
Involvement of Pharmacists in the Emergency Department to Correct Errors in the Medication History and the Impact on Adverse Drug Event Detection
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
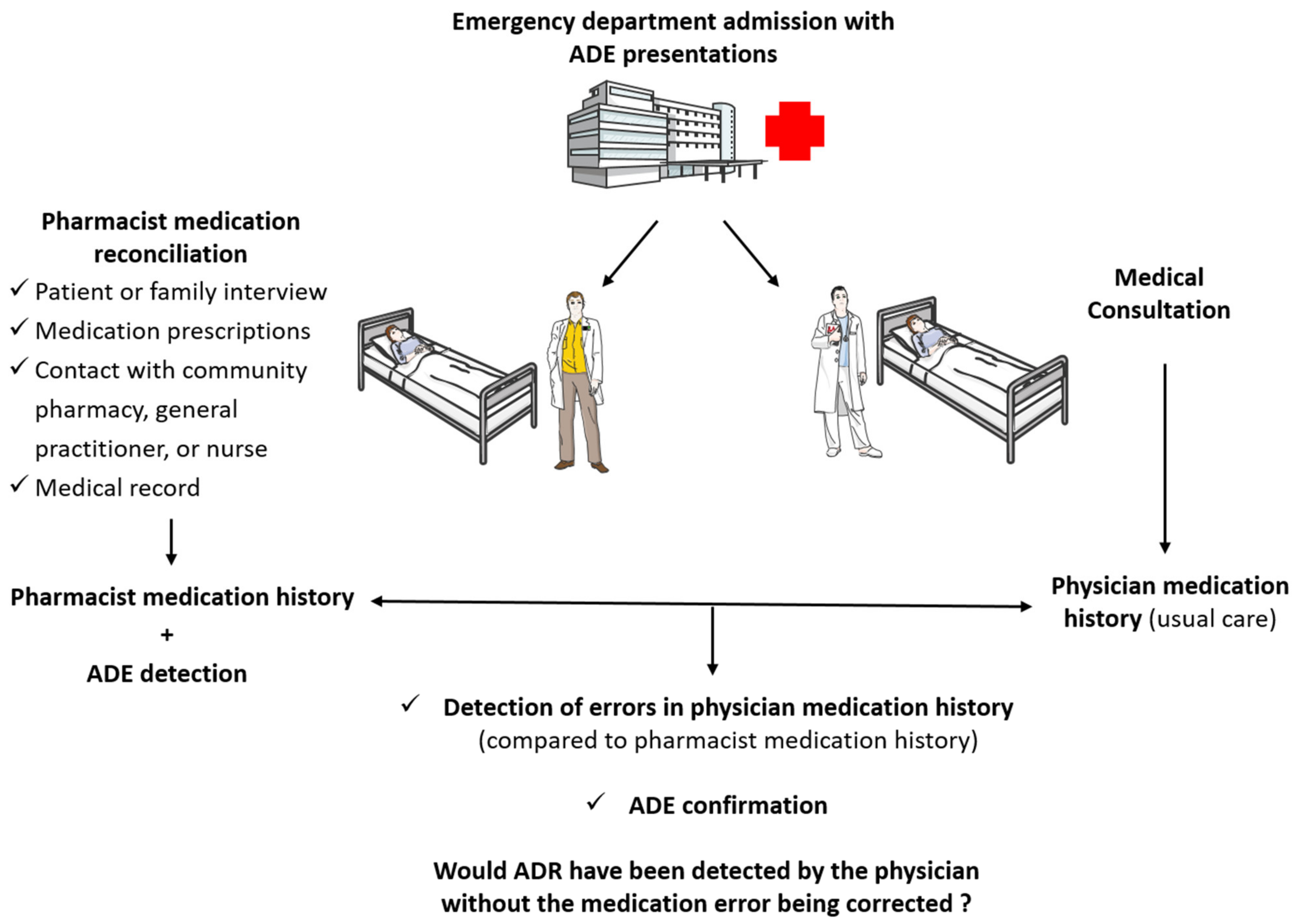
2.1. Study Design and Setting
2.2. Errors on Medication Lists and ADE Detection
2.2.1. Best Possible Medication History
2.2.2. Error Detection
2.2.3. Missed Diagnosis of ADE and Medication List Errors
2.2.4. ADE Detection
2.2.5. Transmission of Information
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Consideration
3. Results
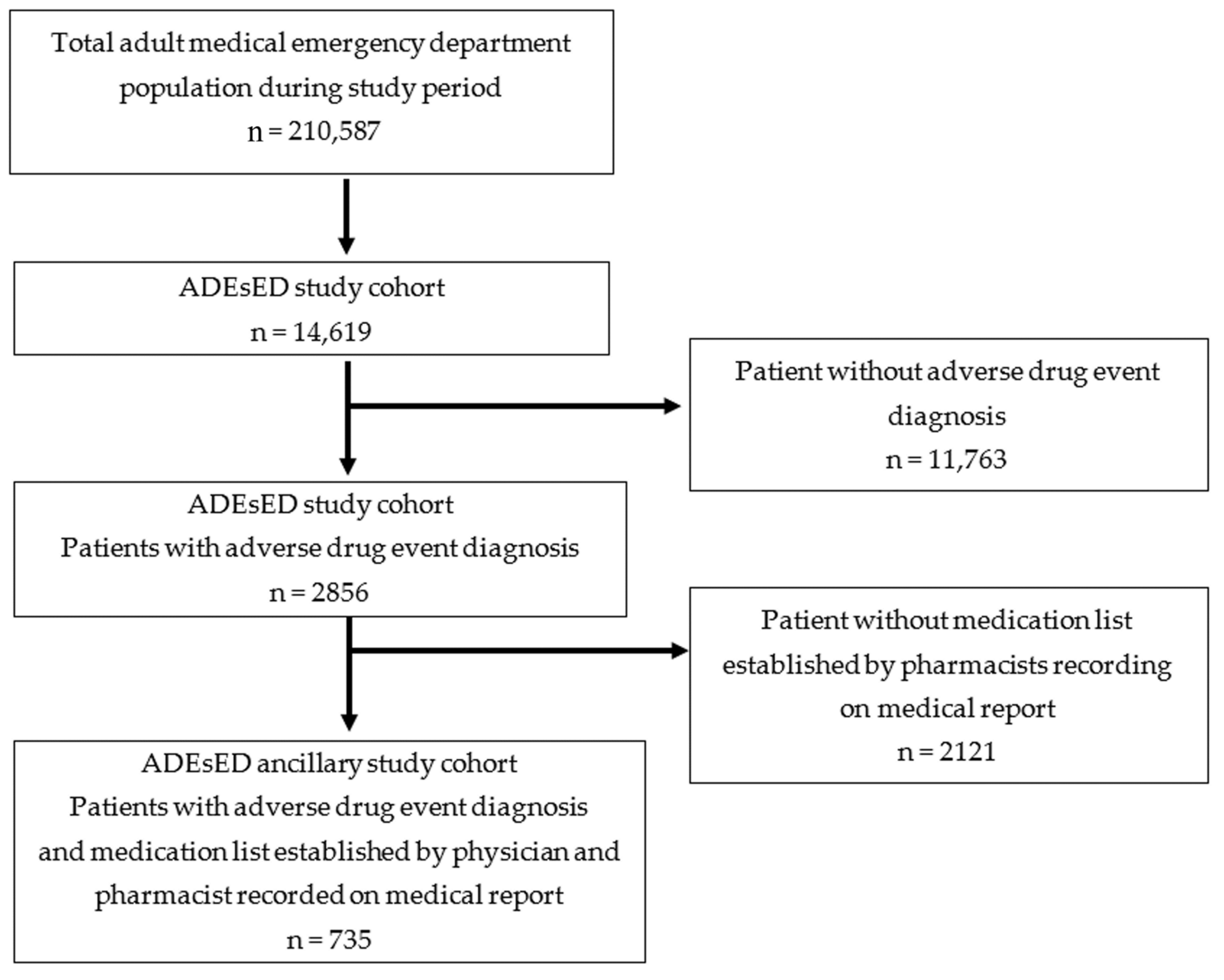
3.1. Characteristics of the Study Population
3.2. Medication Histories Obtained by the Pharmaceutical and Medical Teams
3.3. Medication Histories Obtained by the Pharmaceutical and Medical Teams
3.4. Errors on Medication Lists Obtained by the Medical Team and ADEs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bates, D.W.; Cullen, D.J.; Laird, N.; Petersen, L.A.; Small, S.D.; Servi, D.; Laffel, G.; Sweitzer, B.J.; Shea, B.F.; Hallisey, R.; et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 1995, 274, 29–34. [Google Scholar]
