
The Effect of Age on Non-Invasive Hemodynamics in Chronic Heart Failure Patients on Left-Ventricular Assist Device Support: A Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
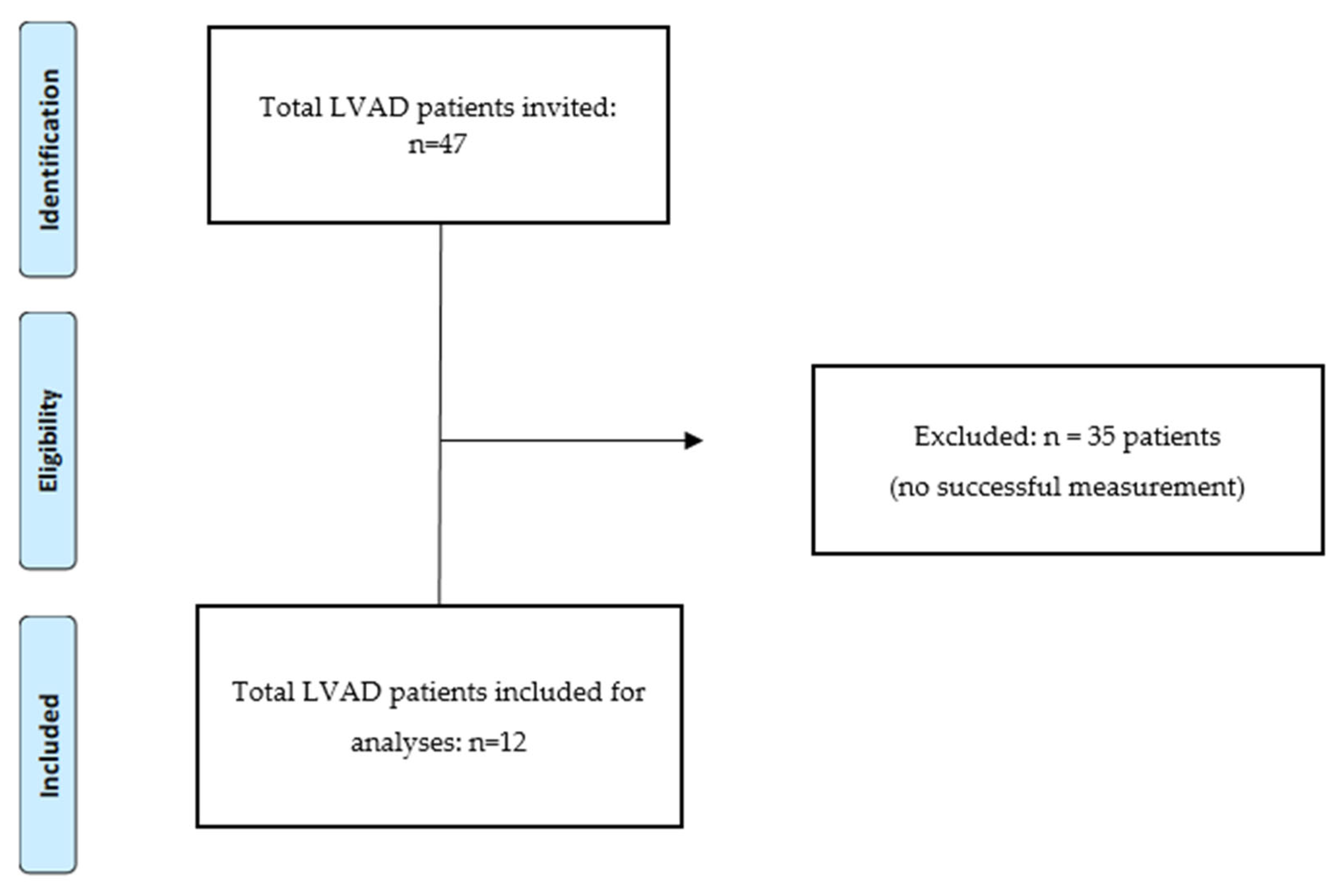
2.1. Patient Selection
2.2. Variables
2.3. Hemodynamic Data
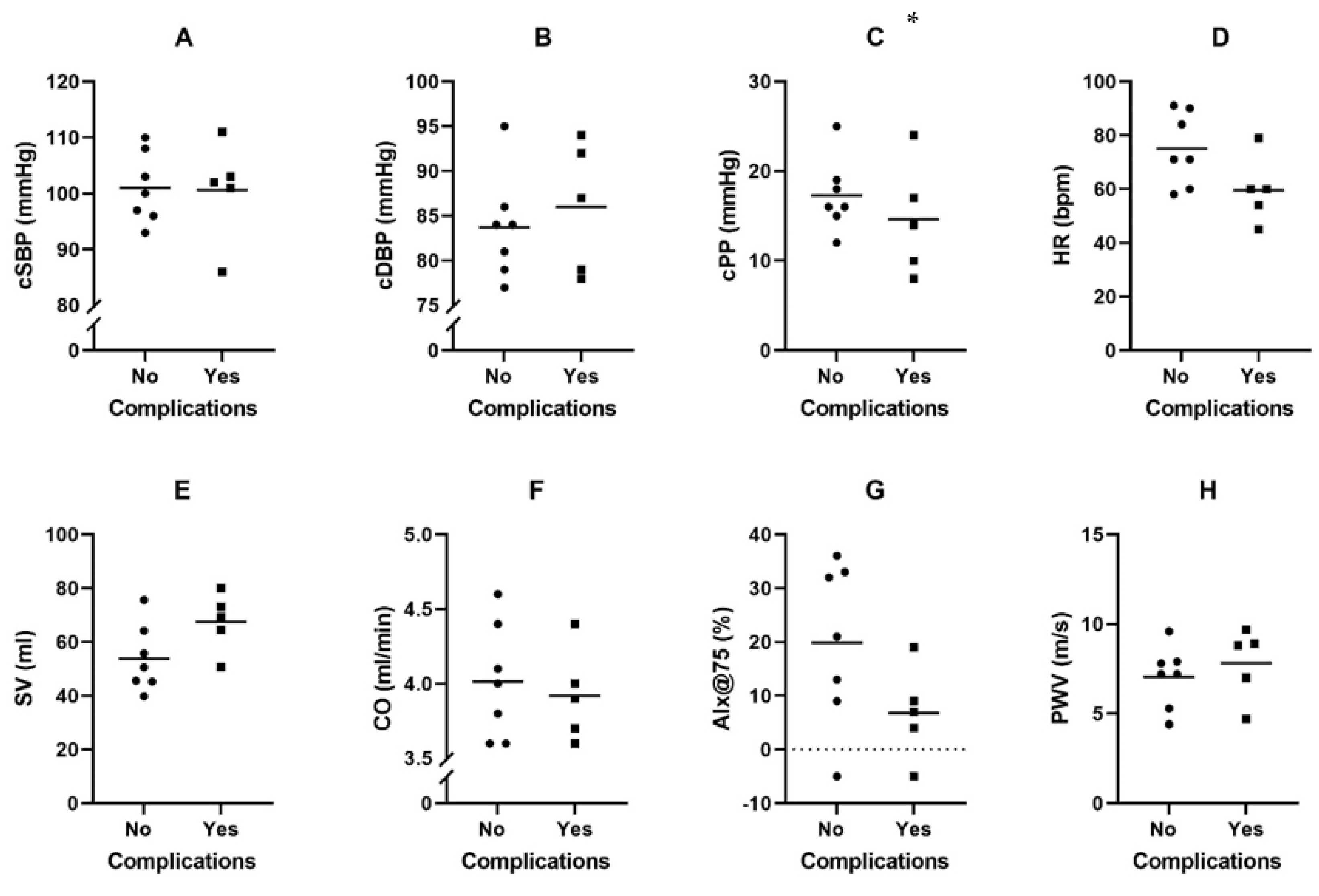
2.4. Adverse Events Registration
2.5. Statistical Analysis
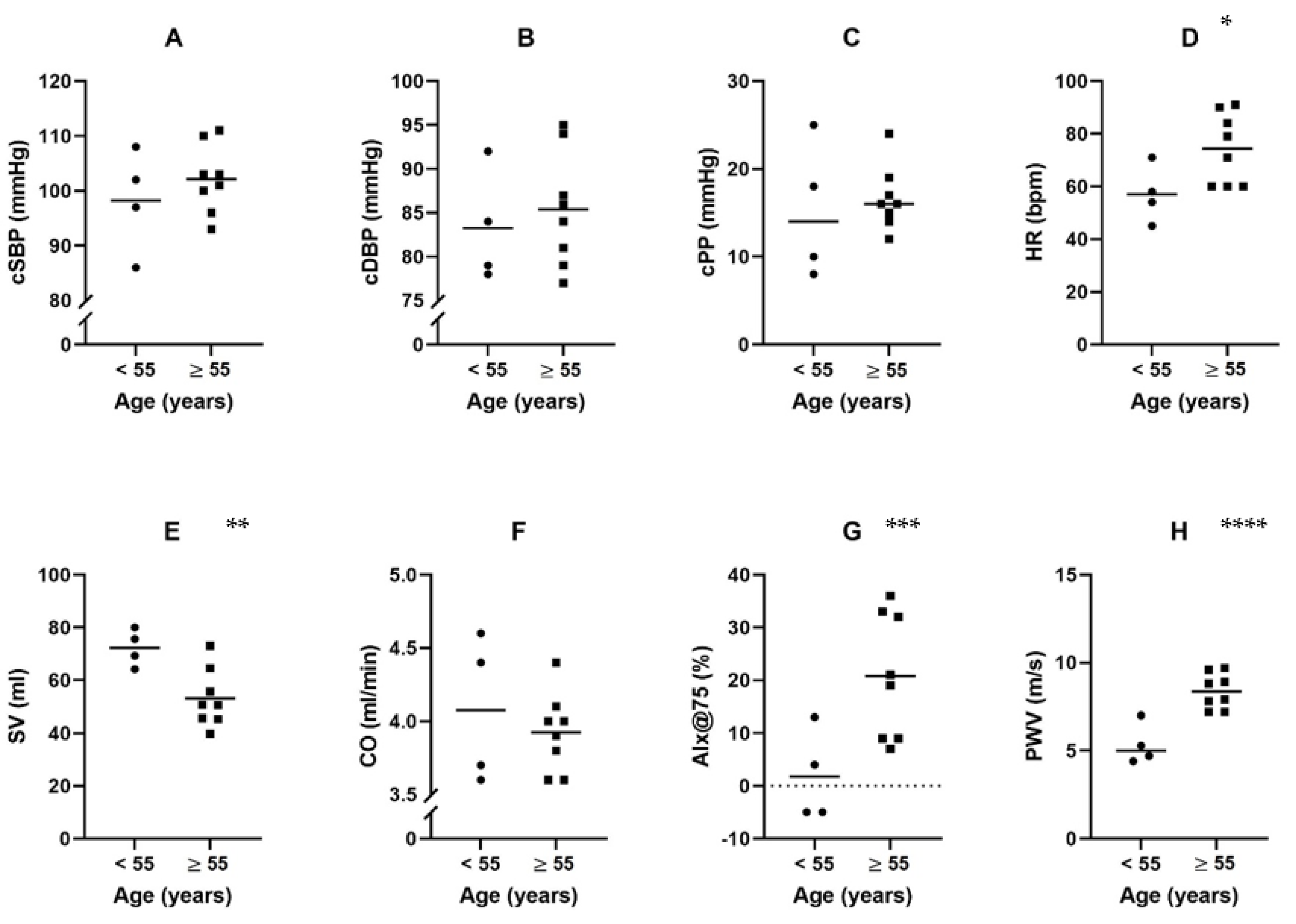
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, S.; Nicholson, L.; Cassidy, C.J.; Wong, K.Y. Left ventricular assist device: A bridge to transplant or destination therapy? Postgrad. Med. J. 2016, 92, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Frazier, O.H.; Rose, E.A.; Oz, M.C.; Dembitsky, W.; McCarthy, P.; Radovancevic, B.; Poirier, V.L.; Dasse, K.A.; HeartMate LVAS Investigators. Multicenter clinical evaluation of the HeartMate vented electric left ventricular assist system in patients awaiting heart transplantation. J. Thorac. Cardiovasc. Surg. 2001, 122, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slaughter, M.S.; Singh, R. The role of ventricular assist devices in advanced heart failure. Rev. Esp. Cardiol. Engl. Ed. 2012, 65, 982–985. [Google Scholar] [CrossRef] [PubMed]
- Bleumink, G.S.; Knetsch, A.M.; Sturkenboom, M.C.; Straus, S.M.; Hofman, A.; Deckers, J.W.; Witteman, J.C.; Stricker, B.H. Quantifying the heart failure epidemic: Prevalence, incidence rate, lifetime risk and prognosis of heart failure The Rotterdam Study. Eur. Heart J. 2004, 25, 1614–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, E.A.; Gelijns, A.C.; Moskowitz, A.J.; Heitjan, D.F.; Stevenson, L.W.; Dembitsky, W.; Long, J.W.; Ascheim, D.D.; Tierney, A.R.; Levitan, R.G.; et al. Long-term use of a left ventricular assist device for end-stage heart failure. N. Engl. J. Med. 2001, 345, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, M.S.; Rogers, J.G.; Milano, C.A.; Russell, S.D.; Conte, J.V.; Feldman, D.; Sun, B.; Tatooles, A.J.; Delgado, R.M., III; Long, J.W.; et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N. Engl. J. Med. 2009, 361, 2241–2251. [Google Scholar] [CrossRef] [Green Version]
