1. Introduction
Research shows as many as 85% of two-year-old children with cerebral palsy (CP) present with communication impairment, with only 10% expected to outgrow their delay by 4 years of age [
1]. Early communication difficulties in young children with CP may be associated with sensory, motor and/or cognitive impairment [
2] and are predictive of later language difficulties [
3,
4] that place children at risk of educational and social disadvantage and long-term activity and participation limitations [
5].
Recent advances in the early identification of CP have seen the development of specific motor interventions for children less than two years of age [
6,
7]. These interventions were designed to mitigate the cascading consequences of impairment by capitalising on sensitive periods of neuroplasticity in early development [
8,
9]. In contrast, no such evidence-base of interventions exist for early communication impairment for children at-risk of CP [
10]. This is despite the recognition that children who cross performance thresholds “earlier in life have better outcomes later” [
11], p. 1609 and research demonstrating the impact of multi-modal experiences during sensitive periods of early development on later language learning [
12].
For example, Kuhl and colleagues [
9,
12] identify the period between 6 months and 12 months of age as a sensitive period for phonetic learning, representing the earliest milestone in language acquisition [
13]. The shaping or attunement of early speech perception and production to a child’s native language is highly dependent on the multi-modal and bidirectional communicative exchanges that take place between a parent and infant [
14]. Research has shown that infants of caregivers who engage in a high proportion of contingent communicative interactions show greater attunement and produce more mature vocalisations [
15], with a direct positive influence on vocabulary development [
16,
17].
Moreover, there is good evidence to show that infant vocalisations provide a significant foundation for speech and language learning, as well as social, emotional, and cognitive abilities [
18,
19,
20]. Infant vocalisations considered precursors to speech are termed protophones [
21]. They follow a developmental trajectory of increasing vocal control and complexity [
17]. For example, infants progress from pre-canonical vocalisations such as marginal babbling, containing consonant-like (closant) and vowel-like (vocant) elements with slow movement transitions, through to the canonical babble stage that features speech-like consonant–vowel (CV) syllables with quick transitions [
22]. Whilst the age of emergence varies, it is typically reported infants gain control of basic canonical syllables between 5 and 10 months of age [
21]. The canonical babbling stage progresses to more advanced or motorically complex forms and provides a foundation for the child to produce their first words with communicative intent. From this perspective, delays or restrictions in the development of infant vocalizations due to an underlying deficit should be predictive of ongoing constraints on the expansion of these vocal production skills into intelligible language, hence, contributing to communication impairment. Consistent with this expectation, research has shown that delayed emergence of canonical syllables predicts poor expressive language, particularly, vocabulary development, in children [
18,
20]. Furthermore, recent research focusing on identifying biomarkers in infant vocalisations [
23,
24] has been undertaken in children with neurodevelopmental conditions, such as autism [
25] and Down Syndrome [
26], contributing to the development of targeted early interventions designed to ameliorate the impact of communication impairment. The development of infant vocalisations in children with CP with the potential to identify communication impairment and intervene early has received limited attention.
In 1999, Levin [
27] reported on the vocalisations of eight, 12-month-old infants with CP. The babbling of all eight participants was limited to monosyllables with the phonetic repertoire comprised largely of back vowels, plosives and velars. These vocal behaviors were associated with limited oral motor control that included the speech subsystems of respiration, phonation and articulation. Nyman and Lohmander [
28] also reported on the canonical babble in three children with CP, representing a subset of 18 children with neurodevelopmental disability. They identified children with CP presented with significantly lower levels of canonical babble and limited phonetic repertoire. More recently, Ward et al. [
29] reported longitudinal data of 18 infants with CP, as compared to TD infants, utilising the Infant Monitor of vocal Production (IMP). They identified divergence from typical development in the vocalisations of infants with CP at 9 and 12 months of age suggesting delays in the transition from the pre-canonical to canonical babble stage. Collectively, these findings provide evidence of impaired emergence of speech motor control in very young children with CP, and represent an opportunity for the development of CP specific early interventions to benefit their early speech production skills and subsequent communication development.