- Nebeker, J.R.; Barach, P.; Samore, M.H. Clarifying adverse drug events: A clinician’s guide to terminology, documentation, and reporting. Ann. Intern. Med. 2004, 140, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Khan, L.M. Comparative epidemiology of hospital-acquired adverse drug reactions in adults and children and their impact on cost and hospital stay—A systematic review. Eur. J. Clin. Pharmacol. 2013, 69, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Hohl, C.M.; Nosyk, B.; Kuramoto, L.; Zed, P.J.; Brubacher, J.R.; Abu-Laban, R.B.; Sheps, S.B.; Sobolev, B. Outcomes of emergency department patients presenting with adverse drug events. Ann. Emerg. Med. 2011, 58, 270–279.e274. [Google Scholar] [CrossRef]
- Lahue, B.J.; Pyenson, B.; Iwasaki, K.; Blumen, H.E.; Forray, S.; Rothschild, J. National burden of preventable adverse drug events associated with inpatient injectable medications: Healthcare and medical professional liability costs. Am. Health Drug Benefits 2012, 5, 1–10. [Google Scholar]
- Martins, A.C.; Giordani, F.; Rozenfeld, S. Adverse drug events among adult inpatients: A meta-analysis of observational studies. J. Clin. Pharm. Ther. 2014, 39, 609–620. [Google Scholar] [CrossRef]
- Tache, S.V.; Sonnichsen, A.; Ashcroft, D.M. Prevalence of adverse drug events in ambulatory care: A systematic review. Ann. Pharmacother. 2011, 45, 977–989. [Google Scholar] [CrossRef]