- Kirklin, J.K.; Naftel, D.C.; Kormos, R.L.; Pagani, F.D.; Myers, S.L.; Stevenson, L.W.; Givertz, M.M.; Young, J.B. Quantifying the effect of cardiorenal syndrome on mortality after left ventricular assist device implant. J. Heart Lung Transpl. 2013, 32, 1205–1213. [Google Scholar] [CrossRef]
- Rosenblum, H.; Pinsino, A.; Zuver, A.; Javaid, A.; Mondellini, G.; Ji, R.; Cockcroft, J.R.; Yuzefpolskaya, M.; Garan, A.R.; Shames, S.; et al. Increased Aortic Stiffness Is Associated with Higher Rates of Stroke, Gastrointestinal Bleeding and Pump Thrombosis in Patients With a Continuous Flow Left Ventricular Assist Device. J. Card. Fail. 2021, 27, 696–699. [Google Scholar] [CrossRef]
- Imamura, T.; Nguyen, A.; Kim, G.; Raikhelkar, J.; Sarswat, N.; Kalantari, S.; Smith, B.; Juricek, C.; Rodgers, D.; Ota, T.; et al. Optimal haemodynamics during left ventricular assist device support are associated with reduced haemocompatibility-related adverse events. Eur. J. Heart Fail. 2019, 21, 655–662. [Google Scholar] [CrossRef]
- Castagna, F.; McDonnell, B.J.; Stöhr, E.J.; Yuzefpolskaya, M.; Trinh, P.N.; Topkara, V.K.; Garan, A.R.; Flannery, M.A.; Takeda, K.; Takayama, H.; et al. Non-invasive measurement of peripheral, central and 24-hour blood pressure in patients with continuous-flow left ventricular assist device. J. Heart Lung Transpl. 2017, 36, 694–697. [Google Scholar] [CrossRef]
