
Prosthesis Tailoring for Patients Undergoing Transcatheter Aortic Valve Implantation
 , ,
, ,
Abstract
:1. Introduction
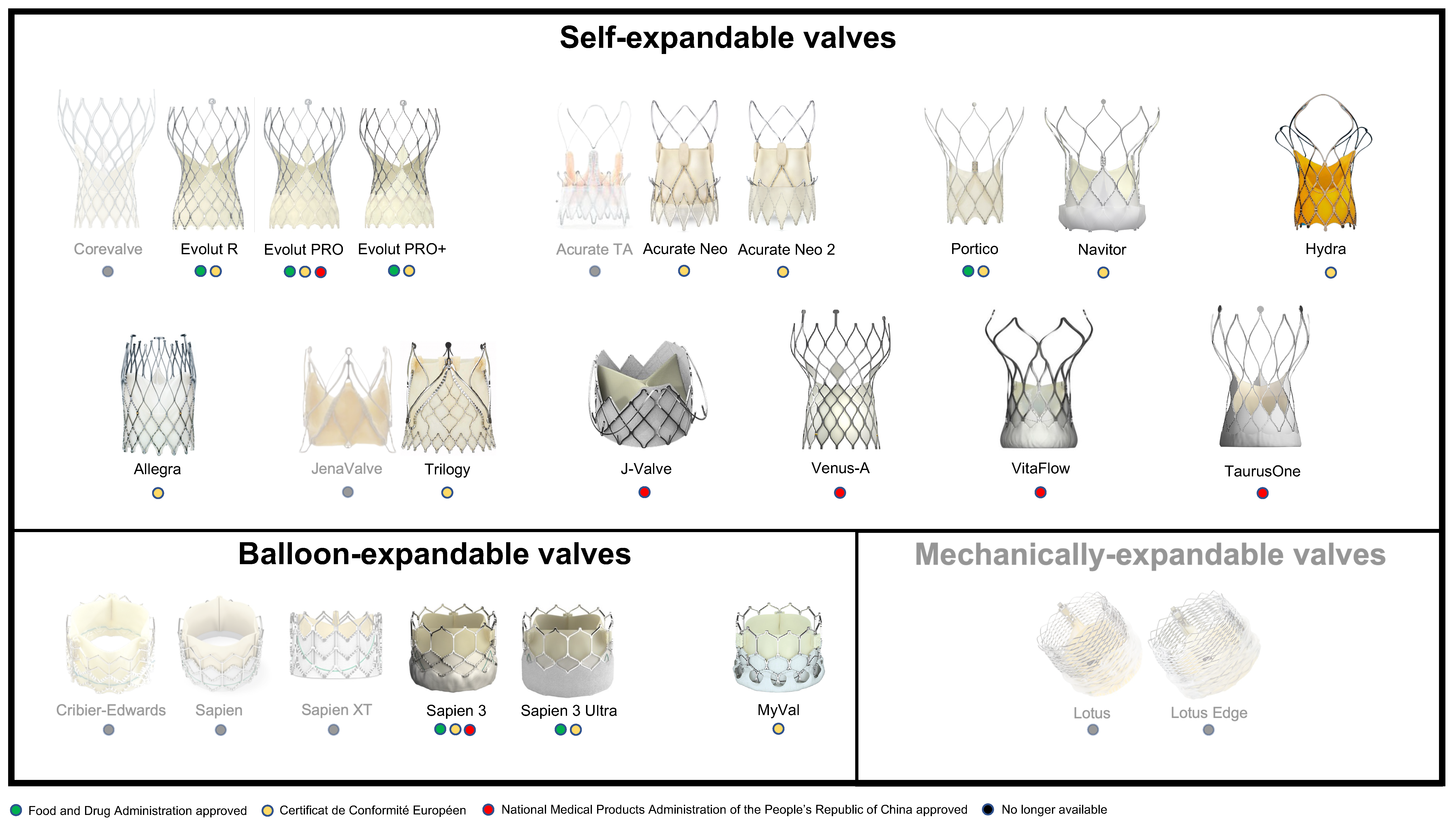
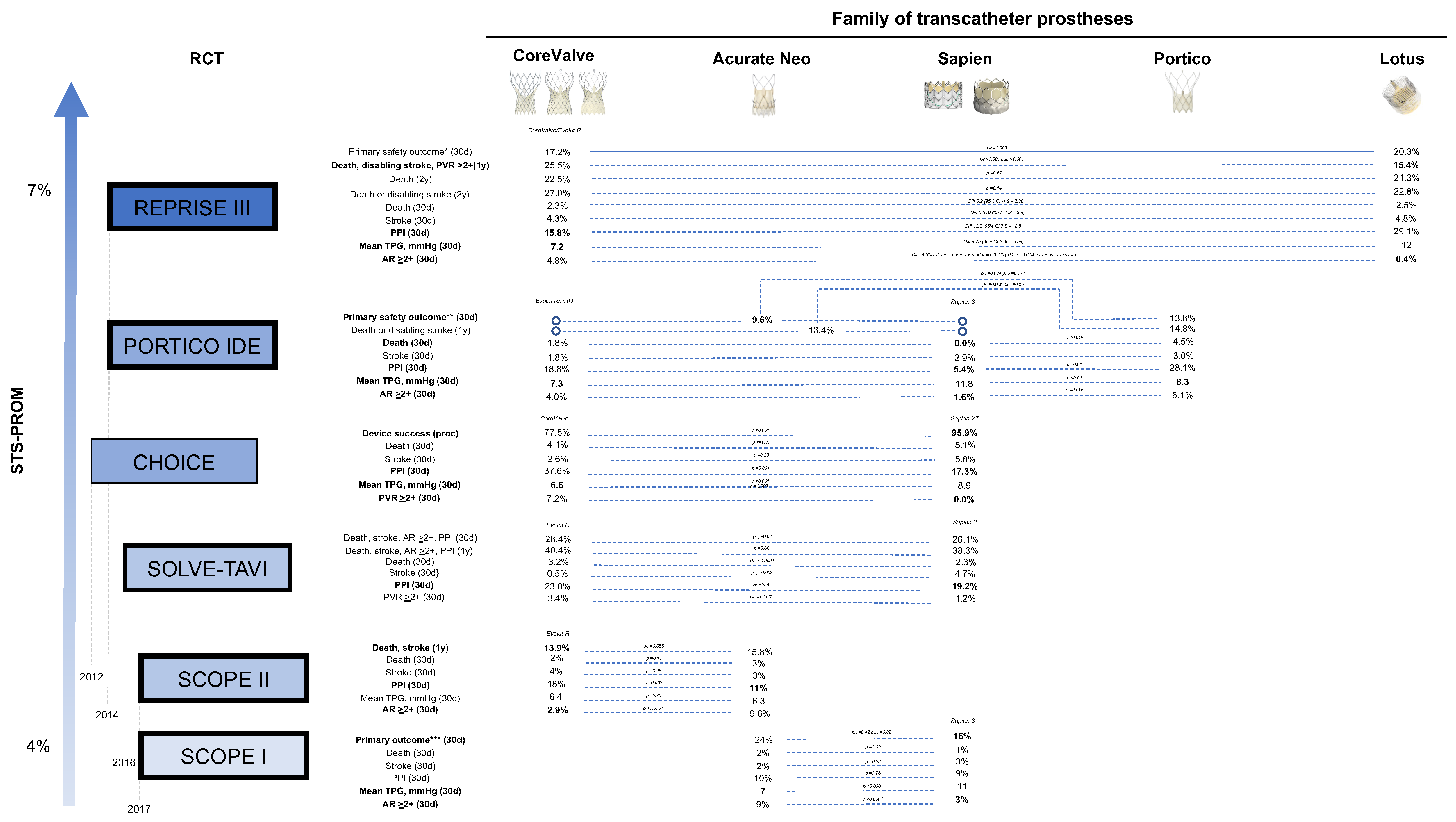
2. Prostheses
2.1. Self-Expandable Valves
2.1.1. Evolut PRO+ and CoreValve Family
2.1.2. Acurate Neo and Acurate Neo 2
2.1.3. Portico and Navitor
2.1.4. Others
2.2. Balloon-Expandable Valves
2.2.1. Sapien 3 Ultra and Sapien Family
2.2.2. MyVal
2.3. Mechanically Expandable Valves
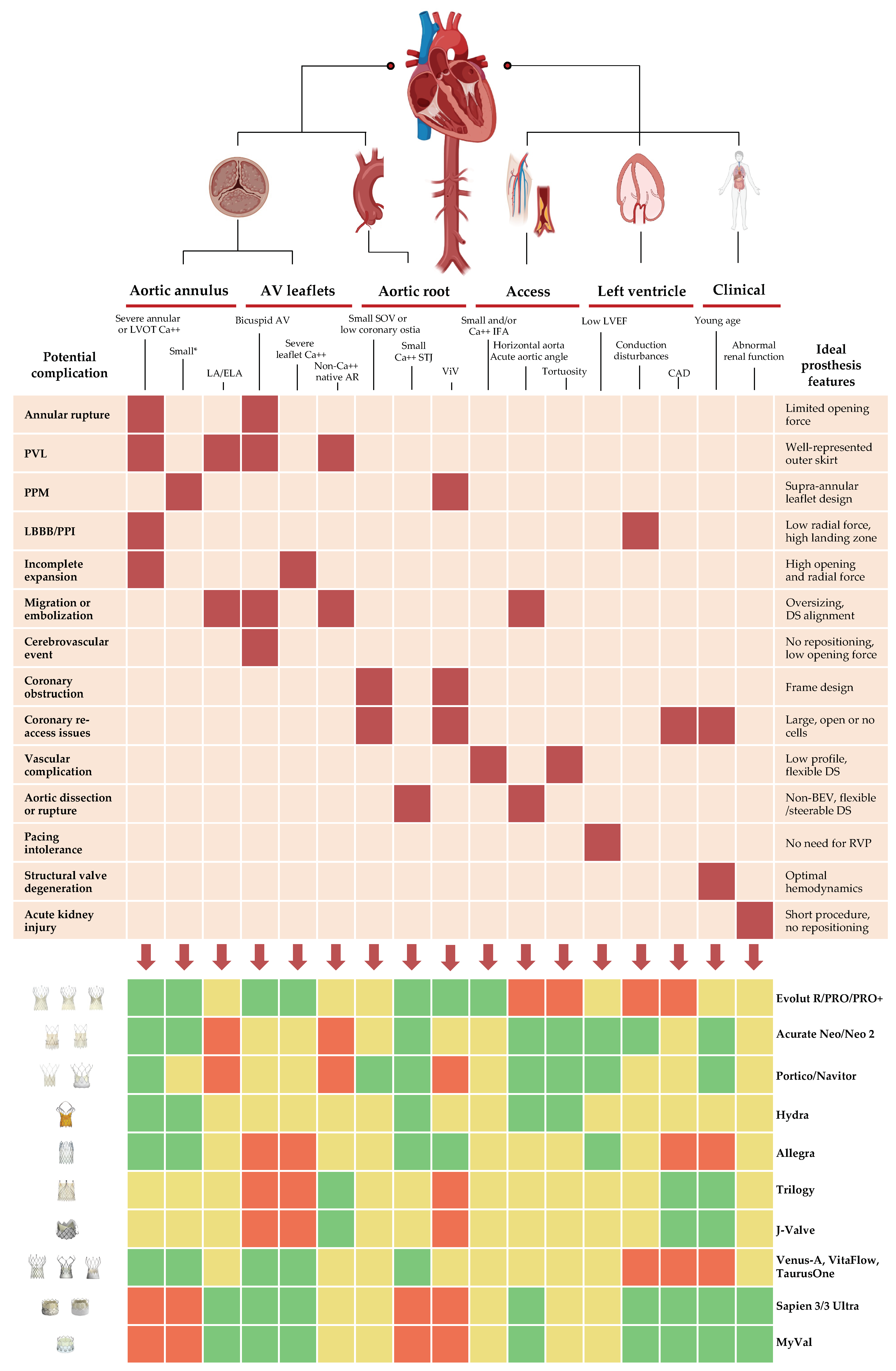
3. Factors to Consider for TAVI Prosthesis Tailoring
3.1. Aortic Annulus, Aortic Valve Leaflets and Aortic Root
3.1.1. Annular Size
3.1.2. Bicuspid Aortic Valve
3.1.3. Aortic Root Calcifications
3.1.4. Aortic Root Anatomy
3.1.5. Valve-in-Valve
3.1.6. Pure Native AR
3.2. Access and Delivery
3.2.1. Peripheral Vessel Calcification, Size and Tortuosity
3.2.2. Aortic Root Angulation
3.3. Left Ventricle
3.3.1. Pre-Existing Conduction Disturbances
3.3.2. Left Ventricular Ejection Fraction
3.3.3. Coronary Artery Disease
3.4. Clinical Factors
3.4.1. Age
3.4.2. Sex
3.4.3. Abnormal Baseline Renal Function
3.4.4. Body Size
3.5. Ease of Use
4. Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | aortic stenosis |
| AR | aortic regurgitation |
| BEV | balloon-expandable valve |
| EOA | effective orifice area |
| PPM | prosthesis-patient mismatch |
| MEV | mechanically expandable valve |
| PVL | paravalvular leak |
| RVP | rapid ventricular pacing |
| SAVR | surgical aortic valve replacement |
| SEV | self-expandable valve |
| TAVI | transcatheter aortic valve implantation |
| ViV | valve-in-valve |
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Eveborn, G.W.; Schirmer, H.; Heggelund, G.; Lunde, P.; Rasmussen, K. The evolving epidemiology of valvular aortic stenosis. The Tromsø Study. Heart 2013, 99, 396–400. [Google Scholar] [CrossRef] [Green Version]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef]
- Ross, J.; Braunwald, E. Aortic Stenosis. Circulation 1968, 38 (Suppl. 1), 61–67. [Google Scholar] [CrossRef]
- Cribier, A.; Eltchaninoff, H.; Bash, A.; Borenstein, N.; Tron, C.; Bauer, F.; Derumeaux, G.; Anselme, F.; Laborde, F.; Leon, M.B. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation 2002, 106, 3006–3008. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [Green Version]
- Kodali, S.K.; Williams, M.R.; Smith, C.R.; Svensson, L.G.; Webb, J.G.; Makkar, R.R.; Fontana, G.P.; Dewey, T.M.; Thourani, V.H.; Pichard, A.D.; et al. Two-Year Outcomes after Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2012, 366, 1686–1695. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makkar, R.R.; Fontana, G.P.; Jilaihawi, H.; Kapadia, S.; Pichard, A.D.; Douglas, P.S.; Thourani, V.H.; Babaliaros, V.C.; Webb, J.G.; Herrmann, H.C.; et al. Transcatheter Aortic-Valve Replacement for Inoperable Severe Aortic Stenosis. N. Engl. J. Med. 2012, 366, 1696–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef] [PubMed]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Søndergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Thyregod, H.G.H.; Steinbrüchel, D.A.; Ihlemann, N.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Transcatheter versus surgical aortic valve replacement in patients with severe aortic valve stenosis: 1-year results from the all-comers NOTION randomized clinical trial. J. Am. Coll. Cardiol. 2015, 65, 2184–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, M.-P.; Bartko, P.; Hofer, F.; Zbiral, M.; Burger, A.; Ghanim, B.; Kastner, J.; Lang, I.M.; Mascherbauer, J.; Hengstenberg, C.; et al. Evolution of outcome and complications in TAVR: A meta-analysis of observational and randomized studies. Sci. Rep. 2020, 10, 15568. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Guidelines for the management of valvular heart disease Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef]
- Claessen, B.E.; Tang, G.H.L.; Kini, A.S.; Sharma, S.K. Considerations for Optimal Device Selection in Transcatheter Aortic Valve Replacement: A Review. JAMA Cardiol. 2021, 6, 102–112. [Google Scholar] [CrossRef]
- Mahtta, D.; Elgendy, I.Y.; Bavry, A.A. From CoreValve to Evolut PRO: Reviewing the Journey of Self-Expanding Transcatheter Aortic Valves. Cardiol. Ther. 2017, 6, 183–192. [Google Scholar] [CrossRef]
- Leone, P.P.; Regazzoli, D.; Pagnesi, M.; Sanz-Sanchez, J.; Chiarito, M.; Cannata, F.; Van Mieghem, N.M.; Barbanti, M.; Tamburino, C.; Teles, R.; et al. Predictors and Clinical Impact of Prosthesis-Patient Mismatch After Self-Expandable TAVR in Small Annuli. JACC Cardiovasc. Interv. 2021, 14, 1218–1228. [Google Scholar] [CrossRef]
- Mangieri, A.; Montalto, C.; Pagnesi, M.; Lanzillo, G.; Demir, O.; Testa, L.; Colombo, A.; Latib, A. TAVI and Post Procedural Cardiac Conduction Abnormalities. Front. Cardiovasc. Med. 2018, 5, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbanti, M.; Costa, G.; Picci, A.; Criscione, E.; Reddavid, C.; Valvo, R.; Todaro, D.; Deste, W.; Condorelli, A.; Scalia, M.; et al. Coronary Cannulation after Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc. Interv. 2020, 13, 2542–2555. [Google Scholar] [CrossRef] [PubMed]
- Lanz, J.; Kim, W.-K.; Walther, T.; Burgdorf, C.; Möllmann, H.; Linke, A.; Redwood, S.; Thilo, C.; Hilker, M.; Joner, M.; et al. Safety and efficacy of a self-expanding versus a balloon-expandable bioprosthesis for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: A randomised non-inferiority trial. Lancet 2019, 394, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Tamburino, C.; Bleiziffer, S.; Thiele, H.; Scholtz, S.; Hildick-Smith, D.; Cunnington, M.; Wolf, A.; Barbanti, M.; Tchetché, D.; Garot, P.; et al. Comparison of Self-Expanding Bioprostheses for Transcatheter Aortic Valve Replacement in Patients with Symptomatic Severe Aortic Stenosis: The SCOPE 2 Randomized Clinical Trial. Circulation 2020, 142, 2431–2442. [Google Scholar] [CrossRef]
- Möllmann, H.; Holzhey, D.M.; Hilker, M.; Toggweiler, S.; Schäfer, U.; Treede, H.; Joner, M.; Søndergaard, L.; Christen, T.; Allocco, D.J.; et al. The ACURATE neo2 valve system for transcatheter aortic valve implantation: 30-day and 1-year outcomes. Clin. Res. Cardiol. 2021, 110, 1912–1920. [Google Scholar] [CrossRef]