- Bailey, C.; Peddie, D.; Wickham, M.E.; Badke, K.; Small, S.S.; Doyle-Waters, M.M.; Balka, E.; Hohl, C. Adverse drug event reporting systems: A systematic review. Br. J. Clin. Pharmacol. 2016, 82, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Queneau, P.; Bannwarth, B.; Carpentier, F.; Guliana, J.M.; Bouget, J.; Trombert, B.; Leverve, X.; Lapostolle, F.; Borron, S.; Adnet, F. Association Pedagogique Nationale pour l’Enseignement de la, Emergency department visits caused by adverse drug events: Results of a French survey. Drug Saf. 2007, 30, 81–88. [Google Scholar] [CrossRef]
- Budnitz, D.S.; Lovegrove, M.C.; Shehab, N.; Richards, C.L. Emergency hospitalizations for adverse drug events in older Americans. N. Engl. J. Med. 2011, 365, 2002–2012. [Google Scholar] [CrossRef]
- Santé Publique France, Incidence des Événements Indésirables Graves Associés aux Soins Dans les Établissements de Santé (Eneis 3): Quelle Évolution dix ans Après. Available online: https://www.santepubliquefrance.fr/docs/incidence-des-evenements-indesirables-graves-associes-aux-soins-dans-les-etablissements-de-sante-eneis-3-quelle-evolution-dix-ans-apres (accessed on 20 December 2022).
