
Telerehabilitation Approaches for People with Chronic Heart Failure: A Systematic Review and Meta-Analysis
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Interventions
2.3. Information Sources and Study Selection
2.4. Selection and Data Collection Process
2.5. Study Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Risk of Bias in Studies
3.3. Participants
3.4. Telerehabilitation Intervention Descriptors
3.5. Telerehabilitation Actions
3.6. Telerehabilitation Technology
3.7. Telerehabilitation Adherence and Safety
3.8. Efficacy of Telerehabilitation
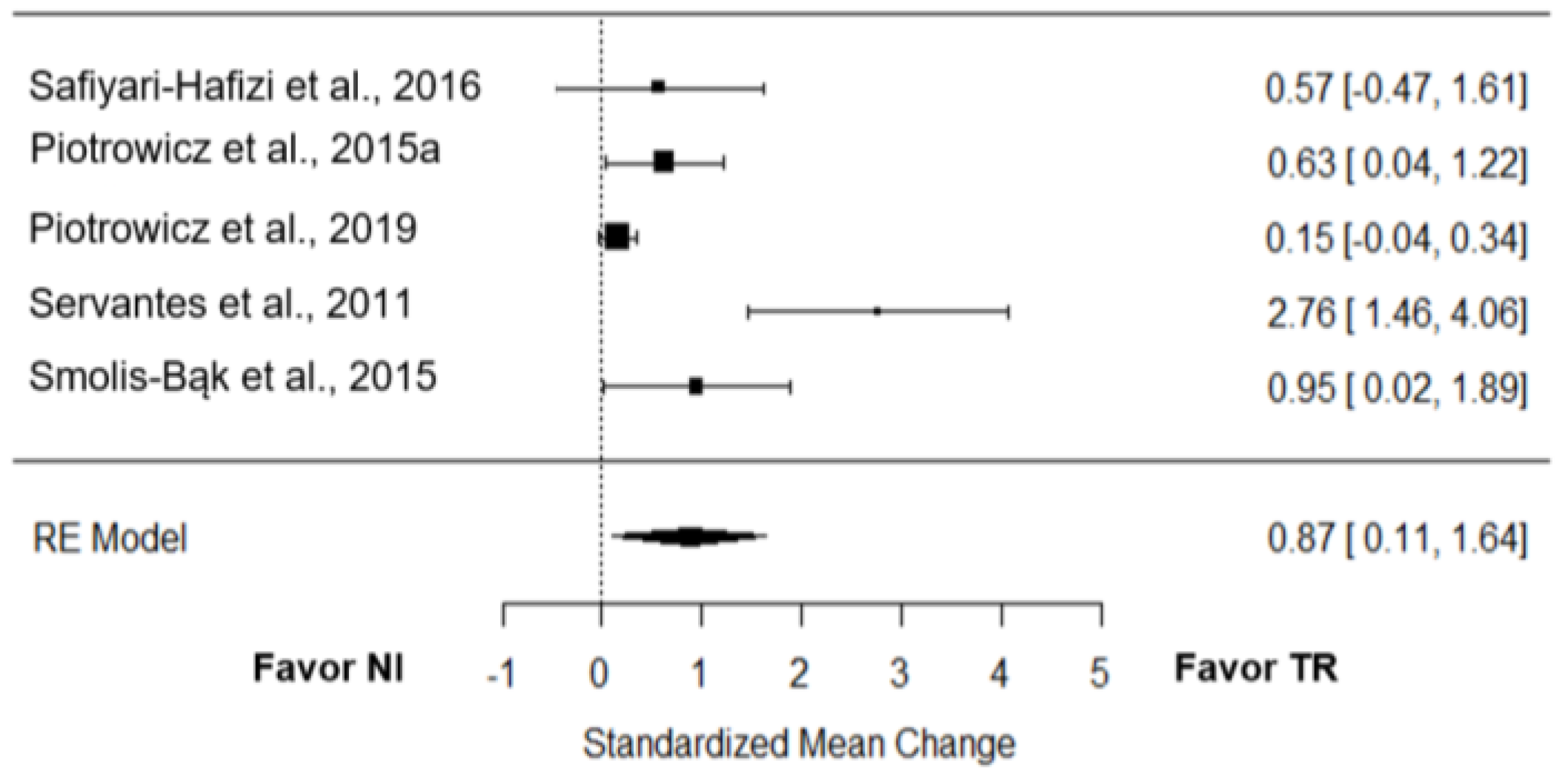
3.8.1. Functional Capacity
3.8.2. Quality of Life
4. Discussion
4.1. Telerehabilitation Intervention Descriptors
4.2. Telerehabilitation Technology and Actions
4.3. Telerehabilitation Safety and Adherence
4.4. Telerehabilitation Effect
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ziaeian, B.; Fonarow, G.C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 2016, 13, 368–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019, 140, e69–e89. [Google Scholar] [CrossRef] [PubMed]
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, CD003331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldridge, N.; Pakosh, M.; Grace, S.L. A systematic review of recent cardiac rehabilitation meta-analyses in patients with coronary heart disease or heart failure. Future Cardiol. 2019, 15, 227–249. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Bowles, K.A.; Lane, R.; Morphet, J. Barriers to Engagement in Chronic Heart Failure Rehabilitation: An Australian Survey. Heart Lung Circ. 2020, 29, e177–e184. [Google Scholar] [CrossRef] [PubMed]
- Buckingham, S.A.; Taylor, R.S.; Jolly, K.; Zawada, A.; Dean, S.G.; Cowie, A.; Norton, R.J.; Dalal, H.M. Home-based versus centre-based cardiac rehabilitation: Abridged Cochrane systematic review and meta-analysis. Open Heart 2016, 3, e000463. [Google Scholar] [CrossRef] [Green Version]
- Bock, B.C.; Carmona-Barros, R.E.; Esler, J.L.; Tilkemeier, P.L. Program participation and physical activity maintenance after cardiac rehabilitation. Behav. Modif. 2003, 27, 37–53. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Topol, E.J. Telemedicine 2020 and the next decade. Lancet 2020, 395, 859. [Google Scholar] [CrossRef]
- Topol, E. The Topol Review. Preparing the Healthcare Workforce to Deliver the Digital Future; NHS: London, UK, 2019. [Google Scholar]
- Isernia, S.; Pagliari, C.; Bianchi, L.N.C.; Banfi, P.I.; Rossetto, F.; Borgnis, F.; Tavanelli, M.; Brambilla, L.; Baglio, F. Characteristics, Components, and Efficacy of Telerehabilitation Approaches for People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15165. [Google Scholar] [CrossRef]