- Hametner, B.; Wassertheurer, S.; Kropf, J.; Mayer, C.; Eber, B.; Weber, T. Oscillometric estimation of aortic pulse wave velocity: Comparison with intra-aortic catheter measurements. Blood Press. Monit. 2013, 18, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.K.; Roberts, C.A.; Dordunoo, D.; Shah, A.; Russell, S.D. Ideal methodology to assess systemic blood pressure in patients with continuous-flow left ventricular assist devices. J. Heart Lung Transpl. 2010, 29, 593–594. [Google Scholar] [CrossRef] [PubMed]
- Castagna, F.; McDonnell, B.; Yuzefpolskaya, M.; Topkara, V.; Garan, A.; Willey, J.; Trinh, P.; Wong, K.; Cagliostro, B.; Flannery, M.; et al. Validity and Reliability of a Next Generation Non-Invasive Blood Pressure Monitor in Patients with Continuous-Flow Left Ventricular Assist Device. J. Heart Lung Transpl. 2016, 35, S326–S327. [Google Scholar] [CrossRef]
- Barić, D. Why pulsatility still matters: A review of current knowledge. Croat. Med. J. 2014, 55, 609–620. [Google Scholar] [CrossRef] [Green Version]
- Schofield, R.S.; Pierce, G.L.; Nichols, W.W.; Klodell, C.T.; Aranda, J.M.; Pauly, D.F.; Hill, J.A.; Braith, R.W. Arterial-wave reflections are increased in heart failure patients with a left-ventricular assist device. Am. J. Hypertens. 2007, 20, 622–628. [Google Scholar] [CrossRef] [Green Version]
- Houghton, D.; Jones, T.W.; Cassidy, S.; Siervo, M.; MacGowan, G.A.; Trenell, M.I.; Jakovljevic, D.G. The effect of age on the relationship between cardiac and vascular function. Mech. Ageing Dev. 2016, 153, 1–6. [Google Scholar] [CrossRef]
- Mattace-Raso, F.; van der Cammen, T.J.; Hofman, A.; van Popele, N.M.; Bos, M.L.; Schalekamp, M.A.; Asmar, R.; Reneman, R.S.; Hoeks, A.P.; Breteler, M.M.; et al. Arterial stiffness and risk of coronary heart disease and stroke: The Rotterdam study. Circulation 2006, 113, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A. Arterial stiffness and cardiovascular events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Styczynski, G.; Cienszkowska, K.; Ludwiczak, M.; Szmigielski, C. Age-related values of aortic pulse wave velocity in healthy subjects measured by Doppler echocardiography. J. Hum. Hypertens. 2021, 35, 1081–1087. [Google Scholar] [CrossRef]