- Roulet, L.; Asseray, N.; Dary, M.; Chiffoleau, A.; Potel, G.; Ballereau, F. Implementing a clinical pharmacy survey of adverse drug events in a French emergency department. Int. J. Clin. Pharm. 2012, 34, 902–910. [Google Scholar] [CrossRef]
- Hohl, C.M.; Zed, P.J.; Brubacher, J.R.; Abu-Laban, R.B.; Loewen, P.S.; Purssell, R.A. Do emergency physicians attribute drug-related emergency department visits to medication-related problems? Ann. Emerg. Med. 2010, 55, 493–502.e494. [Google Scholar] [CrossRef]
- Stergiopoulos, S.; Brown, C.A.; Felix, T.; Grampp, G.; Getz, K.A. A Survey of Adverse Event Reporting Practices among US Healthcare Professionals. Drug Saf. 2016, 39, 1117–1127. [Google Scholar] [CrossRef] [Green Version]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef]
- Howe, C.L. A review of the Office of Inspector General’s reports on adverse event identification and reporting. J. Healthc. Risk Manag. 2011, 30, 48–54. [Google Scholar] [CrossRef]
- Hohl, C.; Lexchin, J.R.; Balka, E. Can reporting of adverse drug reactions create safer systems while improving health data? CMAJ 2015, 187, 789–790. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, G.; Schwartz, R.B. Frequency of incomplete medication histories obtained at triage. Am. J. Health Syst. Pharm. 2009, 66, 65–69. [Google Scholar] [CrossRef]
- Mazer, M.; Deroos, F.; Hollander, J.E.; McCusker, C.; Peacock, N.; Perrone, J. Medication history taking in emergency department triage is inaccurate and incomplete. Acad. Emerg. Med. 2011, 18, 102–104. [Google Scholar] [CrossRef]
- Tam, V.C.; Knowles, S.R.; Cornish, P.L.; Fine, N.; Marchesano, R.; Etchells, E.E. Frequency, type and clinical importance of medication history errors at admission to hospital: A systematic review. CMAJ 2005, 173, 510–515. [Google Scholar] [CrossRef] [Green Version]
- Caglar, S.; Henneman, P.L.; Blank, F.S.; Smithline, H.A.; Henneman, E.A. Emergency department medication lists are not accurate. J. Emerg. Med. 2011, 40, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Boockvar, K.S.; Liu, S.; Goldstein, N.; Nebeker, J.; Siu, A.; Fried, T. Prescribing discrepancies likely to cause adverse drug events after patient transfer. Qual. Saf. Health Care 2009, 18, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Agence Nationale de Sécurité du Médicament et des Produits de Santé, Qu’est ce Qu’une Erreur Médicamenteuse? Available online: https://archiveansm.integra.fr/Declarer-un-effet-indesirable/Erreurs-medicamenteuses/Qu-est-ce-qu-une-erreur-medicamenteuse/(offset)/0 (accessed on 28 December 2022).
- Breuker, C.; Abraham, O.; di Trapanie, L.; Mura, T.; Macioce, V.; Boegner, C.; Jalabert, A.; Villiet, M.; Castet-Nicolas, A.; Avignon, A.; et al. Patients with diabetes are at high risk of serious medication errors at hospital: Interest of clinical pharmacist intervention to improve healthcare. Eur. J. Intern. Med. 2017, 38, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, J.W.; Grgurich, P.E. Impact of students pharmacists on the medication reconciliation process in high-risk hospitalized general medicine patients. Am. J. Pharm. Educ. 2014, 78, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathys, M.; Neyland-Turner, E.; Hamouie, K.; Kim, E. Effect of pharmacy students as primary pharmacy members on inpatient interdisciplinary mental health teams. Am. J. Health Syst. Pharm. 2015, 72, 663–667. [Google Scholar] [CrossRef]