Currently, a multi-modal approach to very early intervention is recommended [
30]. This includes supporting the social foundations of communication (i.e., joint attention for engagement, and play); building comprehension to facilitate the transition to spoken language [
31]; and providing access to expressive communication including building speech production, all embedded in the child’s routine to increase opportunities of practice of targeted skills [
32]. These principles are consistent with research showing interventions that target parent–child interactions benefit the development of expressive language skills in children at risk of language impairment [
33]. However, few interventions to date have been directed at the development of early vocalisations in infants at risk of motor-speech impairments including infants at risk of CP [
34,
35,
36].
In light of the above, this paper reports on a multi-modal case-series intervention for children under 24 months with communication impairment associated with CP. Consideration was given to recommendations for principles of early communication intervention [
33], including CP specific early intervention [
10], and theoretical constructs that consider a child’s development to arise from bi-directional interactions within the physical, social, cognitive and environmental domains.
The PROMPT approach we adopted in the present study encompasses each of the aforementioned elements [
37]. PROMPT has previously been used in children with CP [
38] and found to be effective in improving speech motor control and intelligibility in children aged 3 years to 14 years. It is an empirically supported and manualised approach guided by key tenets of Dynamic Systems Theory, as illustrated within the PROMPT conceptual framework [
37]. Clinicians undertake a dynamic assessment of the physical–sensory, cognitive linguistic and social emotional domains utilising the Global Domain Evaluation to determine intervention goals and priorities for functional communication. This is based on the presumption that “all domains interact during communication and that audition and somatosensory information are equally important in the development and organisation of motor-speech behaviour” [
37], p. 477. PROMPT trained clinicians will “alternate” their treatment priorities between the communication domains, with the first intervention priority chosen to achieve the greatest shift. For example, intervention with a child who is pre-linguistic and not engaging in reciprocity, will focus on the social–emotional domain, as their priority. All intervention goals and objectives are functionally motivated and developed with consideration given to the child’s and family’s environment, and sufficient opportunity for repetition and practice within the daily routine.
Within the physical–sensory domain, three intervention priorities are determined using the Systems Analysis Observation and Motor Speech Hierarchy (MSH) [
37]. The MSH represents seven stages of motor-speech subsystem control and based upon the inter-hierarchical sequence of motor-speech development [
39].
A PROMPT session must include tactile input that is used to (a) create an interactive awareness for communication with intention; (b) provide associative mapping for cognitive-linguistic input; and/or (c) develop speech subsystems at the sound, word, or phrase level. In addition to behavioural based studies that have demonstrated modifications to the speech system brought about through tactile input [
40], more recent exploratory work by Fiori et al. [
41] has identified neural changes in participants subsequent to intervention.
In summary, this study tests the hypothesis that intervention started before 2 years of age, framed within the PROMPT approach and utilising tactile input, will improve the vocal complexity of children with communication impairment secondary to CP. The single-subject experimental methodology was selected to (a) demonstrate proof-of-concept for a multi-modal intervention, focused on speech sound practice for young children at risk of communication impairment secondary to CP; (b) inform a larger scale research design; and (c) accommodate the heterogeneity of the participants.
Three intervention blocks, each using an ABA sequence, were designed to build successive complexity as follows. Block one focused primarily on preparing the child for learning by building social interaction and reciprocity, teaching targeted words within home-based daily routines and play activities. The tactile input was timed to precede or follow the turn-taking routine, avoiding disruption to the reciprocity of the interaction. It was hypothesised the tactile input during block one intervention would contribute to achieving the vocal production priorities developed for each child, our primary outcome of interest, although these changes may be minimal or not consistently sustained.
In contrast, block two and three focused more directly on building the complexity and diversity of vocalisations/speech produced with communicative intent and increasing motor control, in accordance with the developed motor-speech priorities for each child in each block. The tactile input was provided to shape articulator (i.e., motor) movements during speech production. It was hypothesised that intervention blocks two and three would be associated with an increase in the use of target vocal patterns or protophones (e.g., CV syllable production) and associated speech movements (e.g., closed to open and open to closed jaw transitions with phonation control) during vocal elicitation tasks.