- Fantin, F.; Mattocks, A.; Bulpitt, C.J.; Banya, W.; Rajkumar, C. Is augmentation index a good measure of vascular stiffness in the elderly? Age Ageing 2007, 36, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckmann, M.; Jacomella, V.; Kohler, M.; Lachat, M.; Salem, A.; Amann-Vesti, B.; Husmann, M. Risk Stratification of Patients with Peripheral Arterial Disease and Abdominal Aortic Aneurysm Using Aortic Augmentation Index. PLoS ONE 2015, 10, e0139887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirklin, J.K.; Naftel, D.C.; Pagani, F.D.; Kormos, R.L.; Stevenson, L.W.; Blume, E.D.; Miller, M.A.; Baldwin, J.T.; Young, J.B. Sixth INTERMACS annual report: A 10,000-patient database. J. Heart Lung Transpl. 2014, 33, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, A.; Cogswell, R.; John, R. Future developments in left ventricular assist device therapy. J. Thorac. Cardiovasc. Surg. 2021, 162, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Markham, D.W.; Fu, Q.; Palmer, M.D.; Drazner, M.H.; Meyer, D.M.; Bethea, B.T.; Hastings, J.L.; Fujimoto, N.; Shibata, S.; Levine, B.D. Sympathetic neural and hemodynamic responses to upright tilt in patients with pulsatile and nonpulsatile left ventricular assist devices. Circ. Heart Fail. 2013, 6, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Pinsino, A.; Castagna, F.; Zuver, A.M.; Royzman, E.A.; Nasiri, M.; Stöhr, E.J.; Cagliostro, B.; McDonnell, B.; Cockcroft, J.R.; Garan, A.R.; et al. Prognostic implications of serial outpatient blood pressure measurements in patients with an axial continuous-flow left ventricular assist device. J. Heart Lung Transpl. 2019, 38, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Cappell, M.S.; Lebwohl, O. Cessation of recurrent bleeding from gastrointestinal angiodysplasias after aortic valve replacement. Ann. Intern. Med. 1986, 105, 54–57. [Google Scholar] [CrossRef]