- Mergenhagen, K.A.; Blum, S.S.; Kugler, A.; Livote, E.E.; Nebeker, J.R.; Ott, M.C.; Signor, D.; Sung, S.; Yeh, J.; Boockvar, K.S. Pharmacist—versus physician—initiated admission medication reconciliation: Impact on adverse drug events. Am. J. Geriatr. Pharmacother. 2012, 10, 242–250. [Google Scholar] [CrossRef]
- Arrison, W.; Merritt, E.; Powell, A. Comparing medication histories obtained by pharmacy technicians and nursing staff in the emergency department. Res. Social Adm. Pharm. 2020, 16, 1398–1400. [Google Scholar] [CrossRef]
- Greenwood, D.; Steinke, D.; Martin, S.; Tully, M.P. Development of an Emergency Department Pharmacist Practitioner service specification. Res. Soc. Adm. Pharm. 2021, 17, 1140–1150. [Google Scholar] [CrossRef]
- Roulet, L.; Ballereau, F.; Hardouin, J.B.; Chiffoleau, A.; Moret, L.; Potel, G.; Asseray, N. Assessment of adverse drug event recognition by emergency physicians in a French teaching hospital. Emerg. Med. J. 2013, 30, 63–67. [Google Scholar] [CrossRef]
- Roulet, L.; Asseray, N.; Ballereau, F. Establishing a pharmacy presence in the emergency department: Opportunities and challenges in the French setting. Int. J. Clin. Pharm. 2014, 36, 471–475. [Google Scholar] [CrossRef]
- Leenhardt, F.; Perier, D.; Pinzani, V.; Giraud, I.; Villiet, M.; Castet-Nicolas, A.; Gourhant, V.; Breuker, C. Pharmacist intervention to detect drug adverse events on admission to the emergency department: Two case reports of neuroleptic malignant syndrome. J. Clin. Pharm. Ther. 2017, 42, 502–505. [Google Scholar] [CrossRef]
- Laureau, M.; Vuillot, O.; Gourhant, V.; Perier, D.; Pinzani, V.; Lohan, L.; Faucanie, M.; Macioce, V.; Marin, G.; Giraud, I.; et al. Adverse Drug Events Detected by Clinical Pharmacists in an Emergency Department: A Prospective Monocentric Observational Study. J. Patient Saf. 2021, 17, e1040–e1049. [Google Scholar] [CrossRef]
- Lohan, L.; Marin, G.; Faucanie, M.; Laureau, M.; Macioce, V.; Perier, D.; Pinzani, V.; Giraud, I.; Castet-Nicolas, A.; Jalabert, A.; et al. Impact of medication characteristics and adverse drug events on hospital admission after an emergency department visit: Prospective cohort study. Int. J. Clin. Pract. 2021, 75, e14224. [Google Scholar] [CrossRef]
- Lohan, L.; Marin, G.; Faucanie, M.; Laureau, M.; Perier, D.; Pinzani, V.; Giraud, I.; Villiet, M.; Sebbane, M.; Sultan, A.; et al. Frequency, Characteristics, and Predictive Factors of Adverse Drug Events in an Adult Emergency Department according to Age: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 5731. [Google Scholar] [CrossRef]
- Breuker, C.; Macioce, V.; Mura, T.; Castet-Nicolas, A.; Audurier, Y.; Boegner, C.; Jalabert, A.; Villiet, M.; Avignon, A.; Sultan, A. Medication Errors at Hospital Admission and Discharge: Risk Factors and Impact of Medication Reconciliation Process to Improve Healthcare. J. Patient Saf. 2021, 17, e645–e652. [Google Scholar] [CrossRef]
- van den Bemt, P.M.; van der Schrieck-de Loos, E.M.; van der Linden, C.; Theeuwes, A.M.; Pol, A.G.; Dutch CBO WHO. Effect of medication reconciliation on unintentional medication discrepancies in acute hospital admissions of elderly adults: A multicenter study. J. Am. Geriatr. Soc. 2013, 61, 1262–1268. [Google Scholar] [CrossRef]
- Arimone, Y.; Bidault, I.; Dutertre, J.P.; Gerardin, M.; Guy, C.; Haramburu, F.; Hillaire-Buys, D.; Meglio, C.; Penfornis, C.; Theophile, H.; et al. Updating the French method for the causality assessment of adverse drug reactions. Therapie 2013, 68, 69–76. [Google Scholar] [CrossRef]
