascularization. Vasa 2022, 51, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: The European Stroke Organization (ESO). The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooke, T.W.; Hirsch, A.T.; Misra, S.; Sidawy, A.N.; Beckman, J.A.; Findeiss, L.K.; Golzarian, J.; Gornik, H.L.; Halperin, J.L.; Jaff, M.R.; et al. 2011 ACCF/AHA Focused Update of the Guideline for the Management of patients with peripheral artery disease (Updating the 2005 Guideline): A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2011, 124, 2020–2045. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahe, G.; Boulon, C.; Desormais, I.; Lacroix, P.; Bressollette, L.; Guilmot, J.L.; Le Hello, C.; Sevestre, M.A.; Pernod, G.; Constans, J.; et al. Statement for Doppler waveforms analysis. Vasa 2017, 46, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manu, C.A.; Freedman, B.; Rashid, H.; Winkley, K.; Edmonds, M.E. Peripheral Arterial Disease Located in the Feet of Patients with Diabetes and Foot Ulceration Demands a New Approach to the Assessment of Ischemia. Int. J. Low. Extrem. Wounds 2020, 21, 1534734620947979. [Google Scholar] [CrossRef] [PubMed]
- Barshes, N.R.; Flores, E.; Belkin, M.; Kougias, P.; Armstrong, D.G.; Mills, J.L., Sr. The accuracy and cost-effectiveness of strategies used to identify peripheral artery disease among patients with diabetic foot ulcers. J. Vasc. Surg. 2016, 64, 1682–1690.e1683. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Limbs (n) | 148 | |
| Patients (n) | 85 | |
| Vascular ultrasound (n) | 148 | 85 |
| CTA (n) | 120 (81%) | 57 (67%) |
| Standard ABPI (n) | 129 (87%) | 77 (91%) |
| Standard ABPI ≤1.1 (n) | 100 (68%) | 60 (78%) |
| PAD based on ultrasound (n) | 111 (75%) | 65 (76%) |
| PAD based on CTA (n) | 86 (72%) | 48 (56%) |
| Rutherford 0–2 (n) | 6 (4%) | 2 (2%) |
| Rutherford 3 (n) | 24 (16%) | 16 (19%) |
| Rutherford 4 (n) | 13 (9%) | 6 (7%) |
| Rutherford 5 (n) | 64 (43%) | 39 (46%) |
| Chronic limb-threatening ischaemia (n) | 67 (52%) | 45 (53%) |
| Post angioplasty (n) | 9 (6%) | 2 (2%) |
| Age (years) | 70 ± 11 | 70 ± 12 |
| Diabetes mellitus (n) | 76 (51%) | 45 (53%) |
| Type 1 (n) | 8 (5%) | 4 (5%) |
| Type 2 (n) | 65 (44%) | 39 (46%) |
| Unknown type (n) | 3 (2%) | 2 (2%) |
| Arterial hypertension (n) | 109 (74%) | 63 (74%) |
| Chronic obstructive pulmonary disease (n) | 32 (22%) | 17 (20%) |
| Coronary artery disease (n) | 50 (34%) | 30 (35%) |
| Chronic heart failure (n) | 30 (20%) | 18 (21%) |
| Chronic kidney disease (n) | 72 (49%) | 42 (49%) |
| Stroke (n) | 16 (11%) | 10 (12%) |
| Cancer (n) | 15 (10%) | 9 (11%) |
| Abdominal aortic aneurysm (n) | 3 (2%) | 2 (2%) |
| Atrial fibrillation (n) | 27 (18%) | 16 (19%) |
| Smoker (n) | 29 (20%) | 17 (20%) |
| Ex-Smoker (n) | 85 (57%) | 51 (60%) |
| Not Diabetes Mellitus | Diabetes Mellitus | p | |
|---|---|---|---|
| Limbs (n) | 65 | 83 | |
| Patients (n) | 40 | 45 | |
| Vascular ultrasound (n) | 65 (100%) | 83 (100%) | |
| CT angiogram (n) | 49 (75%) | 53 (64%) | |
| Standard ABPI (n) | 50 (77%) | 79 (95%) | |
| Standard ABPI | 0.77 ± 0.38 | 0.83 ± 0.34 | 0.225 |
| AccI (cm/s2) | 419 ± 321 | 384 ± 291 | 0.113 |
| eABPI | 0.74 ± 0.29 | 0.74 ± 0.25 | 0.078 |
| PAD based on ultrasound (n) | 43 (66%) | 68 (82%) | |
| PAD based on CTA (n) | 36 (73%) | 50 (94%) | |
| Rutherford 0–2 (n) | 3 (4%) | 3 (4%) | |
| Rutherford 3 (n) | 17 (20%) | 7 (8%) | |
| Rutherford 4 (n) | 11 (13%) | 2 (2%) | |
| Rutherford 5 (n) | 12 (14%) | 52 (63) | |
| Chronic limb-threatening ischaemia (n) | 23 (28%) | 54 (65%) | |
| Post angioplasty (n) | 4 (5%) | 5 (6%) | |
| Age (years) | 71 ± 10 | 69 ± 12 | 0.289 |
| Arterial hypertension (n) | 42 (51%) | 67 (81%) | |
| Chronic pulmonary disease (n) | 13 (16%) | 19 (23%) | |
| Coronary artery disease (n) | 14 (17%) | 36 (43%) | |
| Chronic heart failure (n) | 9 (11%) | 21 (25%) | |
| Chronic kidney disease (n) | 24 (19%) | 48 (58%) | |
| Stroke (n) | 4 (5%) | 12 (14%) | |
| Cancer (n) | 7 (8%) | 8 (10%) | |
| Abdominal aortic aneurysm (n) | 2 (2%) | 1 (1%) | |
| Atrial fibrillation (n) | 15 (18%) | 12 (14%) | |
| Smoker (n) | 15 (18%) | 14 (17%) | |
| Ex-Smoker (n) | 33 (40%) | 52 (63%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodway, A.D.; Cheal, D.; Allan, C.; Pazos-Casal, F.; Hanna, L.; Field, B.C.T.; Pankhania, A.; Aston, P.J.; Skene, S.S.; Maytham, G.D.; et al. Ankle Doppler for Cuffless Ankle Brachial Index Estimation and Peripheral Artery Disease Diagnosis Independent of Diabetes. J. Clin. Med. 2023, 12, 97. https://doi.org/10.3390/jcm12010097
Rodway AD, Cheal D, Allan C, Pazos-Casal F, Hanna L, Field BCT, Pankhania A, Aston PJ, Skene SS, Maytham GD, et al. Ankle Doppler for Cuffless Ankle Brachial Index Estimation and Peripheral Artery Disease Diagnosis Independent of Diabetes. Journal of Clinical Medicine. 2023; 12(1):97. https://doi.org/10.3390/jcm12010097
Chicago/Turabian StyleRodway, Alexander D., Darren Cheal, Charlotte Allan, Felipe Pazos-Casal, Lydia Hanna, Benjamin C. T. Field, Ajay Pankhania, Philip J. Aston, Simon S. Skene, Gary D. Maytham, and et al. 2023. "Ankle Doppler for Cuffless Ankle Brachial Index Estimation and Peripheral Artery Disease Diagnosis Independent of Diabetes" Journal of Clinical Medicine 12, no. 1: 97. https://doi.org/10.3390/jcm12010097