- Makkar, R.R.; Cheng, W.; Waksman, R.; Satler, L.F.; Chakravarty, T.; Groh, M.; Abernethy, W.; Russo, M.J.; Heimansohn, D.; Hermiller, J.; et al. Self-expanding intra-annular versus commercially available transcatheter heart valves in high and extreme risk patients with severe aortic stenosis (PORTICO IDE): A randomised, controlled, non-inferiority trial. Lancet 2020, 396, 669–683. [Google Scholar] [CrossRef]
- Linke, A.; Holzhey, D.; Möllmann, H.; Manoharan, G.; Schäfer, U.; Frerker, C.; Worthley, S.G.; van Boven, A.; Redwood, S.; Kovac, J.; et al. Treatment of Aortic Stenosis With a Self-Expanding, Resheathable Transcatheter Valve. Circ. Cardiovasc. Interv. 2018, 11, e005206. [Google Scholar] [CrossRef]
- Fontana, G.P.; Bedogni, F.; Groh, M.; Smith, D.; Chehab, B.M.; Garrett, H.E.; Yong, G.; Worthley, S.; Manoharan, G.; Walton, A.; et al. Safety Profile of an Intra-Annular Self-Expanding Transcatheter Aortic Valve and Next-Generation Low-Profile Delivery System. JACC Cardiovasc. Interv. 2020, 13, 2467–2478. [Google Scholar] [CrossRef]
- Corcione, N.; Berni, A.; Ferraro, P.; Morello, A.; Cimmino, M.; Albanese, M.; Nestola, L.; Bardi, L.; Pepe, M.; Giordano, S.; et al. Transcatheter aortic valve implantation with the novel-generation Navitor device: Procedural and early outcomes. Catheter. Cardiovasc. Interv. 2022, 100, 114–119. [Google Scholar] [CrossRef]
- Bajoras, V.; Nuyens, P.; Vanhaverbeke, M.; Wang, X.; Bieliauskas, G.; De Backer, O.; Sondergaard, L. TAVR With the Novel Navitor Titan™ Transcatheter Heart Valve to Treat Aortic Stenosis Patients with Large Aortic Annuli. Cardiovasc. Revascularization Med. 2022, 40, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Aidietis, A.; Srimahachota, S.; Dabrowski, M.; Bilkis, V.; Buddhari, W.; Cheung, G.S.; Nair, R.K.; Mussayev, A.A.; Mattummal, S.; Chandra, P.; et al. 30-Day and 1-Year Outcomes with HYDRA Self-Expanding Transcatheter Aortic Valve: The Hydra CE Study. JACC Cardiovasc. Interv. 2022, 15, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Jilaihawi, H.; Wang, M.; Chen, M.; Wang, J.; Wang, W.; Feng, Y.; Liu, X.; Zhang, R.; Kong, X.; et al. Severe Symptomatic Bicuspid and Tricuspid Aortic Stenosis in China: Characteristics and Outcomes of Transcatheter Aortic Valve Replacement with the Venus-A Valve. Struct. Heart 2018, 2, 60–68. [Google Scholar] [CrossRef]
- Liao, Y.-B.; Zhao, Z.-G.; Wei, X.; Xu, Y.-N.; Zuo, Z.-L.; Li, Y.-J.; Zheng, M.-X.; Feng, Y.; Chen, M. Transcatheter aortic valve implantation with the self-expandable venus A-Valve and CoreValve devices: Preliminary Experiences in China. Catheter. Cardiovasc. Interv. 2017, 89, 528–533. [Google Scholar] [CrossRef]
- Zhou, D.; Pan, W.; Wang, J.; Wu, Y.; Chen, M.; Modine, T.; Mylotte, D.; Piazza, N.; Ge, J. VitaFlow™ transcatheter valve system in the treatment of severe aortic stenosis: One-year results of a multicenter study. Catheter. Cardiovasc. Interv. 2020, 95, 332–338. [Google Scholar] [CrossRef]
- Wang, M.; Song, G.; Chen, M.; Feng, Y.; Wang, J.; Liu, X.; Zhou, S.; Fang, Z.; Han, Y.; Xu, K.; et al. Twelve-month outcomes of the TaurusOne valve for transcatheter aortic valve implantation in patients with severe aortic stenosis. EuroIntervention 2022, 17, 1070–1076. [Google Scholar] [CrossRef]
- Schäfer, U.; Butter, C.; Landt, M.; Frerker, C.; Treede, H.; Schirmer, J.; Koban, C.; Allali, A.; Schmidt, T.; Charitos, E.; et al. One-year clinical outcomes of a novel transcatheter heart valve to treat degenerated surgical valves: The VIVALL study. EuroIntervention 2022, 17, 1077–1080. [Google Scholar] [CrossRef]
- Treede, H.; Mohr, F.-W.; Baldus, S.; Rastan, A.; Ensminger, S.; Arnold, M.; Kempfert, J.; Figulla, H.-R. Transapical transcatheter aortic valve implantation using the JenaValveTM system: Acute and 30-day results of the multicentre CE-mark study. Eur. J. Cardio-Thoracic Surg. 2012, 41, e131–e138. [Google Scholar] [CrossRef] [Green Version]
- Adam, M. First Clinical Results of the JenaValve TAVI System in Patients with Aortic Regurgitation; London Valves: London, UK, 2021. [Google Scholar]
- Hensey, M.; Murdoch, D.J.; Sathananthan, J.; Alenezi, A.; Sathananthan, G.; Moss, R.; Blanke, P.; Leipsic, J.; Wood, D.A.; Cheung, A.; et al. First-in-human experience of a new-generation transfemoral transcatheter aortic valve for the treatment of severe aortic regurgitation: The J-Valve transfemoral system. EuroIntervention 2019, 14, e1553–e1555. [Google Scholar] [CrossRef]
- Saia, F.; Gandolfo, C.; Palmerini, T.; Berti, S.; Doshi, S.N.; Laine, M.; Marcelli, C.; Piva, T.; Ribichini, F.; De Benedictis, M.; et al. In-hospital and thirty-day outcomes of the SAPIEN 3 Ultra balloon-expandable transcatheter aortic valve: The S3U registry. EuroIntervention 2020, 15, 1240–1247. [Google Scholar] [CrossRef]
- Sharma, S.K.; Rao, R.S.; Chandra, P.; Goel, P.K.; Bharadwaj, P.; Joseph, G.; Jose, J.; Mahajan, A.U.; Mehrotra, S.; Sengottovelu, G.; et al. First-in-human evaluation of a novel balloon-expandable transcatheter heart valve in patients with severe symptomatic native aortic stenosis: The MyVal-1 study. Eurointervention 2020, 16, 421–429. [Google Scholar] [CrossRef]
- Feldman, T.E.; Reardon, M.J.; Rajagopal, V.; Makkar, R.R.; Bajwa, T.K.; Kleiman, N.S.; Linke, A.; Kereiakes, D.J.; Waksman, R.; Thourani, V.H.; et al. Effect of Mechanically Expanded vs Self-Expanding Transcatheter Aortic Valve Replacement on Mortality and Major Adverse Clinical Events in High-Risk Patients With Aortic Stenosis: The REPRISE III Randomized Clinical Trial. JAMA 2018, 319, 27–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Belle, E.; Vincent, F.; Lab, C.; Auffret, V.; Debry, N.; Lefèvre, T.; Eltchaninoff, H.; Manigold, T.; Gilard, M.; Verhoye, J.-P.; et al. Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Replacement: A Propensity-Matched Comparison From the FRANCE-TAVI Registry. Circulation 2020, 141, 243–259. [Google Scholar] [CrossRef]
- Deharo, P.; Bisson, A.; Herbert, J.; Lacour, T.; Saint Etienne, C.; Grammatico-Guillon, L.; Porto, A.; Collart, F.; Bourguignon, T.; Cuisset, T.; et al. Impact of Sapien 3 Balloon-Expandable Versus Evolut R Self-Expandable Transcatheter Aortic Valve Implantation in Patients with Aortic Stenosis: Data from a Nationwide Analysis. Circulation 2020, 141, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Mehilli, J.; Frerker, C.; Neumann, F.-J.; Kurz, T.; Tölg, R.; Zachow, D.; Guerra, E.; Massberg, S.; Schäfer, U.; et al. Comparison of balloon-expandable vs. self-expandable valves in patients undergoing transcatheter aortic valve replacement: The CHOICE randomized clinical trial. JAMA 2014, 311, 1503–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feistritzer, H.-J.; Kurz, T.; Stachel, G.; Hartung, P.; Lurz, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; Vigelius-Rauch, U.; et al. Impact of Anesthesia Strategy and Valve Type on Clinical Outcomes After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2021, 77, 2204–2215. [Google Scholar] [CrossRef] [PubMed]