- Di Tella, S.; Pagliari, C.; Blasi, V.; Mendozzi, L.; Rovaris, M.; Baglio, F. Integrated telerehabilitation approach in multiple sclerosis: A systematic review and meta-analysis. J. Telemed. Telecare 2020, 26, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, A.H.; Silva Cardoso, J.; Rocha, A.; Moreira, E.; Azevedo, L.F. Effectiveness of Tele-rehabilitation Programs in Heart Failure: A Systematic Review and Meta-analysis. Health Serv. Insights 2021, 14, 11786329211021668. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid. Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Cowie, A.; Thow, M.K.; Granat, M.H.; Mitchell, S.L. A comparison of home and hospital-based exercise training in heart failure: Immediate and long-term effects upon physical activity level. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 158–166. [Google Scholar] [CrossRef]
- Hwang, R.; Bruning, J.; Morris, N.R.; Mandrusiak, A.; Russell, T. Home-based telerehabilitation is not inferior to a centre-based program in patients with chronic heart failure: A randomised trial. J. Physiother. 2017, 63, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Nagatomi, Y.; Ide, T.; Higuchi, T.; Nezu, T.; Fujino, T.; Tohyama, T.; Nagata, T.; Higo, T.; Hashimoto, T.; Matsushima, S.; et al. Home-based cardiac rehabilitation using information and communication technology for heart failure patients with frailty. ESC Heart Fail. 2022, 9, 2407–2418. [Google Scholar] [CrossRef]
- Peng, X.; Su, Y.; Hu, Z.; Sun, X.; Li, X.; Dolansky, M.A.; Qu, M.; Hu, X. Home-based telehealth exercise training program in Chinese patients with heart failure: A randomized controlled trial. Medicine 2018, 97, e12069. [Google Scholar] [CrossRef]
- Piotrowicz, E.; Zieliński, T.; Bodalski, R.; Rywik, T.; Dobraszkiewicz-Wasilewska, B.; Sobieszczańska-Małek, M.; Stepnowska, M.; Przybylski, A.; Browarek, A.; Szumowski, Ł.; et al. Home-based telemonitored Nordic walking training is well accepted, safe, effective and has high adherence among heart failure patients, including those with cardiovascular implantable electronic devices: A randomised controlled study. Eur. J. Prev. Cardiol. 2015, 22, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Buchner, T.; Piotrowski, W.; Piotrowicz, R. Influence of home-based telemonitored Nordic walking training on autonomic nervous system balance in heart failure patients. Arch. Med. Sci. 2015, 11, 1205–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piotrowicz, E.; Pencina, M.J.; Opolski, G.; Zareba, W.; Banach, M.; Kowalik, I.; Orzechowski, P.; Szalewska, D.; Pluta, S.; Glówczynska, R.; et al. Effects of a 9-Week Hybrid Comprehensive Telerehabilitation Program on Long-term Outcomes in Patients With Heart Failure: The Telerehabilitation in Heart Failure Patients (TELEREH-HF) Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Baranowski, R.; Bilinska, M.; Stepnowska, M.; Piotrowska, M.; Wójcik, A.; Korewicki, J.; Chojnowska, L.; Malek, L.A.; Klopotowski, M.; et al. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: Effectiveness, quality of life, and adherence. Eur. J. Heart Fail. 2010, 12, 164–171. [Google Scholar] [CrossRef]
- Safiyari-Hafizi, H.; Taunton, J.; Ignaszewski, A.; Warburton, D.E. The Health Benefits of a 12-Week Home-Based Interval Training Cardiac Rehabilitation Program in Patients with Heart Failure. Can. J. Cardiol. 2016, 32, 561–567. [Google Scholar] [CrossRef]