- Trotti, A.; Colevas, A.D.; Setser, A.; Rusch, V.; Jaques, D.; Budach, V.; Langer, C.; Murphy, B.; Cumberlin, R.; Coleman, C.N.; et al. CTCAE v3.0: Development of a comprehensive grading system for the adverse effects of cancer treatment. Semin. Radiat. Oncol. 2003, 13, 176–181. [Google Scholar] [CrossRef]
- De Winter, S.; Spriet, I.; Indevuyst, C.; Vanbrabant, P.; Desruelles, D.; Sabbe, M.; Gillet, J.B.; Wilmer, A.; Willems, L. Pharmacist- versus physician-acquired medication history: A prospective study at the emergency department. Qual. Saf. Health Care 2010, 19, 371–375. [Google Scholar] [CrossRef]
- Miller, S.M.; Miller, S.; Balon, J.; Helling, T.S. Medication reconciliation in a rural trauma population. Ann. Emerg. Med. 2008, 52, 483–491. [Google Scholar] [CrossRef]
- Gleason, K.M.; Groszek, J.M.; Sullivan, C.; Rooney, D.; Barnard, C.; Noskin, G.A. Reconciliation of discrepancies in medication histories and admission orders of newly hospitalized patients. Am. J. Health Syst. Pharm. 2004, 61, 1689–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, V.; Jellinek, S.P.; Likourezos, A.; Nemeth, I.; Paul, T.; Murphy, D. Variation in medication information for elderly patients during initial interventions by emergency department physicians. Am. J. Health Syst. Pharm. 2008, 65, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.K.; Allin, D.M.; Scott, L.A.; Grauer, D. Pharmacist-acquired medication histories in a university hospital emergency department. Am. J. Health Syst. Pharm. 2006, 63, 2500–2503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzsimons, M.; Grimes, T.; Galvin, M. Sources of pre-admission medication information: Observational study of accuracy and availability. Int. J. Pharm. Pract. 2011, 19, 408–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornish, P.L.; Knowles, S.R.; Marchesano, R.; Tam, V.; Shadowitz, S.; Juurlink, D.N.; Etchells, E.E. Unintended medication discrepancies at the time of hospital admission. Arch. Intern. Med. 2005, 165, 424–429. [Google Scholar] [CrossRef]
- Lau, H.S.; Florax, C.; Porsius, A.J.; De Boer, A. The completeness of medication histories in hospital medical records of patients admitted to general internal medicine wards. Br. J. Clin. Pharmacol. 2000, 49, 597–603. [Google Scholar] [CrossRef]
- Vira, T.; Colquhoun, M.; Etchells, E. Reconcilable differences: Correcting medication errors at hospital admission and discharge. Qual. Saf. Health Care 2006, 15, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Balon, J.; Thomas, S.A. Comparison of hospital admission medication lists with primary care physician and outpatient pharmacy lists. J. Nurs. Scholarsh. 2011, 43, 292–300. [Google Scholar] [CrossRef]
- Marvin, V.; Kuo, S.; Poots, A.J.; Woodcock, T.; Vaughan, L.; Bell, D. Applying quality improvement methods to address gaps in medicines reconciliation at transfers of care from an acute UK hospital. BMJ Open 2016, 6, e010230. [Google Scholar] [CrossRef] [Green Version]
- Uitvlugt, E.B.; Suijker, R.; Janssen, M.J.A.; Siegert, C.E.H.; Karapinar-Carkit, F. Quality of medication related information in discharge letters: A prospective cohort study. Eur. J. Intern. Med. 2017, 46, e23–e25. [Google Scholar] [CrossRef]