- Reardon, M.J.; Feldman, T.E.; Meduri, C.U.; Makkar, R.R.; O’Hair, D.; Linke, A.; Kereiakes, D.J.; Waksman, R.; Babliaros, V.; Stoler, R.C.; et al. Two-Year Outcomes after Transcatheter Aortic Valve Replacement with Mechanical vs Self-expanding Valves: The REPRISE III Randomized Clinical Trial. JAMA Cardiol. 2019, 4, 223–229. [Google Scholar] [CrossRef]
- Søndergaard, L.; Rodés-Cabau, J.; Linke, A.H.-P.; Fichtlscherer, S.; Schäfer, U.; Kuck, K.-H.; Kempfert, J.; Arzamendi, D.; Bedogni, F.; Asch, F.M.; et al. Transcatheter Aortic Valve Replacement with a Repositionable Self-Expanding Prosthesis The PORTICO-I Trial 1-Year Outcomes. J. Am. Coll. Cardiol. 2018, 72, 2859–2867. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.-H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Thourani, V.H.; Kodali, S.; Makkar, R.R.; Herrmann, H.C.; Williams, M.; Babaliaros, V.; Smalling, R.; Lim, S.; Malaisrie, S.C.; Kapadia, S.; et al. Transcatheter aortic valve replacement versus surgical valve replacement in intermediate-risk patients: A propensity score analysis. Lancet 2016, 387, 2218–2225. [Google Scholar] [CrossRef]
- Waksman, R.; Rogers, T.; Torguson, R.; Gordon, P.; Ehsan, A.; Wilson, S.R.; Goncalves, J.; Levitt, R.; Hahn, C.; Parikh, P.; et al. Transcatheter Aortic Valve Replacement in Low-Risk Patients With Symptomatic Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2018, 72, 2095–2105. [Google Scholar] [CrossRef] [PubMed]
- Van Mieghem, N.M.; Wöhrle, J.; Hildick-Smith, D.; Bleiziffer, S.; Blackman, D.J.; Abdel-Wahab, M.; Gerckens, U.; Linke, A.; Ince, H.; Wenaweser, P.; et al. Use of a Repositionable and Fully Retrievable Aortic Valve in Routine Clinical Practice: The RESPOND Study and RESPOND Extension Cohort. JACC Cardiovasc. Interv. 2019, 12, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Falk, V.; Wöhrle, J.; Hildick-Smith, D.; Bleiziffer, S.; Blackman, D.J.; Abdel-Wahab, M.; Gerckens, U.; Linke, A.; Ince, H.; Wenaweser, P.; et al. Safety and efficacy of a repositionable and fully retrievable aortic valve used in routine clinical practice: The RESPOND Study. Eur. Heart J. 2017, 38, 3359–3366. [Google Scholar] [CrossRef] [Green Version]
- Waksman, R.; Torguson, R.; Medranda, G.A.; Shea, C.; Zhang, C.; Gordon, P.; Ehsan, A.; Wilson, S.R.; Levitt, R.; Hahn, C.; et al. Transcatheter aortic valve replacement in low-risk patients: 2-year results from the LRT trial. Am. Heart J. 2021, 237, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Mack, M.J.; Hahn, R.T.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Alu, M.C.; Madhavan, M.V.; Chau, K.H.; Russo, M.; et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J. Am. Coll. Cardiol. 2021, 77, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Forrest, J.K.; Deeb, G.M.; Yakubov, S.J.; Rovin, J.D.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Sorajja, P.; Heiser, J.C.; et al. 2-Year Outcomes After Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients. J. Am. Coll. Cardiol. 2022, 79, 882–896. [Google Scholar] [CrossRef]
- Thyregod, H.G.H.; Ihlemann, N.; Jørgensen, T.H.; Nissen, H.; Kjeldsen, B.J.; Petursson, P.; Chang, Y.; Franzen, O.W.; Engstrøm, T.; Clemmensen, P.; et al. Five-Year Clinical and Echocardiographic Outcomes From the NOTION Randomized Clinical Trial in Patients at Lower Surgical Risk. Circulation 2019, 139, 2714–2723. [Google Scholar] [CrossRef]
- Pagnesi, M.; Kim, W.-K.; Conradi, L.; Barbanti, M.; Stefanini, G.G.; Zeus, T.; Pilgrim, T.; Schofer, J.; Zweiker, D.; Testa, L.; et al. Transcatheter Aortic Valve Replacement with Next-Generation Self-Expanding Devices: A Multicenter, Retrospective, Propensity-Matched Comparison of Evolut PRO Versus Acurate neo Transcatheter Heart Valves. JACC Cardiovasc. Interv. 2019, 12, 433–443. [Google Scholar] [CrossRef]
- Husser, O.; Kim, W.-K.; Pellegrini, C.; Holzamer, A.; Walther, T.; Mayr, P.N.; Joner, M.; Kasel, A.M.; Trenkwalder, T.; Michel, J.; et al. Multicenter Comparison of Novel Self-Expanding Versus Balloon-Expandable Transcatheter Heart Valves. JACC Cardiovasc. Interv. 2017, 10, 2078–2087. [Google Scholar] [CrossRef]
- Kim, W.-K.; Hengstenberg, C.; Hilker, M.; Kerber, S.; Schäfer, U.; Rudolph, T.; Linke, A.; Franz, N.; Kuntze, T.; Nef, H.; et al. The SAVI-TF Registry: 1-Year Outcomes of the European Post-Market Registry Using the ACURATE neo Transcatheter Heart Valve Under Real-World Conditions in 1000 Patients. JACC Cardiovasc. Interv. 2018, 11, 1368–1374. [Google Scholar] [CrossRef]
- Maisano, F.; Worthley, S.; Rodés-Cabau, J.; Linke, A.H.-P.; Fichtlscherer, S.; Schäfer, U.; Makkar, R.R.; Fontana, G.; Asch, F.M.; Søndergaard, L. Early commercial experience from transcatheter aortic valve implantation using the Portico™ bioprosthetic valve: 30-day outcomes in the multicentre PORTICO-1 study. EuroIntervention 2018, 14, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Freitas-Ferraz, A.B.; Tirado, G.; Dagenais, F.; Ruel, M.; Al-Atassi, T.; Dumont, E.; Mohammadi, S.; Bernier, M.; Pibarot, P.; Rodés-Cabau, J. Aortic Stenosis and Small Aortic Annulus: Clinical Challenges and Current Therapeutic Alternatives. Circulation 2019, 139, 2685–2702. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, H.C.; Daneshvar, S.A.; Fonarow, G.C.; Stebbins, A.; Vemulapalli, S.; Desai, N.D.; Malenka, D.J.; Thourani, V.H.; Rymer, J.; Kosinski, A.S. Prosthesis–Patient Mismatch in Patients Undergoing Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. J. Am. Coll. Cardiol. 2018, 72, 2701–2711. [Google Scholar] [CrossRef] [PubMed]
- Regazzoli, D.; Chiarito, M.; Cannata, F.; Pagnesi, M.; Miura, M.; Ziviello, F.; Picci, A.; Reifart, J.; De Marco, F.; Bedogni, F.; et al. Transcatheter Self-Expandable Valve Implantation for Aortic Stenosis in Small Aortic Annuli: The TAVI-SMALL Registry. JACC Cardiovasc. Interv. 2020, 13, 196–206. [Google Scholar] [CrossRef]