- Servantes, D.M.; Pelcerman, A.; Salvetti, X.M.; Salles, A.F.; de Albuquerque, P.F.; de Salles, F.C.; Lopes, C.; de Mello, M.T.; Almeida, D.R.; Filho, J.A. Effects of home-based exercise training for patients with chronic heart failure and sleep apnoea: A randomized comparison of two different programmes. Clin. Rehabil. 2012, 26, 45–57. [Google Scholar] [CrossRef]
- Smolis-Bąk, E.; Dąbrowski, R.; Piotrowicz, E.; Chwyczko, T.; Dobraszkiewicz-Wasilewska, B.; Kowalik, I.; Kazimierska, B.; Jędrzejczyk, B.; Smolis, R.; Gepner, K.; et al. Hospital-based and telemonitoring guided home-based training programs: Effects on exercise tolerance and quality of life in patients with heart failure (NYHA class III) and cardiac resynchronization therapy. A randomized, prospective observation. Int. J. Cardiol. 2015, 199, 442–447. [Google Scholar] [CrossRef]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.M.; Franklin, B.; Sanderson, B.; Southard, D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2007, 115, 2675–2682. [Google Scholar] [CrossRef] [Green Version]
- Matamala-Gomez, M.; Maisto, M.; Montana, J.I.; Mavrodiev, P.A.; Baglio, F.; Rossetto, F.; Mantovani, F.; Riva, G.; Realdon, O. The Role of Engagement in Teleneurorehabilitation: A Systematic Review. Front. Neurol. 2020, 11, 354. [Google Scholar] [CrossRef]
- Comín-Colet, J.; Enjuanes, C.; Lupón, J.; Cainzos-Achirica, M.; Badosa, N.; Verdú, J.M. Transitions of Care Between Acute and Chronic Heart Failure: Critical Steps in the Design of a Multidisciplinary Care Model for the Prevention of Rehospitalization. Rev. Esp. Cardiol. 2016, 69, 951–961. [Google Scholar] [CrossRef]
- Page, K.; Marwick, T.H.; Lee, R.; Grenfell, R.; Abhayaratna, W.P.; Aggarwal, A.; Briffa, T.G.; Cameron, J.; Davidson, P.M.; Driscoll, A.; et al. A systematic approach to chronic heart failure care: A consensus statement. Med. J. Aust. 2014, 201, 146–150. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Tot |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eligibility | Randomization | Allocation | Groups Similarity at Baseline | Assessor Blinding | Outcome Measures | Intention-to-Treat | Between Group Statistical Comparison | Point Measures and Measures of Variability | Activity Monitoring in Control Group | Exercise Intensity Remained Constant | Exercise Volume and Energy Expenditure | ||
| [18] | 1 | 1 | 1 | 1 | 0 | 2 | 0 | 1 | 1 | 0 | 1 | 1 | 10 |
| [19] | 1 | 1 | 1 | 1 | 1 | 3 | 1 | 2 | 1 | 1 | 1 | 1 | 15 |
| [20] | 1 | 1 | 0 | 1 | 0 | 3 | 1 | 2 | 1 | 0 | 1 | 1 | 12 |
| [21] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 1 | 12 |
| [22] | 1 | 0 | 0 | 0 | 0 | 3 | 0 | 2 | 1 | 0 | 1 | 1 | 9 |
| [23] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 4 |
| [24] | 1 | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 1 | 0 | 1 | 1 | 10 |
| [25] | 1 | 0 | 0 | 1 | 0 | 2 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| [26] | 1 | 0 | 0 | 1 | 1 | 2 | 0 | 1 | 0 | 0 | 1 | 1 | 8 |
| [27] | 1 | 1 | 0 | 1 | 0 | 3 | 0 | 1 | 1 | 1 | 1 | 1 | 11 |
| [28] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 4 |
| Study | Group | Subjects [N] | Sex [N Male; Female] | Age (y) [M; SD] | HFLEF | HF Etiologies | VO2 [M; SD] |