Each intervention block included three word sets that targeted increasing motor control, as based on the MSH. Word set 1 contained words with the lowest level of complexity, targeted intervention priority one and were trained throughout the whole intervention phase. As Word set 2 contained a higher level of complexity, these were introduced half-way through the intervention phase to allow initial focus on the priority one word set. Word set 3 represented intervention priority three. These words acted as a control and were not actively trained but were embedded within meaningful daily interactions.
It was hypothesised a treatment effect would be observed for trained items that were part of the intervention. Untrained items, that is, different words containing the same target protophones and requiring the same speech movement pattern, were included in the elicitation tasks to test for generalisation effects to other items. The third word set represents the control goal and as such no treatment effect was expected.
3. Results
The speech probe data plotted across the study phases for each intervention block are shown in
Figure 2,
Figure 3 and
Figure 4 for P1,
Figure 5,
Figure 6 and
Figure 7 for P2, and
Figure 8 and
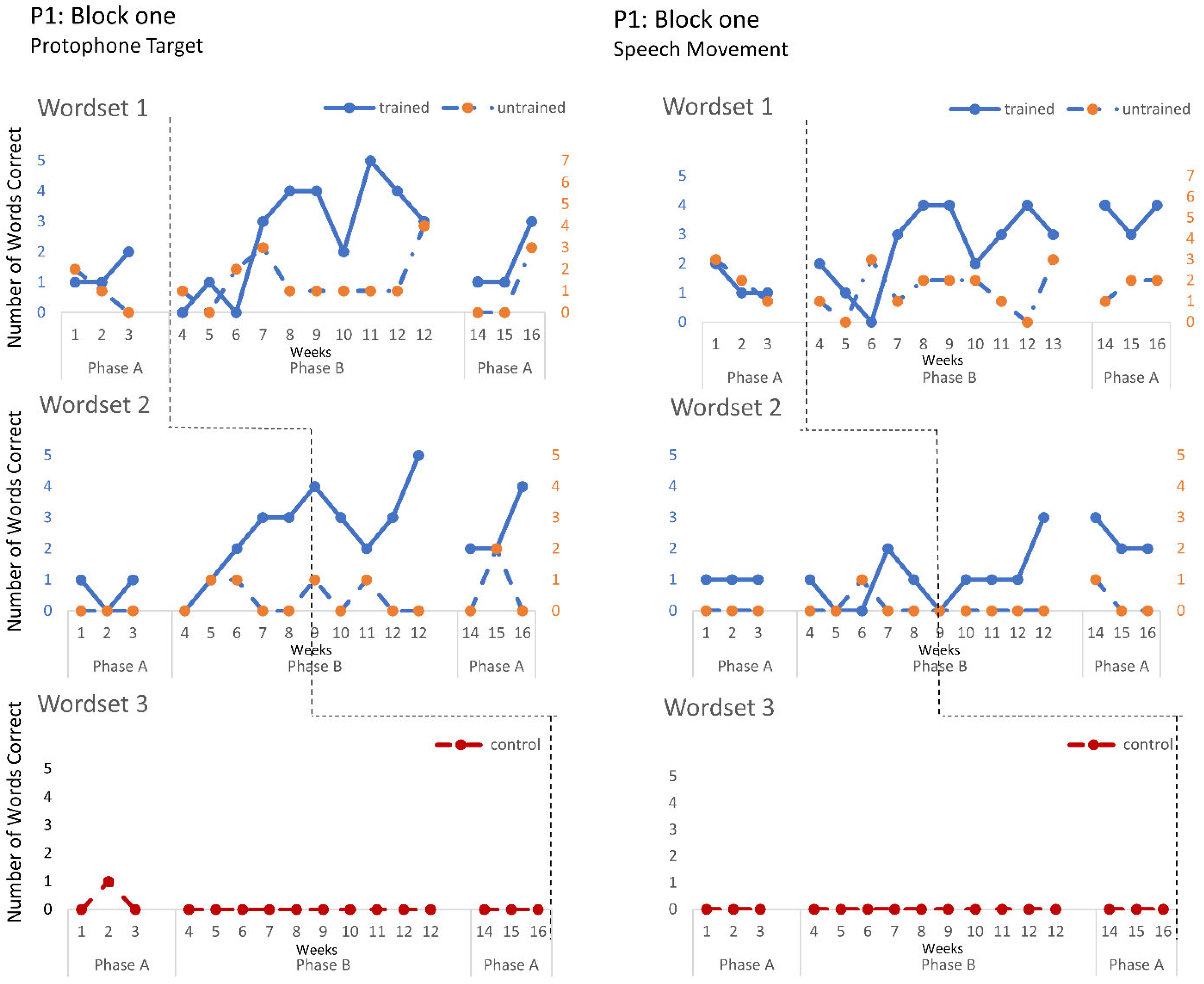
Figure 9 for P3. Each data point represents the number of elicited vocal productions coded as achieved within each word set for protophone targets (in panel A) and speech movement targets (in panel B). The number achieved for trained items is given on the left vertical axis, and the number of achieved untrained items is given on the right, with the maximum value of each scale adjusted according to the total number of items for that word set condition. Visual analysis indicates the initial baselines for each intervention block were relatively stable with low or no variability for all participants. A positive treatment effect, that is, an increase in the number of trained items from word sets 1 and 2 achieving the target priorities compared to pre-intervention baseline counts, was seen for all participants for some intervention blocks. The magnitude of treatment effect is reported in
Table 5 for protophone targets and
Table 6 for speech movement targets. As an overall summary across participants and outcome measures, the mean Tau coefficient effect size for trained items in word set 1 (i.e., items trained throughout the intervention block) was 0.61 (
SD = 0.27, range 0.22–1.0), a large effect size. Of those 15 Tau coefficients, five were statistically significant with large or very large effect size. The mean difference in percent for the word set 1 trained items between the post-intervention and pre-intervention baselines was positive and averaged 37% (