- Crow, S.; John, R.; Boyle, A.; Shumway, S.; Liao, K.; Colvin-Adams, M.; Toninato, C.; Missov, E.; Pritzker, M.; Martin, C.; et al. Gastrointestinal bleeding rates in recipients of nonpulsatile and pulsatile left ventricular assist devices. J. Thorac. Cardiovasc. Surg. 2009, 137, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.C.; Dodson, R.B.; Cornwell, W.K.; Hunter, K.S.; Cleveland, J.C.; Brieke, A.; Lindenfeld, J.; Ambardekar, A.V. Dynamic Changes in Aortic Vascular Stiffness in Patients Bridged to Transplant with Continuous-Flow Left Ventricular Assist Devices. JACC Heart Fail. 2017, 5, 449–459. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Successful Measurement (12) | Failed Measurement (35) | p-Value |
|---|---|---|---|
| Age, years, IQR | 57 (34–66) | 60 (53–64) | ns |
| Sex, men, n (%) | 10 (83.3) | 30 (85.7) | ns |
| Weight, kg | 80 (78–96) | 88.2 (77.6–101.2) | ns |
| BMI, kg/m2 | 26.6 (25.3–30) | 27.8 (25.3–30.0] | ns |
| Time on LVAD, months | 19.5 (3–30) | 23 (13–41] | ns |
| Etiology of HF, ischemic, % (n) | 58.3 (7) | 57.1 (20) | ns |
| Smoking, % | 2 (16.7) | 2 (5.7) | ns |
| Diabetes, % | 2 (16.7) | 5 (14.3) | ns |
| Hypertension, % | 2 (16.7) | 6 (17.1) | ns |
| LVAD device type, HM-3, % (n) | 11 (91.7) | 35 (100) | ns |
| SBP, mmHg | 108 (104–116) | 102 (99–112) | ns |
| MAP, mmHg | 93 (84–96) | 85 (82–90) | ns |
| DBP, mmHg | 83 (75–87) | 79 (73–84) | ns |
| PP, mmHg | 23 (17–28) | 26 (23–30) | ns |
| LVAD parameters | |||
| • RPM, r/min | 5300 (5200–5400) | 5400 (5300–5500) | ns |
| • Flow, L/min | 4.4 (4.1–4.5) | 4.6 (4.3–4.9) | 0.014 |
| • PI | 4.4 (3.9–5.7) | 3.6 (2.9–4.40) | 0.002 |
| • Pulse Power, Watt | 3.8 (3.8–4) | 4.0 (3.8–4.2) | ns |