- Okuno, T.; Tomii, D.; Heg, D.; Lanz, J.; Praz, F.; Stortecky, S.; Reineke, D.; Windecker, S.; Pilgrim, T. Five-year outcomes of mild paravalvular regurgitation after transcatheter aortic valve implantation. Eurointervention 2022, 18, 33–42. [Google Scholar] [CrossRef]
- Sengupta, A.; Zaid, S.; Kamioka, N.; Terre, J.; Miyasaka, M.; Hirji, S.A.; Hensey, M.; Geloo, N.; Petrossian, G.; Robinson, N.; et al. Mid-Term Outcomes of Transcatheter Aortic Valve Replacement in Extremely Large Annuli WITH Edwards SAPIEN 3 Valve. JACC Cardiovasc. Interv. 2020, 13, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Armijo, G.; Tang, G.H.; Kooistra, N.; Ferreira-Neto, A.N.; Toggweiler, S.; Amat-Santos, I.J.; Keller, L.S.; Urena, M.; Ahmad, H.; Soto, J.T.; et al. Third-Generation Balloon and Self-Expandable Valves for Aortic Stenosis in Large and Extra-Large Aortic Annuli from the TAVR-LARGE Registry. Circ. Cardiovasc. Interv. 2020, 13, e009047. [Google Scholar] [CrossRef] [PubMed]
- Deeb, G.M.; Reardon, M.J.; Ramlawi, B.; Yakubov, S.J.; Chetcuti, S.J.; Kleiman, N.S.; Mangi, A.A.; Zahr, F.; Song, H.K.; Gada, H.; et al. Propensity-Matched 1-Year Outcomes Following Transcatheter Aortic Valve Replacement in Low-Risk Bicuspid and Tricuspid Patients. JACC Cardiovasc. Interv. 2022, 15, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.R.; Jilaihawi, H.; Makkar, R.; O’Neill, W.W.; Guyton, R.; Malaisrie, S.C.; Brown, D.L.; Blanke, P.; Leipsic, J.A.; Pibarot, P.; et al. The PARTNER 3 Bicuspid Registry for Transcatheter Aortic Valve Replacement in Low-Surgical-Risk Patients. JACC Cardiovasc. Interv. 2022, 15, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Vincent, F.; Ternacle, J.; Denimal, T.; Shen, M.; Redfors, B.; Delhaye, C.; Simonato, M.; Debry, N.; Verdier, B.; Shahim, B.; et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation 2021, 143, 1043–1061. [Google Scholar] [CrossRef]
- Makkar, R.R.; Yoon, S.-H.; Chakravarty, T.; Kapadia, S.R.; Krishnaswamy, A.; Shah, P.B.; Kaneko, T.; Skipper, E.R.; Rinaldi, M.; Babaliaros, V.; et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke Among Patients at Low Surgical Risk. JAMA 2021, 326, 1034–1044. [Google Scholar] [CrossRef] [PubMed]
- Montalto, C.; Sticchi, A.; Crimi, G.; Laricchia, A.; Khokhar, A.A.; Giannini, F.; Reimers, B.; Colombo, A.; Latib, A.; Waksman, R.; et al. Outcomes After Transcatheter Aortic Valve Replacement in Bicuspid Versus Tricuspid Anatomy: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Interv. 2021, 14, 2144–2155. [Google Scholar] [CrossRef] [PubMed]
- Waksman, R.; Craig, P.E.; Torguson, R.; Asch, F.M.; Weissman, G.; Ruiz, D.; Gordon, P.; Ehsan, A.; Parikh, P.; Bilfinger, T.; et al. Transcatheter Aortic Valve Replacement in Low-Risk Patients With Symptomatic Severe Bicuspid Aortic Valve Stenosis. JACC Cardiovasc. Interv. 2020, 13, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Lefèvre, T.; Ahn, J.-M.; Perlman, G.Y.; Dvir, D.; Latib, A.; Barbanti, M.; Deuschl, F.; De Backer, O.; Blanke, P.; et al. Transcatheter Aortic Valve Replacement With Early- and New-Generation Devices in Bicuspid Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2016, 68, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, A.; Tchetchè, D.; Kim, W.-K.; Pagnesi, M.; Sinning, J.-M.; Landes, U.; Kornowski, R.; De Backer, O.; Nickenig, G.; Ielasi, A.; et al. Balloon Versus Self-Expandable Valve for the Treatment of Bicuspid Aortic Valve Stenosis: Insights From the BEAT International Collaborative Registrys. Circ. Cardiovasc. Interv. 2020, 13, e008714. [Google Scholar] [CrossRef]
- Fonseca, P.; Figueiredo, B.; Almeida, C.; Almeida, J.; Bettencourt, N.; Sampaio, F.; Ferreira, N.; Gonçalves, H.; Braga, P.; Ribeiro, V.G. Aortic Valve Calcium Volume Predicts Paravalvular Regurgitation and the Need for Balloon Post-Dilatation After Transcatheter Aortic Valve Implantation. J. Interv. Cardiol. 2016, 29, 117–123. [Google Scholar] [CrossRef]
- Hansson, N.C.; Leipsic, J.; Pugliese, F.; Andersen, H.R.; Rossi, A.; Simonato, M.; Jensen, K.T.; Christiansen, E.H.; Terkelsen, C.J.; Blanke, P.; et al. Aortic valve and left ventricular outflow tract calcium volume and distribution in transcatheter aortic valve replacement: Influence on the risk of significant paravalvular regurgitation. J. Cardiovasc. Comput. Tomogr. 2018, 12, 290–297. [Google Scholar] [CrossRef]
- Barbanti, M.; Petronio, A.S.; Capodanno, D.; Ettori, F.; Colombo, A.; Bedogni, F.; De Marco, F.; De Carlo, M.; Fiorina, C.; Latib, A.; et al. Impact of Balloon Post-Dilation on Clinical Outcomes after Transcatheter Aortic Valve Replacement with the Self-Expanding CoreValve Prosthesis. JACC Cardiovasc. Interv. 2014, 7, 1014–1021. [Google Scholar] [CrossRef]
- Pagnesi, M.; Jabbour, R.J.; Latib, A.; Kawamoto, H.; Tanaka, A.; Regazzoli, D.; Mangieri, A.; Montalto, C.; Ancona, M.B.; Giannini, F.; et al. Usefulness of Predilation before Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 118, 107–112. [Google Scholar] [CrossRef]
- Biasco, L.; Cerrato, E.; Tersalvi, G.; Pedrazzini, G.; Wilkins, B.; Faletra, F.; Ferrari, E.; Demertzis, S.; Senatore, G.; Di Leo, A.; et al. WorldwIde SurvEy on Clinical and Anatomical Factors Driving the Choice of Transcatheter Aortic Valve pRostheses. Front. Cardiovasc. Med. 2020, 7, 38. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, H.B.; Webb, J.G.; Makkar, R.R.; Cohen, M.G.; Kapadia, S.R.; Kodali, S.; Tamburino, C.; Barbanti, M.; Chakravarty, T.; Jilaihawi, H.; et al. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: Insights from a large multicenter registry. J. Am. Coll. Cardiol. 2013, 62, 1552–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabbour, R.; Tanaka, A.; Finkelstein, A.; Mack, M.; Tamburino, C.; Van Mieghem, N.; De Backer, O.; Testa, L.; Gatto, P.; Purita, P.; et al. Delayed Coronary Obstruction After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2018, 71, 1513–1524. [Google Scholar] [CrossRef]
- Sá, M.P.; Ramlawi, B.; Sicouri, S.; Torregrossa, G.; Al Abri, Q.; Kempfert, J.; Kofler, M.; Falk, V.; Unbehaun, A.; Van Praet, K.M.; et al. Lifetime management of aortic valve disease: Aligning surgical and transcatheter armamentarium to set the tone for the present and the future. J. Card. Surg. 2022, 37, 205–213. [Google Scholar] [CrossRef]