SD = 24.9, range 6.7–75.0). The Tau coefficient also correlated strongly with the mean difference scores (
r = 0.86,
p < 0.001,
n = 15), confirming larger effects during the intervention phase for trained word set 1 items tended to be associated with a higher post-intervention mean (see also
Figure 2,
Figure 3,
Figure 4,
Figure 5,
Figure 6,
Figure 7,
Figure 8 and
Figure 9).
The mean Tau coefficient effect size for trained word set 2 items, also calculated across participants and outcome measures, was 0.51 (SD = 0.36, range −0.1–1.0), a moderate to large effect size, with seven out of 15 coefficients being statistically significant with a large or very large effect size. The pre to post-intervention mean differences in percent averaged 35% (SD = 24.4, range 0.0 to 75) for trained word set 2 items. The correlation between the Tau coefficient and the mean difference for the same items was positive and statistically significant (r = 0.57, p = 0.026, n = 15).
There was some limited evidence of generalisation to untrained items with five out of 30 Tau coefficients, all from either block two or three, being statistically significant with a large or very large effect size. The average mean difference across word set 1 and 2 untrained items was 23% (SD = 25.2, range −6.67–100). No changes were recorded in the control goal for any participant.
P1. In block one, intervention targeted controlled phonation, whilst moving the jaw from closed to open (closant–vocant) and open to closed (vocant–closant) syllable shapes, with target words containing predominantly bilabials. A moderate treatment effect was recorded for the protophone targets and speech movements on trained word set 1. In addition, a large and significant treatment effect was also observed in protophone targets for trained words containing bilabials in word set 2. Block two recorded a moderate treatment effect on trained word set 1 with generalisation to the untrained word set (moderate effect), where intervention targeted the production of protophones requiring open–close (vowel–consonant), close–open (consonant–vowel). Furthermore, a moderate treatment effect was observed on speech movements for the word set 2 trained items, and a significant effect for the untrained word set 2 items, showing the targeted vowels contained rounded and retracted lip movements. Block three recorded the largest treatment effects for protophone targets in word sets 1 and 2 and for speech movement targets in trained word sets 1 for items containing labial-fricatives (e.g., /f/, /v/) and lingual sounds (e.g., /d/, /g/), with large or very large effect sizes. Overall, there was a trend for larger and more consistent effects in block three for P1 compared to block one and two, which indicates a possible cumulative response to intervention.