|---|---|---|---|---|---|---|---|
| [18] | TR | 20 | 18; 2 | 65.50; - | 5% Medium; 20% Medium-Reduced; 75% Reduced | 55% Ischemic; 45% non-ischemic | - |
| CI | 20 | 16; 4 | 71.20; - | 15% Medium; 35% Medium-Reduced; 50% Reduced | 75% Ischemic; 25% non-ischemic | - | |
| NI | 20 | 17; 3 | 61.40; - | 20% Medium; 30% Medium-Reduced; 50% Severe | 65% Ischemic; 35% non-ischemic | - | |
| [19] | TR | 24 | 19; 5 | 68.00; 14.00 | Reduced (LVEF% = 36.00 ± 16.00) | 58% Ischemic; 4% valvular; 17% idiopathic dilated cardiomyopathy; 13% HF with preserved EF | - |
| CI | 29 | 21; 8 | 67.00; 11.00 | Reduced (LVEF% = 35.00 ± 17.00) | 52% Ischemic; 3% valvular; 21% idiopathic dilated cardiomyopathy; 7% HF with preserved EF | - | |
| [20] | TR | 15 | 9; 6 | 59.80; 10.00 | Medium (LVEF% = 44.50 ± 17.30) | 6% Ischemic; 43% dilated cardiomyopathy; 14% sarcoidosis; 7% amyloidosis; 7% hypertensive; 29% other | - |
| CI | 15 | 7; 8 | 67.70; 8.90 | Reduced (LVEF% = 39.90 ± 17.80) | 20% Ischemic; 25% dilated cardiomyopathy; 25% sarcoidosis; 8% amyloidosis; 17% hypertrophic cardiomyopathy; 25% other | - | |
| [21] | TR | 49 | 28; 21 | - | Reduced (LVEF% = 34.03 ± 6.64) | 61.2% Ischemic; 14.3% valvular; 14.3% idiopathic cardiomyopathy; 10.2% other | - |
| NI | 49 | 30; 19 | - | Reduced (LVEF% = 34.07 ± 6.66) | 59.2% Ischemic; 18.4% valvular; 14.3%; idiopathic cardiomyopathy; 8.1% other | - | |
| [22] | TR | 75 | 64; 11 | 54.40; 10.90 | Reduced (LVEF% = 30.00 ± 8.00) | 66.7% Ischemic; 33.3% non-ischemic | 16.10; 4.00 |
| NI | 32 | 31; 1 | 62.10; 12.50 | Reduced (LVEF% = 34.00 ± 6.00) | 84.4% Ischemic; 15.6% non-ischemic | 17.40; 3.30 | |
| [23] | TR | 36 | 31; 5 | 52.60; 10.12 | Reduced (LVEF% = 32.00 ± 7.00) | 69.4% Ischemic; 30.6% non-ischemic | 16.98; 4.02 |
| NI | 15 | 15; 0 | 61.40; 13.20 | Reduced (LVEF% = 33.00 ± 8.00) | 80.0% Ischemic; 20.0% non-ischemic | 17.90; 3.61 | |
| [24] | TR | 425 | 377; 48 | 62.60; 10.80 | Reduced (LVEF% = 31.00 ± 7.00) | 66.1% Ischemic; 33.9% non-ischemic | 16.9; 6.0 |
| NI | 425 | 376; 49 | 62.20; 10.20 | Reduced (LVEF% = 30.00 ± 7.00) | 64.5% Ischemic; 35.5% non-ischemic | 16.6; 6.0 | |
| [25] | TR | 75 | 64; 11 | 56.40; 10.90 | Reduced (LVEF% = 30.20 ± 8.20) | 73.3% Ischemic; 26.7% non-ischemic | 17.80; 4.10 |
| CI | 56 | 53; 3 | 60.50; 8.80 | Reduced (LVEF% = 30.80 ± 6.70) | 85.7% Ischemic; 14.3% non-ischemic | 17.90; 4.40 | |
| [26] | TR | 20 | 15; 5 | 57.80; 8.10 | Reduced (LVEF% = 27.80 ± 8.80) | - | 10.10; 3.10 |
| NI | 20 | 14; 6 | 58.90; 6.90 | Reduced (LVEF% = 26.00 ± 8.30) | - | 10.10; 2.80 | |
| [27] | TR1 | 17 | - | 51.76; 9.83 | Reduced (LVEF% = 29.59 ± 6.61) | 15.40;2.70 | |
| TR2 | 17 | - | 50.82; 9.45 | Reduced (LVEF% = 31.00 ± 5.02) | - | 15.60; 2.70 | |
| NI | 11 | - | 53.00; 8.19 | Reduced (LVEF% = 31.55 ± 5.77) | - | 15.70; 3.00 | |
| [28] | TR | 26 | 25; 1 | 60.00; 8.50 | Reduced (LVEF% < 35) | 42.6% Ischemic; 34.5% Other, 23.1% Unknown | 13.00; 2.30 |
| NI | 26 | 22; 4 | 65.10; 8.20 | 50.0% Ischemic; 46.2% Other, 3.8% Unknown | 10.70; 3.20 |