- Raschpichler, M.C.; Woitek, F.; Chakravarty, T.; Flint, N.; Yoon, S.; Mangner, N.; Patel, C.G.; Singh, C.; Kashif, M.; Kiefer, P.; et al. Valve-in-Valve for Degenerated Transcatheter Aortic Valve Replacement Versus Valve-in-Valve for Degenerated Surgical Aortic Bioprostheses: A 3-Center Comparison of Hemodynamic and 1-Year Outcome. J. Am. Heart Assoc. 2020, 9, e013973. [Google Scholar] [CrossRef]
- Brinkmann, C.; Abdel-Wahab, M.; Bedogni, F.; Bhadra, O.D.; Charbonnier, G.; Conradi, L.; Hildick-Smith, D.; Kargoli, F.; Latib, A.; Van Mieghem, N.M.; et al. Outcomes of valve-in-valve transcatheter aortic valve implantation with and without bioprosthetic valve fracture. EuroIntervention 2021, 17, 848–855. [Google Scholar] [CrossRef]
- Hamilton, G.W.; Koshy, A.N.; Fulcher, J.; Tang, G.H.; Bapat, V.; Murphy, A.; Horrigan, M.; Farouque, O.; Yudi, M.B. Meta-analysis Comparing Valve-In-Valve Transcatheter Aortic Valve Implantation With Self-Expanding Versus Balloon-Expandable Valves. Am. J. Cardiol. 2020, 125, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, T.; Oakley, L.; Sekhon, N.; Komatsu, I.; Flint, N.; Kaewkes, D.; Yoon, S.-H.; Raschpichler, M.; Patel, V.; Tiwana, R.; et al. Risk of Coronary Obstruction Due to Sinus Sequestration in Redo Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 2617–2627. [Google Scholar] [CrossRef]
- Khan, J.M.; Greenbaum, A.B.; Babaliaros, V.C.; Rogers, T.; Eng, M.H.; Paone, G.; Leshnower, B.G.; Reisman, M.; Satler, L.; Waksman, R.; et al. The BASILICA Trial: Prospective Multicenter Investigation of Intentional Leaflet Laceration to Prevent TAVR Coronary Obstruction. JACC Cardiovasc. Interv. 2019, 12, 1240–1252. [Google Scholar] [CrossRef] [PubMed]
- Edelman, J.J.; Khan, J.M.; Rogers, T.; Shults, C.; Satler, L.F.; Ben-Dor, I.I.; Waksman, R.; Thourani, V.H. Valve-in-Valve TAVR: State-of-the-Art Review. Innovations 2019, 14, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.-H.; Schmidt, T.; Bleiziffer, S.; Schofer, N.; Fiorina, C.; Munoz-Garcia, A.J.; Yzeiraj, E.; Amat-Santos, I.J.; Tchetche, D.; Jung, C.; et al. Transcatheter Aortic Valve Replacement in Pure Native Aortic Valve Regurgitation. J. Am. Coll. Cardiol. 2017, 70, 2752–2763. [Google Scholar] [CrossRef]
- Sawaya, F.J.; Deutsch, M.-A.; Seiffert, M.; Yoon, S.-H.; Codner, P.; Wickramarachchi, U.; Latib, A.; Petronio, A.S.; Rodés-Cabau, J.; Taramasso, M.; et al. Safety and Efficacy of Transcatheter Aortic Valve Replacement in the Treatment of Pure Aortic Regurgitation in Native Valves and Failing Surgical Bioprostheses: Results from an International Registry Study. JACC Cardiovasc. Interv. 2017, 10, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Lefèvre, T.; Chevalier, B.; Hovasse, T.; Romano, M.; Garot, P.; Mylotte, D.; Uribe, J.; Farge, A.; Donzeau-Gouge, P.; et al. Transfemoral Aortic Valve Implantation: New Criteria to Predict Vascular Complications. JACC Cardiovasc. Interv. 2011, 4, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gedela, M.; Khera, S.; Tadros, R.O.; Krishnamoorthy, P.; Hooda, A.; Moreno, P.; Dangas, G.D.; Sharma, S.K.; Kini, A.S.; Tang, G.H. Balloon Dilatation of Expandable Sheath to Facilitate Transfemoral SAPIEN 3 Transcatheter Aortic Valve Replacement in Severely Calcified Vasculature. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100009. [Google Scholar] [CrossRef]
- Taramasso, M.; Denegri, A.; Kuwata, S.; Rickli, H.; Haager, P.K.; Sütsch, G.; Biefer, H.R.C.; Kottwitz, J.; Nietlispach, F.; Maisano, F. Feasibility and safety of transfemoral sheathless portico aortic valve implantation: Preliminary results in a single center experience. Catheter. Cardiovasc. Interv. 2018, 91, 533–539. [Google Scholar] [CrossRef]
- Di Mario, C.; Goodwin, M.; Ristalli, F.; Ravani, M.; Meucci, F.; Stolcova, M.; Sardella, G.; Salvi, N.; Bedogni, F.; Berti, S.; et al. A Prospective Registry of Intravascular Lithotripsy-Enabled Vascular Access for Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 502–504. [Google Scholar] [CrossRef]
- Abramowitz, Y.; Maeno, Y.; Chakravarty, T.; Kazuno, Y.; Takahashi, N.; Kawamori, H.; Mangat, G.; Cheng, W.; Jilaihawi, H.; Makkar, R.R. Aortic Angulation Attenuates Procedural Success Following Self-Expandable But Not Balloon-Expandable TAVR. JACC Cardiovasc. Imaging 2016, 9, 964–972. [Google Scholar] [CrossRef]
- Gallo, F.; Gallone, G.; Kim, W.-K.; Reifart, J.; Veulemans, V.; Zeus, T.; Toggweiler, S.; De Backer, O.; Søndergaard, L.; Mangieri, A.; et al. Horizontal Aorta in Transcatheter Self-Expanding Valves: Insights from the HORSE International Multicentre Registry. Circ. Cardiovasc. Interv. 2021, 14, 958–966. [Google Scholar] [CrossRef]
- Renker, M.; Kim, W.-K. Choice of transcatheter heart valve: Should we select the device according to each patient’s characteristics or should it be “one valve fits all”? Ann. Transl. Med. 2020, 8, 961. [Google Scholar] [CrossRef]
- Houthuizen, P.; Van Garsse, L.A.F.M.; Poels, T.T.; De Jaegere, P.; Van Der Boon, R.M.; Swinkels, B.M.; Berg, J.M.T.; Van Der Kley, F.; Schalij, M.J.; Baan, J.; et al. Left Bundle-Branch Block Induced by Transcatheter Aortic Valve Implantation Increases Risk of Death. Circulation 2012, 126, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Bruno, F.; D’Ascenzo, F.; Vaira, M.P.; Elia, E.; Omedè, P.; Kodali, S.; Barbanti, M.; Rodès-Cabau, J.; Husser, O.; Sossalla, S.; et al. Predictors of pacemaker implantation after transcatheter aortic valve implantation according to kind of prosthesis and risk profile: A systematic review and contemporary meta-analysis. Eur. Hear. J. Qual. Care Clin. Outcomes 2021, 7, 143–153. [Google Scholar] [CrossRef]
- Pascual, I.; Hernández-Vaquero, D.; Alperi, A.; Almendarez, M.; Avanzas, P.; Kalavrouziotis, D.; Lorca, R.; Mesnier, J.; Arboine, L.; Mohammadi, S.; et al. Permanent Pacemaker Reduction Using Cusp-Overlapping Projection in TAVR: A Propensity Score Analysis. JACC Cardiovasc. Interv. 2022, 15, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, H.B.; Lerakis, S.; Gilard, M.; Cavalcante, J.L.; Makkar, R.; Herrmann, H.C.; Windecker, S.; Enriquez-Sarano, M.; Cheema, A.N.; Nombela-Franco, L.; et al. Transcatheter Aortic Valve Replacement in Patients With Low-Flow, Low-Gradient Aortic Stenosis: The TOPAS-TAVI Registry. J. Am. Coll. Cardiol. 2018, 71, 1297–1308. [Google Scholar] [CrossRef]