- Zhang, M.; Holman, C.D.; Price, S.D.; Sanfilippo, F.M.; Preen, D.B.; Bulsara, M.K. Comorbidity and repeat admission to hospital for adverse drug reactions in older adults: Retrospective cohort study. BMJ 2009, 338, a2752. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Aguila, S.; Contel, J.C.; Farre, J.; Campuzano, J.L.; Rajmil, L. Predictive model for emergency hospital admission and 6-month readmission. Am. J. Manag Care. 2011, 17, e348-57. [Google Scholar]
- Breuker, C.; Faucanie, M.; Laureau, M.; Perier, D.; Pinzani, V.; Marin, G.; Sebbane, M.; Villiet, M. Impact of a medico-pharmaceutical follow-up and an optimized communication between hospital and community on the readmission to the emergency department for an adverse drug event: URGEIM, study protocol for a randomized controlled trial. Trials 2021, 22, 521. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 735) |
|---|---|
| Age (years) | 74.3 ± 17.4 |
| Gender, male | 369 (50.2) |
| FRENCH triage scale | |
| Level 1 | 40 (5.4) |
| Level 2 | 111 (15.1) |
| Level 3 | 384 (52.2) |
| Level 4 | 136 (18.5) |
| Level 5 | 64 (8.7) |
| Main cause of ED visit | |
| Neurological disorders | 149 (20.3) |
| Bleeding | 101 (13.7) |
| Falling | 94 (12.8) |
| Hepato-gastrointestinal disorders | 91 (12.4) |
| Pulmonary disorders | 71 (9.7) |
| Cardiovascular disorders | 61 (8.3) |
| Alteration of the general condition | 58 (7.9) |
| Abnormality of biological results | 28 (3.8) |
| Metabolic disorders | 20 (2.7) |
| Other | 62 (8.4) |
| ADE symptoms | |
| Bleeding | 197 (26.8) |
| Metabolic disorders | 114 (15.5) |
| Neurological disorders | 110 (15.0) |
| Cardiovascular disorders | 84 (11.4) |
| Hepato-gastrointestinal disorders | 75 (10.2) |
| Hematology and coagulation test abnormalities | 75 (10.2) |
| Skin diseases | 22 (3.0) |
| Fatigue/fall | 21 (2.9) |
| Other | 37 (5.0) |
| ADE severity | |
| Spontaneous regression | 51 (6.9) |
| Regression after symptomatic treatment | 310 (42.2) |
| Hospitalization with no life threat | 288 (39.2) |
| Hospitalization with life-threatening risk | 51 (6.9) |
| Death | 1.5 (2.0) |
| Undetermined | 20 (2.7) |
| ED visit outcome | |
| Discharge | 346 (47.1) |
| Hospitalization | 379 (51.6) |
| Death | 10 (1.4) |
| Total (n = 735) | |
|---|---|
| Number of sources used by clinical pharmacy team | 2.9 ± 0.6 |
| Type of information sources used by clinical pharmacy team | |
| Personal source (patient, family or entourage) | 557 (75.8) |
| Medication prescription (or general practitioner referral letter, nursing home emergency liaison record, ambulance sheet, medications brough in, etc.) | 718 (97.7) |
| Computerized medical file | 117 (15.9) |
| Community pharmacist | 566 (77.0) |
| General practitioner | 77 (10.5) |
| Nurse | 97 (13.2) |
| Number of daily medications | |
| Medication list made by emergency physicians | 6.6 ± 3.9 |
| Medication list made by pharmacists | 8.8 ± 4.1 |
| Errors on medication lists | |
| Patients with at least one error | 684 (93.1) |
| Patient with an error regarding at least one drug involved in an ADE | 420 (57.1) |
| Number of errors per patient | 5.7 ± 4.1 |
| Total Medications n = 6108 | Total Medications with Error n = 4186 | Errors Concerning ADE Medication n = 537 |
|---|---|---|
| Medication involved in errors | ||
| Alimentary tract and metabolism | 935 (22.3) | 47 (8.8) |
| Blood and blood-forming organs | 402 (9.6) | 152 (28.3) |
| Cardiovascular system | 838 (20.0) | 94 (17.5) |