P2. Treatment effects were observed in the intentional use of vocalisations and target protophones and speech movements across all three intervention blocks. Block one targeted the production of protophone vocalisations with communicative intent, thereby decreasing non-communicative vocalisations. The data for four intervention sessions are missing due to technical failure. Nonetheless, the data show a large treatment effect on word set 2. Furthermore, the child vocalisation count, automatically generated from the LENA DLP, revealed a significant treatment effect, with decreasing vocalisations recorded within the home environment (Tau = −1, z = −2.393, p = 0.017). Block two recorded a moderate treatment effect on speech movement in trained word sets 1 and 2, where the intervention targeted jaw transitions from open-to-closed and closed-to-open; however, performance was variable. These changes in motor-speech control coincided with a large treatment effect in the number of target protophones for word set 1 trained items, with evidence of closant–vocant and vocant–closant productions, not previously sampled with communicative intent. Block three recorded treatment effects consistent with block two (e.g., significant effect for trained items from word set 2 for both protophone and speech movement targets), and showed evidence of generalisation of target protophone production in untrained words (word set 1). Treatment effects were greater for word set 2 than word set 1 for protophone production and speech movement targets, with evidence of CV (i.e., consonant–vowel), VC and CVCV productions, the phonemes /m/, /b/, /d/, /h/ and low vowels (e.g., /a/), for words such as bubble, bye and more.
P3. P3 participated in two intervention blocks. During block one, there was a moderate increase in the production of controlled phonation on single protophones in word set 1, with no controlled phonation evident during baseline. Jaw transitions from closed-to-open and closed-to-open were not produced with communicative intent. These treatment effects were not maintained during post-intervention baseline. In contrast to block one, block two reveals a very large and significant treatment effect on trained word sets 1 and 2, for both protophone and speech movement targets, and large significant effects on word sets 1 and 2 untrained items for speech movement target for CV, VC and CVC words containing bi-labials (/b/, /p/, /m), alveolars (t/d/ and the velar (/g/). Post intervention data show the treatment effects were maintained for word sets 1 and 2.
5. Limitations
There are a number of limitations to consider with this study. The highest level of single-subject research design (SSRD) is a randomised n-of-1 design, which may include random assignment of participant to treatment or order of treatment administration, as well as extended baselines when responses are more variable. This standard, whilst desirable, was not able to be met. At the time of this study, two additional multisite research trials were in process within this clinical population and age group. However, we mitigated risks to internal validity through the minimum of three data points per phase, systematic manipulation and assessment of the dependent variables by more than one assessor, and replication with at least three demonstrations of the experimental effect [
42,
43].
SSRD research requires repeated measures that are standardised, sensitive to change, reliable and valid. Given SSRD has been heralded as a methodology with clinical relevance, outcome measures should also be feasible to administer. The coding of speech probes for this study, however, required phonetic transcription, manual coding of the protophones, and visual-perceptual analysis of speech movements. The analysis was therefore labor intensive, and this potentially limits the clinically feasibility of the intervention.
Furthermore, the outcome measures of this study required the a priori compilation of trained and untrained word sets with equal numbers of items in each word set. However, in response to participant interest and motivation, or the fact that some items did not get trained as intended, some words moved from their assigned word set resulting in a different number of items in the trained and untrained conditions (see
Appendix A). A greater number of items within a condition may result in more opportunities to show improvement. This potential bias in effect size from differences in item numbers when comparing the trained and untrained data should be taken into account. However, we do note that the imbalance in item numbers does not systematically favour either the trained or untrained item conditions across participants.
Finally, whilst parents were provided with a LENA device to record the elicitation of the speech probes once per week during intervention block one, and two times per week during intervention blocks two and three, home practice was not monitored to track cumulative treatment intensity.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}