| Study | FITT Descriptors | TR APPROACH | Technology | |||
|---|---|---|---|---|---|---|
| Model | Monitoring/ Assessment | Decision | Feedback | |||
| [18] | Frequency: 2 sessions/W for 8 W Intensity: 40–60% HR reserve Time: 60 min Type: I, M (educational + aerobic exercise training) | A | Y | Y | Offline | Device: HR monitor Digital content |
| [19] | Frequency: 2 sessions/W for 12 W Intensity: 9–13 score at perceived exertion scale Time: - Type: G, M (educational + exercise training) | S | Y | Y | Online | Platform: videoconference platform Device: automatic sphygmomanometer, finger pulse oximeter Digital content |
| [20] | Frequency: 5–7 sessions/W for 15 W Intensity: 11–13 score at Borg scale Time: 30–40 min Type: I, M (education + stretching/resistance exercise training) | A | Y | Y | Online/Offline | Device: Fitbit + smartphone Digital content |
| [21] | Frequency: 3–5 sessions/W for 8 W Intensity: 40–70% HR reserve + HR at rest Time: 20–30 min Type: I + G, M (education + aerobic/resistance exercise training) | S | Y | Y | Online | Platform: QQ + WeChat + videoconference platform |
| [25] | Frequency: 3 sessions/W for 8 W Intensity: 40–70% HR reserve + 11 score at Borg scale Time: 45 min Type: I, M (education + psychological support + aerobic/resistance exercise training) | A | Y | Y | Offline | Platform: Data transmission survey Device: EHO 3 device (electrocardiogram) + mobile phone |
| [22] | Frequency: 5 sessions/W for 8 W Intensity: 40–70% HR reserve + Borg scale Time: - Type: I, U (aerobic/resistance exercise training) | A | Y | N | Offline | Platform: Data transmission survey Device: EHO 3 device (electrocardiogram) + mobile phone + blood pressure measuring + weighting machine |
| [23] | Frequency: 5 sessions/W for 8 W Intensity: 40–70% HR reserve + functional capacity at CPET Time: 10–45 min Type: I, M (aerobic/resistance exercise training + respiratory exercise training) | A | Y | Y | Offline | Platform: Data transmission survey Device: EHO 3 device (electrocardiogram) + mobile phone |
| [24] | Frequency: 5 sessions/W for 8 W Intensity: 40–70% HR reserve + 5–10 repetitions for resistance/strength exercises + 30–60% of Pi for respiratory exercises Time: - Type: I, M (aerobic/resistance/strength exercise training + respiratory exercise training) | A | Y | Y | Offline | Platform: Data transmission survey + monitoring platform Device: EHO 3 device (electrocardiogram) + mobile phone + blood pressure device + weighting machine |
| [26] | Frequency: 12 W Intensity: 80–85% VO2 peak followed by 40–50% VO2 peak + moderate intensity for resistance exercises Time: - Type: I, U (aerobic/resistance exercise training) | A | Y | Y | Offline | Device: HR monitor + pedometer |
| [27] | Frequency: 12 W Intensity: HR anaerobic threshold + 30–40% repetition maximum for strength exercises Time: - Type: I, U (aerobic/strength exercise training) | A | Y | Y | Offline | Device: HR monitor + free weights |
| [28] | Frequency: 5 sessions/W for 8 W Intensity: - Time: - Type: I, M (respiratory exercise training + strength/range-of-motion/isometric exercise training) | A | Y | Y | Offline | Platform: Data transmission survey Device: Electrocardiogram recording monitor |