| eGFR, ml/min/1.73 m2 | 69 (63–90) | 60.0 (43–77) | ns |
| Hb, mmol/L | 8.7 (7.7–9) | 8.6 (7.8–9.3) | ns |
| Bilirubin, µmol/L | 9.0 (8–16) | 11.0 (8–17) | ns |
| NT-proBNP, pmol/L | 152 (99–213) | 190 (138–390) | 0.057 |
| Characteristics | Age < 55 Years (n = 4) | Age ≥ 55 Years (n = 6) | p-Value |
|---|---|---|---|
| Age, years, IQR | 33 (24.5–49) | 62 (57–72) | <0.001 |
| Sex, men, n (%) | 4 (100) | 6 (75) | ns |
| Weight, kg | 81.7 (77.9–112.6) | 80 (78–96) | ns |
| BMI, kg/m2 | 25.7 (29.4–25.2) | 27.9 (25.7–29.9) | ns |
| Time since LVAD, months | 29 (14.3–66.3) | 6.0 (2–25) | ns |
| Etiology of HF, ischemic, n (%) | 0 | 7 (87.5) | 0.004 |
| Smoking, % | 0 | 2 (25) | ns |
| Diabetes, % | 1 (25) | 1 (12.5) | ns |
| Hypertension, % | 0 | 2 (25) 25% (2) | ns |
| LVAD device type, HM-III, % (n) | 1 (25) | 0 | ns |
| SBP, mmHg | 108.5 (98.3–117.3) | 108 (104–116) | ns |
| MAP, mmHg | 90 (78.8–96) | 93 (87–95) | ns |
| DBP, mmHg | 79.5 (69.8–88.5) | 83 (80–87) | ns |
| PP, mmHg | 25 (21.3–33.3) | 23 (15–28) | ns |
| LVAD parameters | |||
| • RPM, r/min | 5250 (5200–7350) | 5300 (5250–5250) | ns |
| • Flow, L/min | 4.4 (4.1–4.5) | 4.4 (4.2–4.5) | ns |
| • PI | 5.1 (4.5–6.4) | 4.1 (3.9–4.6) | ns |
| • Pulse Power, Watt | 4.0 (3.8–4.8) | 3.8 (3.8–4.0) | ns |
| eGFR, m/min/1.73 m2 | 75.7 (67.5–86) | 63 (54–83.5) | ns |
| Hb, mmol/L | 9.0 (8.6–9.3) | 8.4 (7.7–8.9) | ns |
| Bilirubin, µmol/L | 16 (7.5–29) | 9 (8.5–10.5) | ns |
| NT-proBNP, pmol/L | 117.5 (39.5–201) | 152 (120–215) | ns |
| Characteristics | LVAD without Adverse Event (7) | LVAD with Any Adverse Event (5) | p-Value |
|---|---|---|---|
| Age, years | 57.5 (29.5–63) | 55 (44–72) | ns |
| Sex, men, n (%) | 5 (71.4) | 5 (100) | ns |
| Weight, kg | 78.5 (77.5–86.6) | 96 (79.5–110.1) | ns |
| BMI, kg/m2 | 25.8 (24.7–28.1) | 30 (25.9–30.4) | ns |
| Time since LVAD, months | 13.5 (1.75–28) | 28.3 (7.5–53) | ns |