- Lauten, A.; Zahn, R.; Horack, M.; Sievert, H.; Linke, A.; Ferrari, M.; Harnath, A.; Grube, E.; Gerckens, U.; Kuck, K.-H.; et al. Transcatheter Aortic Valve Implantation in Patients with Low-Flow, Low-Gradient Aortic Stenosis. JACC Cardiovasc. Interv. 2012, 5, 552–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fefer, P.; Bogdan, A.; Grossman, Y.; Berkovitch, A.; Brodov, Y.; Kuperstein, R.; Segev, A.; Guetta, V.; Barbash, I.M. Impact of Rapid Ventricular Pacing on Outcome After Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2018, 7, e009038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yudi, M.B.; Sharma, S.K.; Tang, G.H.; Kini, A. Coronary Angiography and Percutaneous Coronary Intervention After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2018, 71, 1360–1378. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Cerrato, E.; Pivato, C.A.; Joner, M.; Testa, L.; Rheude, T.; Pilgrim, T.; Pavani, M.; Brouwer, J.; Otero, D.L.; et al. Unplanned Percutaneous Coronary Revascularization After TAVR: A Multicenter International Registry. JACC Cardiovasc. Interv. 2021, 14, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Fovino, L.N.; Scotti, A.; Massussi, M.; Cardaioli, F.; Rodinò, G.; Benedetti, A.; Boiago, M.; Matsuda, Y.; Continisio, S.; et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment: The ALIGN-ACCESS Study. Circ. Cardiovasc. Interv. 2022, 15, e011045. [Google Scholar] [CrossRef] [PubMed]
- Fovino, L.N.; Scotti, A.; Massussi, M.; Cardaioli, F.; Rodinò, G.; Matsuda, Y.; Pavei, A.; Masiero, G.; Napodano, M.; Fraccaro, C.; et al. Coronary Angiography after Transcatheter Aortic Valve Replacement (TAVR) to Evaluate the Risk of Coronary Access Impairment after TAVR-in-TAVR. J. Am. Heart Assoc. 2020, 9, e016446. [Google Scholar] [CrossRef]
- Jørgensen, T.H.; Thyregod, H.G.H.; Ihlemann, N.; Nissen, H.; Petursson, P.; Kjeldsen, B.J.; Steinbrüchel, D.A.; Olsen, P.S.; Søndergaard, L. Eight-year outcomes for patients with aortic valve stenosis at low surgical risk randomized to transcatheter vs. surgical aortic valve replacement. Eur. Heart J. 2021, 42, 2912–2919. [Google Scholar] [CrossRef]
- Makkar, R.R.; Fontana, G.; Jilaihawi, H.; Chakravarty, T.; Kofoed, K.F.; De Backer, O.; Asch, F.M.; Ruiz, C.E.; Olsen, N.T.; Trento, A.; et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N. Engl. J. Med. 2015, 373, 2015–2024. [Google Scholar] [CrossRef]
- Bogyi, M.; Schernthaner, R.E.; Loewe, C.; Gager, G.M.; Dizdarevic, A.M.; Kronberger, C.; Postula, M.; Legutko, J.; Velagapudi, P.; Hengstenberg, C.; et al. Subclinical Leaflet Thrombosis After Transcatheter Aortic Valve Replacement: A Meta-Analysis. JACC Cardiovasc. Interv. 2021, 14, 2643–2656. [Google Scholar] [CrossRef]
- Amat-Santos, I.J.; Messika-Zeitoun, D.; Eltchaninoff, H.; Kapadia, S.R.; Lerakis, S.; Cheema, A.N.; Gutierrez, E.; Muñoz-Garcia, A.; Pan, M.; Webb, J.G.; et al. Infective endocarditis after transcatheter aortic valve implantation results from a large multicenter registry. Circulation 2015, 131, 1566–1574. [Google Scholar] [CrossRef] [Green Version]
- Costa, G.; Saia, F.; Pilgrim, T.; Abdel-Wahab, M.; Garot, P.; Valvo, R.; Gandolfo, C.; Branca, L.; Latib, A.; Santos, I.A.; et al. Transcatheter Aortic Valve Replacement with the Latest-Iteration Self-Expanding or Balloon-Expandable Valves: The Multicenter OPERA-TAVI Registry. JACC Cardiovasc. Interv. 2022, 15, 2398–2407. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, S.R.; Krishnaswamy, A. Valve Choice in TAVR: A Complex Equation to Solve. J. Am. Coll. Cardiol. 2021, 77, 2216–2218. [Google Scholar] [CrossRef] [PubMed]
- Attinger-Toller, A.; Ferrari, E.; Tueller, D.; Templin, C.; Muller, O.; Nietlispach, F.; Toggweiler, S.; Noble, S.; Roffi, M.; Jeger, R.; et al. Age-Related Outcomes After Transcatheter Aortic Valve Replacement: Insights From the SwissTAVI Registry. JACC Cardiovasc. Interv. 2021, 14, 952–960. [Google Scholar] [CrossRef] [PubMed]
- DesJardin, J.T.; Chikwe, J.; Hahn, R.T.; Hung, J.W.; Delling, F.N. Sex Differences and Similarities in Valvular Heart Disease. Circ. Res. 2022, 130, 455–473. [Google Scholar] [CrossRef] [PubMed]
- Leone, P.P.; Fazzari, F.; Cannata, F.; Sanz-Sanchez, J.; Mangieri, A.; Monti, L.; Cozzi, O.; Stefanini, G.G.; Bragato, R.; Colombo, A.; et al. Clinical and Technical Challenges of Prosthesis–Patient Mismatch after Transcatheter Aortic Valve Implantation. Front. Cardiovasc. Med. 2021, 8, 670457. [Google Scholar] [CrossRef]
- Cubeddu, R.J.; Asher, C.R.; Lowry, A.M.; Blackstone, E.H.; Kapadia, S.R.; Alu, M.C.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Herrmann, H.C.; et al. Impact of Transcatheter Aortic Valve Replacement on Severity of Chronic Kidney Disease. J. Am. Coll. Cardiol. 2020, 76, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Julien, H.M.; Stebbins, A.; Vemulapalli, S.; Nathan, A.S.; Eneanya, N.D.; Groeneveld, P.; Fiorilli, P.N.; Herrmann, H.C.; Szeto, W.Y.; Desai, N.D.; et al. Incidence, Predictors, and Outcomes of Acute Kidney Injury in Patients Undergoing Transcatheter Aortic Valve Replacement: Insights from the Society of Thoracic Surgeons/American College of Cardiology National Cardiovascular Data Registry-Transcatheter Valve Therapy Registry. Circ. Cardiovasc. Interv. 2021, 14, e010032. [Google Scholar] [CrossRef]
- Castriota, F.; Nerla, R.; Micari, A.; Squeri, A.; Cremonesi, A. Contrast-Zero Transcatheter Aortic Valve Replacement for Patients with Severe Renal Dysfunction: A Single-Center Experience. JACC Cardiovasc. Interv. 2018, 11, 820–822. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Expansion Mechanism | Prosthesis | Manufacturer | Available | FDA Approval | CE Mark | Chinese Approval | Material | Opening Force | Radial Force | Valve Diameter (mm) | Valve Annulus Size Range | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Frame | Valve | |||||||||||
| SEV | CoreValve | Medtronic, Minneapolis, MN, USA | No | 2014 | 2007 | − | Nitinol | Porcine pericardial | + | + | 26, 29, 31 | 20–29 |
| Evolut R | Medtronic, Minneapolis, MN, USA | Yes | 2015 | 2014 | − | Nitinol | Porcine pericardial | + | ++ | 23, 26, 29, 34 | 18–30 | |
| Evolut PRO | Medtronic, Minneapolis, MN, USA | Yes | 2019 | 2017 | 2022 | Nitinol | Porcine pericardial | + | ++ | 23, 26, 29 | 18–26 | |
| Evolut PRO+ | Medtronic, Minneapolis, MN, USA | Yes | 2019 | 2021 | − | Nitinol | Porcine pericardial | + | ++ | 23, 26, 29, 34 | 18-30 | |
| Acurate TA | Boston Scientific, Marlborough, MA, USA | No | − | 2011 | − | Nitinol | Porcine pericardial | − | − | S, M, L | 21–27 | |