| Outcome | Domain | Subdomain | Tool | Per-Based | Pr-Based | Study |
|---|---|---|---|---|---|---|
| Medical-Benefit | Functional Capacity | Exercise capacity | VO2 peak | x | [22,23,24,25,26,27,28] | |
| Anaerobic threshold | x | [27,28] | ||||
| Exercise tolerance | x | [28] | ||||
| Shuttle walk test | x | [18] | ||||
| 6-min walk distance | x | [19,20,21,22,24,25,26,28] | ||||
| Short physical performance battery | x | [20] | ||||
| Physical activity | activPAL TM | x | [18] | |||
| Strength | dynamometer | x | [19,27] | |||
| Walking speed | 10 m walk test | x | [19] | |||
| Balance | Balance outcome measure for elder rehabilitation | x | [19] | |||
| Sleep | Polysomnography | x | [27] | |||
| Heart function | Heart rate at rest | x | [21,25] | |||
| Heart rate variability/turbulence | x | [23,24] | ||||
| LVEF | x | [21,22,23] | ||||
| NYHA classification | x | [21,25] | ||||
| Echocardiography | x | [28] | ||||
| Brain natriuretic peptide | x | [20] | ||||
| Kansas City Cardiomyopathy Questionnaire | x | [20] | ||||
| Urinary function | Revised Urinary Incontinence Scale | x | [19] | |||
| Frailty | Kihon checklist | x | [20] | |||
| Participation | Quality of life | SF-36 | x | [22,24,25] | ||
| EuroQoL five-dimensional | x | [19] | ||||
| The Minnesota Living with Heart Failure Questionnaire | x | [19,21,26,27] | ||||
| Nottingham Health Profile | x | [28] | ||||
| EuroQol five-dimensional | x | [19] | ||||
| Mood | Hospital anxiety and depression scale | x | [21] | |||
| Beck depression inventory | x | [28] | ||||
| Mortality | [24,25] | |||||
| Patient-Relevant | Adherence | Participation rate | x | [19,20] | ||
| Percentage of patients who carried out the training | x | [22,24,25,26] | ||||
| Safety | Adverse events | x | [19,20,24,25] | |||
| Satisfaction | Client satisfaction questionnaire | x | [19] | |||
| 12-item ad-hoc questionnaire | x | [22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isernia, S.; Pagliari, C.; Morici, N.; Toccafondi, A.; Banfi, P.I.; Rossetto, F.; Borgnis, F.; Tavanelli, M.; Brambilla, L.; Baglio, F., on behalf of the CPTM Group. Telerehabilitation Approaches for People with Chronic Heart Failure: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 64. https://doi.org/10.3390/jcm12010064
Isernia S, Pagliari C, Morici N, Toccafondi A, Banfi PI, Rossetto F, Borgnis F, Tavanelli M, Brambilla L, Baglio F on behalf of the CPTM Group. Telerehabilitation Approaches for People with Chronic Heart Failure: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(1):64. https://doi.org/10.3390/jcm12010064
Chicago/Turabian StyleIsernia, Sara, Chiara Pagliari, Nuccia Morici, Anastasia Toccafondi, Paolo Innocente Banfi, Federica Rossetto, Francesca Borgnis, Monica Tavanelli, Lorenzo Brambilla, and Francesca Baglio on behalf of the CPTM Group. 2023. "Telerehabilitation Approaches for People with Chronic Heart Failure: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 1: 64. https://doi.org/10.3390/jcm12010064