| Etiology of HF, ischemic, % (n) | 57.1 (4) | 60 (3) | ns |
| Smoking, % | 2 (28.6) | 0 | ns |
| Diabetes, % | 0 | 2 (40) | ns |
| Hypertension, % | 2 (28.6) | 0 | ns |
| LVAD device type, HM-III, % (n) | 6 (100) | 4 (80) | ns |
| SBP, mmHg | 112 (102–118.3) | 107 (102–113) | ns |
| MAP, mmHg | 93.5 (84.5–97.8) | 91 (777–95.5) | ns |
| DBP, mmHg | 82.5 (77–89.3) | 83 (65.5–88) | ns |
| PP, mmHg | 20 (14.8–29.8) | 24 (21.5–32.5) | ns |
| LVAD parameters | |||
| • RPM, r/min | 5300 (5175–5300) | 5400 (5200–5400) | ns |
| • Flow, L/min | 4.3 (3.9–4.4) | 4.5 (4.3–4.5) | ns |
| • PI | 4.2 (3.7–7.6) | 4.4 (4.2–5.3) | ns |
| • Pulse Power, Watt | 3.8 (3.7–4.0) | 3.9 (3.8–4.7) | ns |
| eGFR, mL/min/1.73 m2 | 73 (58.5–84) | 66 (54–90) | ns |
| Hb, mmol/L | 8 (7.7–9.5) | 9 (8.6–9) | ns |
| Bilirubin, µmol/L | 9 (6.8–12.8) | 12 (8–25) | ns |
| NT-proBNP, pmol/L | 162 (90.2–256.5) | 152 (66–212) | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Vreede, E.-M.; van den Berg, F.; Jahangiri, P.; Caliskan, K.; Mattace-Raso, F. The Effect of Age on Non-Invasive Hemodynamics in Chronic Heart Failure Patients on Left-Ventricular Assist Device Support: A Pilot Study. J. Clin. Med. 2023, 12, 29. https://doi.org/10.3390/jcm12010029
van de Vreede E-M, van den Berg F, Jahangiri P, Caliskan K, Mattace-Raso F. The Effect of Age on Non-Invasive Hemodynamics in Chronic Heart Failure Patients on Left-Ventricular Assist Device Support: A Pilot Study. Journal of Clinical Medicine. 2023; 12(1):29. https://doi.org/10.3390/jcm12010029
Chicago/Turabian Stylevan de Vreede, Else-Marie, Floor van den Berg, Parsa Jahangiri, Kadir Caliskan, and Francesco Mattace-Raso. 2023. "The Effect of Age on Non-Invasive Hemodynamics in Chronic Heart Failure Patients on Left-Ventricular Assist Device Support: A Pilot Study" Journal of Clinical Medicine 12, no. 1: 29. https://doi.org/10.3390/jcm12010029