| Acurate Neo | Boston Scientific, Marlborough, MA, USA | Yes | − | 2014 | − | Nitinol | Porcine pericardial | − | − | S, M, L | 21–27 | |
| Acurate Neo 2 | Boston Scientific, Marlborough, MA, USA | Yes | − | 2020 | − | Nitinol | Porcine pericardial | − | − | S, M, L | 21–27 | |
| Portico | Abbott, Chicago, IL, USA | Yes | 2021 | 2012 | − | Nitinol | Bovine pericardial | − | − | 23, 25, 27, 29 | 19-27 | |
| Navitor | Abbott, Chicago, IL, USA | Yes | − | 2021 | − | Nitinol | Bovine pericardial | − | − | 23, 25, 27, 29, 35 | 19–30 | |
| Hydra | Sahajanand Medical Technologies Limited, Mumbai, India | Yes | − | 2020 | − | Nitinol | Bovine pericardial | + | + | 22, 26, 30 | 18–28 | |
| Allegra | New Valve Technology, Hechingen, Germany | Yes | − | 2017 | − | Nitinol | Bovine pericardial | + | + | 23, 27, 31 | 19–28 | |
| JenaValve | JenaValve Technology GmbH, Munich, Germany | No | − | 2011 | − | Nitinol | Bovine pericardial | − | − | 23, 25, 27 | 21–27 | |
| Trilogy | JenaValve Technology GmbH, Munich, Germany | Yes | − | 2021 | − | Nitinol | Bovine pericardial | − | − | 23, 25, 27 | 21–27 | |
| J-Valve | JC Medical Inc., Burlingame, CA, USA | Yes | − | − | 2017 | Nitinol | Bovine pericardial | + | + | 22, 25, 28 (TF) | NA | |
| Venus-A | Venus Medtech Inc., Hangzhou, China | Yes | − | − | 2017 | Nitinol | Porcine pericardial | + | ++ | 23, 26, 29, 32 | NA | |
| VitaFlow | MicroPort, Shanghai, China | Yes | − | − | 2019 | Nitinol | Bovine pericardial | + | + | 21, 24, 27, 30 | 21–30 | |
| TaurusOne | Peijia Medical, Suzhou, China | Yes | − | − | 2021 | Nitinol | Bovine pericardial | + | + | 23, 26, 29, 31 | 18–29 | |
| BEV | Sapien | Edwards Lifesciences, Irvine, CA, USA | No | 2011 | 2007 | − | SS | Bovine pericardial | ++ | + | 23, 26 | 18–25 |
| Sapien XT | Edwards Lifesciences, Irvine, CA, USA | No | 2014 | 2010 | − | CoCr | Bovine pericardial | ++ | + | 23, 26, 29 | 18–27 | |
| Sapien 3 | Edwards Lifesciences, Irvine, CA, USA | Yes | 2015 | 2014 | 2020 | CoCr | Bovine pericardial | ++ | + | 20, 23, 26, 29 | 18.6–29.5 | |
| Sapien 3 Ultra | Edwards Lifesciences, Irvine, CA, USA | Yes | 2018 | 2018 | − | CoCr | Bovine pericardial | ++ | + | 20, 23, 26 | 18.6–26.4 | |
| MyVal | Meril, Vapi, Gujarat, India | Yes | − | 2019 | − | NiCo | Bovine pericardial | ++ | − | 20–32 (every 1.5 mm) | 18–32 | |
| MEV | Lotus | Boston Scientific, Marlborough, MA, USA | No | − | 2013 | − | Nitinol | Bovine pericardial | ++ | +++ | 23, 25, 27 | 20–27 |
| Lotus Edge | Boston Scientific, Marlborough, MA, USA | No | 2019 | 2016 | − | Nitinol | Bovine pericardial | ++ | +++ | 21, 23, 25, 27, 29 | 18–29 | |
| Expansion Mechanism | Prosthesis | Valve Height (mm) | Leaflet Position | Frame Cell Size | Outer Seal | Access | Sheath | Delivery System | Repositionable | Retrievable | Commissural Alignment | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID/OD (French) | Integrated | Expandable | OD (French) | Flexible | Steerable | ||||||||||
| SEV | CoreValve | 53–55 | Supra-annular | + | − | TV, TAo | Variable | − | Variable | 18 | − | − | + | + | + |
| Evolut R | 45–46 | Supra-annular | + | − | TV/TAo | 14/18, 16/20 (34 mm) | + | − | 14, 16 | − | − | + | + | + | |
| Evolut PRO | 45 | Supra-annular | + | + | TV/TAo | 16/20 | + | − | 16 | − | − | + | + | + | |
| Evolut PRO+ | 45–46 | Supra-annular | + | ++ | TV | 14/18, 16/20 (34 mm) | + | − | 14, 16 | − | − | + | + | + | |
| Acurate TA | 44–46 | Intra-annular | +++ | − | TA | − | − | − | 28 | − | − | − | − | + | |
| Acurate Neo | 48–51 | Supra-annular | +++ | + | TV, TA | 14/23 | − | + | 18 | + | − | − | − | + | |
| Acurate Neo 2 | 48–51 | Supra-annular | +++ | ++ | TV, TA | 14/23 | − | + | 14 | + | − | − | − | + | |
| Portico | 47–51 | Intra-annular | ++ | + | TV, TAo | 14/18, 15/19 (27, 29 mm) | + | − | 18, 19 | ++ | − | + | + | + | |
| Navitor | 47–48 | Intra-annular | ++ | ++ | TV | 14/18, 15/19 (27, 29, 35 mm) | + | − | 14, 15 | ++ | − | + | + | + | |
| Hydra | 51–55 | Supra-annular | +++ | + | TV | 18/NA | − | − | 18 | + | − | + | + | + | |
| Allegra | 37–43 | Supra-annular | + | − | TV | 18/20.4 | − | − | 18 | + | − | + | + | + | |
| JenaValve | NA | Supra-annular | +++ | − | TA | − | − | − | 32 | − | − | + | − | ++ | |
| Trilogy | NA | Supra-annular | ++ | + | TV | 18 | − | − | 18 | + | + | + | − | ++ | |
| J-Valve | NA | Intra-annular | NA | − | TV/TA | NA | − | − | 18 | − | + | − | − | ++ | |
| Venus-A | NA | Supra-annular | + | + | TV | NA | NA | NA | 19 | NA | NA | + | − | NA | |
| VitaFlow | NA | Supra-annular | ++ | ++ | TV | NA | NA | NA | 16/18 | NA | NA | + | − | NA | |
| TaurusOne | NA | Supra-annular | ++ | + | TV | NA | NA | NA | 18 | NA | NA | + | − | NA | |
| BEV | Sapien | 14–16 | Intra-annular | + | − | TV/TA/TAo | 22/26, 24/28 (26 mm) | − | + | 22, 24 | − | − | − | − | − |
| Sapien XT | 14–19 | Intra-annular | + | − | TV/TA/TAo | 16/20, 18/22 (26 mm), 20/24 (29 mm) | − | + | 16, 18, 20 | − | − | − | − | − | |
| Sapien 3 | 15–22 | Intra-annular | ++ | + | TV/TA/TAo | 14/17.4, 16/20 (29 mm) | − | + | 18, 21 | − | + | − | − | − | |
| Sapien 3 Ultra | 15–20 | Intra-annular | ++ | ++ | TV | 14/17.4 | − | + | 18 | − | + | − | − | − | |
| MyVal | 17–21 | Intra-annular | ++ | ++ | TV | 14/17.4 | − | + | 14 | − | + | − | + | − | |
| MEV | Lotus | 19 | Intra-annular | + | ++ | TV, TAo | 18/22, 20/24 (25, 27 mm) | − | − | 18, 20 | − | − | ++ | ++ | − |
| Lotus Edge | 19 | Intra-annular | + | ++ | TV, TAo | 15/23.7 | − | + | 22 | + | − | ++ | ++ | − | |
| Expansion Mechanism | Prosthesis | Source | Type | Mean STS-PROM | Publication Year | N | Mortality % | MI % | Stroke % | Major Bleeding % | MVC % | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 30d | 1y | 2y | 5y | IH | 30d | 1y | 2y | 5y | IH | 30d | 1y | 2y | 5y | IH | 30d | 1y | IH | 30d | 1y | |||||||
| SEV | CoreValve | CHOICE | RCT | 6.2 | 2015 | 120 | 12.8 | 0.9 | 3.4 | 14.5 | 12.0 | |||||||||||||||
| CoreValve | NOTION | RCT | 2.9 | 2015; 2019 | 145 | 4.9 | 27.6 | 3.5 | 7.6 | 2.9 | 9.0 | 11.3 | 5.6 | |||||||||||||
| CoreValve | SURTAVI | RCT | 4.4 | 2017 | 864 | 6.7 | 11.4 | 2.0 | 2.8 | 5.4 | 6.2 | 12.2 | 6.0 | |||||||||||||
| CoreValve | REPRISE III | RCT | 6.9 | 2018; 2019 | 305 | 11.9 | 27.0 | 3.2 | 6.1 | 9.4 | 11.4 | 10.9 | 5.3 | |||||||||||||
| Evolut R | Evolut Low Risk | RCT | 1.9 | 2019; 2022 | 734 | 2.4 | 4.5 | 1.7 | 2.2 | 4.1 | 4.9 | 3.2 | 4.5 | 3.8 | 3.8 | |||||||||||
| Evolut R | SCOPE II | RCT | 2.7 | 2020 | 398 | 9 | 1 | 6 | 3 * | NA | ||||||||||||||||