| Dermatological | 64 (1.5) | 0 (0) |
| Genito-urinary system and sex hormones | 108 (2.6) | 11 (2.0) |
| Systemic hormonal preparations | 104 (2.5) | 8 (1.5) |
| Anti-infective drugs for systemic use | 155 (3.7) | 38 (7.1) |
| Antineoplastic and immunomodulating agents | 34 (0.8) | 5 (0.9) |
| Muscular-skeletal system | 124 (3.0) | 10 (1.9) |
| Nervous system | 1088 (26.0) | 162 (30.2) |
| Respiratory system | 206 (4.9) | 8 (1.5) |
| Sensory organs | 102 (2.4) | 0 (0) |
| Other | 26 (0.6) | 2 (0.4) |
| Type of errors | ||
| Added medication | 350 (8.4) | NA |
| Missing medication * | ||
| Omission | 2014 (48.1) | 225 (41.9) |
| Wrong molecule | 71 (1.7) | 17 (3.2) |
| Mischaracterization ** | ||
| Wrong dose | 121 (2.9) | 30 (5.6) |
| Wrong frequency | 187 (4.5) | 47 (8.8) |
| Dosage omission | 103 (2.5) | 9 (1.7) |
| Frequency omission | 820 (19.6) | 132 (24.6) |
| Both dosage and frequency omission | 520 (12.4) | 77 (14.3) |
| Missing Medications on the Physician Medication List (Drug Classes) | ADE Symptoms Related to a Medication Missing on the Physician Medication List (n) |
|---|---|
| Alimentary tract and metabolism (n = 21) | Dysglycemia (n = 11) |
| Hepato-gastrointestinal disorders (n = 6) | |
| Other (n = 4) | |
| Blood and blood-forming organs (n = 40) | Bleeding (n = 30) |
| Hematology and coagulation test abnormalities (n = 4) | |
| Other (n = 6) | |
| Cardiovascular system (n = 40) | Dyskalemia (n = 10) |
| Hypotension (n = 5) | |
| Dysnatremia (n = 4) | |
| Respiratory disorders (n = 4) | |
| Malaise (n = 4) | |
| Renal disorders (n = 4) | |
| Other (n = 9) | |
| Anti-infective drugs for systemic use (n = 30) | Hepato-gastrointestinal disorders (n = 8) |
| Hematology and coagulation test abnormalities (n = 6) | |
| Allergy (n = 5) | |
| Other (n = 11) | |
| Nervous system (n = 81) | Disturbed consciousness/fall (n = 33) |
| Hepato-gastrointestinal disorders (n = 16) | |
| Dysnatremia (n = 8) | |
| Seizure (n = 4) | |
| Other (n = 20) | |
| Genito-urinary system and sex hormones/Systemic hormonal preparations/Antineoplastic and immunomodulating agents/Muscular-skeletal system/Respiratory system/Other (n = 30) | Dyskalemia (n = 4) |
| Dysglycemia (n = 3) | |
| Hypotension (n = 3) | |
| Other (n = 20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goulas, C.; Lohan, L.; Laureau, M.; Perier, D.; Pinzani, V.; Faucanie, M.; Macioce, V.; Marin, G.; Giraud, I.; Villiet, M.; et al. Involvement of Pharmacists in the Emergency Department to Correct Errors in the Medication History and the Impact on Adverse Drug Event Detection. J. Clin. Med. 2023, 12, 376. https://doi.org/10.3390/jcm12010376
Goulas C, Lohan L, Laureau M, Perier D, Pinzani V, Faucanie M, Macioce V, Marin G, Giraud I, Villiet M, et al. Involvement of Pharmacists in the Emergency Department to Correct Errors in the Medication History and the Impact on Adverse Drug Event Detection. Journal of Clinical Medicine. 2023; 12(1):376. https://doi.org/10.3390/jcm12010376
Chicago/Turabian StyleGoulas, Clara, Laura Lohan, Marion Laureau, Damien Perier, Véronique Pinzani, Marie Faucanie, Valérie Macioce, Grégory Marin, Isabelle Giraud, Maxime Villiet, and et al. 2023. "Involvement of Pharmacists in the Emergency Department to Correct Errors in the Medication History and the Impact on Adverse Drug Event Detection" Journal of Clinical Medicine 12, no. 1: 376. https://doi.org/10.3390/jcm12010376