| Evolut R | PORTICO-IDE | RCT | 6.2 | 2020 | 110 | 15.4 | 26.1 | NA | 5.5 | 9.1 | 4.5 | 7.2 | ||||||||||||||
| Evolut PRO | NEOPRO | Registry | 5.3 | 2019 | 288 | 2.2 | 0.4 | 2.5 | 3.9 | 3.5 | ||||||||||||||||
| Acurate Neo | Husser et al. | Registry | 18 ** | 2017 | 311 | 2.3 | NA | 2.3 | 4.2 | 10.3 | ||||||||||||||||
| Acurate Neo | SAVI TF | Registry | 6.0 | 2018 | 1000 | 8.0 | 1.3 | 3.5 | 2.0 | NA | ||||||||||||||||
| Acurate Neo | SCOPE I | RCT | 3.7 *** | 2019 | 372 | 2 | 1 | 2 | 11 | 8 | ||||||||||||||||
| Acurate Neo | NEOPRO | Registry | 5.0 | 2019 | 1263 | 3.0 | 0.6 | 2.0 | 6.8 | 6.0 | ||||||||||||||||
| Acurate Neo | SCOPE II | RCT | 3.0 | 2020 | 398 | 13 | 1 | 5 | 2 * | NA | ||||||||||||||||
| Portico | PORTICO-I | Registry | 5.8 | 2018; 2018 | 941 | 2.7 | 12.1 | 1.6 | 2.5 | 2.6 | 4.1 | 8.5 | 8.7 | 5.5 | 5.7 | |||||||||||
| Portico | PORTICO-IDE | RCT | 6.3 | 2020 | 375 | 14.6 | 22.7 | NA | 4.5 | 6.3 | 5.4 | 9.6 | ||||||||||||||
| BEV | Sapien XT | CHOICE | RCT | 5.6 | 2015 | 121 | 17.4 | 0.8 | 9.1 | 21.5 | 11.6 | |||||||||||||||
| Sapien XT | PARTNER 2A | RCT | 5.8 | 2016; 2020 | 1011 | 14.5 | 47.9 | 2.5 | 11.1 | 8.0 | 15.3 | 10.4 | 7.9 | |||||||||||||
| Sapien 3 | Sapien 3 Intermediate Risk | Registry | 5.2 | 2016 | 1077 | 4.0 | 0.3 | 4.6 | 4.6 | 6.1 | ||||||||||||||||
| Sapien 3 | Husser et al. | Registry | 18 ** | 2017 | 622 | 2.3 | NA | 2.3 | 4.2 | 10.3 | ||||||||||||||||
| Sapien 3 | Low risk TAVR | Registry | 1.8 | 2018; 2021 | 200 | 0 | 3.0 | 4.2 | 0 | 0 | 1.0 | 1.1 | 0 | 0.5 | 2.1 | 4.3 | 2.5 | 3.0 | 2.5 | 3.0 | ||||||
| Sapien 3 | PARTNER 3 | RCT | 1.9 | 2019; 2021 | 496 | 1.0 | 2.5 | 1.2 | 1.2 | 3.5 | 3.6 | 2.2 | ||||||||||||||
| Sapien 3 | SCOPE I | RCT | 3.4 *** | 2019 | 367 | 1 | 0 | 3 | 9 | 5 | ||||||||||||||||
| Sapien 3 | PORTICO-IDE | RCT | 6.5 | 2020 | 206 | 8.4 | 15.6 | NA | 6.0 | 8.0 | 4.4 | 7.3 | ||||||||||||||
| MEV | Lotus | REPRISE III | RCT | 6.7 | 2018; 2019 | 607 | 11.9 | 22.8 | 3.2 | 6.1 | 7.0 | 8.4 | 12.8 | 7.0 | ||||||||||||
| Lotus | RESPOND/Extension | Registry | 6.0 | 2017; 2019 | 996 | 2.6 | 11.7 | 0.3 | 1.9 | 3.0 | 4.9 | 2.6 * | 3.6 | 3.4 | 3.4 | |||||||||||
| Expansion | Prosthesis | Source | Type | AKI % | PPI % | Gradient | EOA cm2 | Severe PPM | Mild PVL | Moderate or More PVL | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IH | 30d | 1y | IH | 30d | 1y | IH | 30d | 1y | 2y | 5y | 30d | 1y | 2y | 5y | 30d | IH | 30d | 1y | 2y | 5y | IH | 30d | 1y | 2y | 5y | ||||
| SEV | CoreValve | CHOICE | RCT | NA | 38.0 | 38.0 | 1.8 (0.6) | NA | 39.6 | 12.1 | |||||||||||||||||||
| CoreValve | NOTION | RCT | 0.7 | 34.1 | 34.1 | 1.7 | 1.7 | NA | 55.4 | 52.9 | 15.7 | 8.2 | |||||||||||||||||
| CoreValve | SURTAVI | RCT | 1.7 | 25.9 | 25.9 | 2.2 (0.6) | 2.2 (0.7) | NA | 31.9 | 32.8 | 5.3 | 3.9 | |||||||||||||||||
| CoreValve | REPRISE III | RCT | 3.6 | 19.6 | 19.6 | 2.0 (0.5) | 1.8 (0.5) | NA | 38.8 | 6.8 | 3.8 | ||||||||||||||||||
| Evolut R | Evolut Low Risk | RCT | 0.9 | 17.4 | 17.4 | 2.3 (0.7) | 2.2 (0.5) | 1.1 | 33.1 | 26.6 | 3.7 | 1.7 | |||||||||||||||||
| Evolut R | SCOPE II | RCT | NA | 9 | 18 | 18 | 1.8 (0.5) | 1.8 (0.6) | NA | 52.2 | 35.9 | 2.9 | 3.3 | ||||||||||||||||
| Evolut R | PORTICO-IDE | RCT | 2.7 | 18.8 | 18.8 | 1.9 (0.4) | 1.8 (0.5) | 4 | NA | 4.0 | 0 | ||||||||||||||||||
| Evolut PRO | NEOPRO | Registry | 2.1 | 13.2 | 13.2 | 2.5 | NA | 42.1 | 5.8 | ||||||||||||||||||||
| Acurate Neo | Husser et al. | Registry | 3.2 | 10.2 | 10.2 | 4.2 | NA | 4.8 | NA | ||||||||||||||||||||
| Acurate Neo | SAVI TF | Registry | NA | 9.9 | 9.9 | 1.8 (0.4) | NA | 40.4 | 1.8 | ||||||||||||||||||||
| Acurate Neo | SCOPE I | RCT | 8 | 10 | 10 | 2 | 1.7 | NA | 50.1 | 9.4 | |||||||||||||||||||
| Acurate Neo | NEOPRO | Registry | 3.1 | 8.8 | 8.8 | 2.0 | NA | 56.9 | 5.2 | ||||||||||||||||||||
| Acurate Neo | SCOPE II | RCT | NA | 11 | 11 | 1.7 (0.5) | 1.8 (0.5) | 6 | 63.2 | 57.3 | 9.6 | 4.0 | |||||||||||||||||
| Portico | PORTICO-I | Registry | 3.0 | 4.2 | 18.7 | 21.3 | 18.7 | 21.3 | 2.6 | 1.8 (0.5) | 1.7 (0.5) | NA | 67.6 | 67.9 | 3.9 | 2.6 | |||||||||||||
| Portico | PORTICO-IDE | RCT | 3.0 | 28.1 | 28.1 | 1.8 (0.5) | 1.9 (0.5) | NA | NA | 6.1 | 5.2 | ||||||||||||||||||
| BEV | Sapien XT | CHOICE | RCT | NA | 17.4 | 23.4 | 23.4 | 1.7 (0.4) | NA | 40.4 | 1.1 | ||||||||||||||||||
| Sapien XT | PARTNER 2A | RCT | 1.3 | 8.5 | 8.5 | 1.6 (0.5) | 1.5 | NA | 23.2 | 17.0 | 3.4 | 4.1 | |||||||||||||||||
| Sapien 3 | Sapien 3 Intermediate Risk | Registry | 0.5 | 10.2 | 10.2 | 1.7 (0.4) | NA | 30.3 | 0 | ||||||||||||||||||||
| Sapien 3 | Husser et al. | Registry | 3.2 | 10.2 | 10.2 | 10.3 | NA | NA | |||||||||||||||||||||
| Sapien 3 | Low risk TAVR | Registry | 0 | 0 | 5.0 | 6.5 | 7.3 | 5.0 | 6.5 | 7.3 | 0 | 0.5 | 1.6 (0.4) | 1.7 (0.5) | 1.7 (0.5) | NA | 31.1 | 0.5 | 1.5 | 0 | |||||||||
| Sapien 3 | PARTNER 3 | RCT | 0.4 | 7.9 | 9.1 | 7.9 | 9.1 | 1.7 (0.02) | 1.7 (0.37) | 8.3 | 25.1 | 24.3 | 20.0 | 0.8 | 0.8 | 0.5 | |||||||||||||
| Sapien 3 | SCOPE I | RCT | 7 | 9 | 9 | 3 | 1.5 | NA | 31.1 | 2.8 | |||||||||||||||||||
| Sapien 3 | PORTICO-IDE | RCT | 0.5 | 5.4 | 5.4 | 8.0 | 1.6 (0.4) | 1.6 (0.5) | NA | NA | 1.6 | 0.8 | |||||||||||||||||
| MEV | Lotus | REPRISE III | RCT | 2.5 | 35.5 | 35.5 | 1.6 (0.5) | 1.5 (0.5) | NA | 11.3 | 0.9 | 0.3 | |||||||||||||||||
| Lotus | RESPOND/Extension | Registry | 1.7 | 1.7 | 34.6 | 37.2 | 34.6 | 37.2 | 3.0 | 1.8 (0.4) | 1.8 (0.4) | NA | 7.7 | 5.5 | 0.3 | 0.4 | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leone, P.P.; Scotti, A.; Ho, E.C.; Assafin, M.; Doolittle, J.; Chau, M.; Slipczuk, L.; Levitus, M.; Regazzoli, D.; Mangieri, A.; et al. Prosthesis Tailoring for Patients Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2023, 12, 338. https://doi.org/10.3390/jcm12010338
Leone PP, Scotti A, Ho EC, Assafin M, Doolittle J, Chau M, Slipczuk L, Levitus M, Regazzoli D, Mangieri A, et al. Prosthesis Tailoring for Patients Undergoing Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine. 2023; 12(1):338. https://doi.org/10.3390/jcm12010338
Chicago/Turabian StyleLeone, Pier Pasquale, Andrea Scotti, Edwin C. Ho, Manaf Assafin, James Doolittle, Mei Chau, Leandro Slipczuk, Matthew Levitus, Damiano Regazzoli, Antonio Mangieri, and et al. 2023. "Prosthesis Tailoring for Patients Undergoing Transcatheter Aortic Valve Implantation" Journal of Clinical Medicine 12, no. 1: 338. https://doi.org/10.3390/jcm12010338