The Assessment of Immune Fitness



Abstract
:1. Introduction
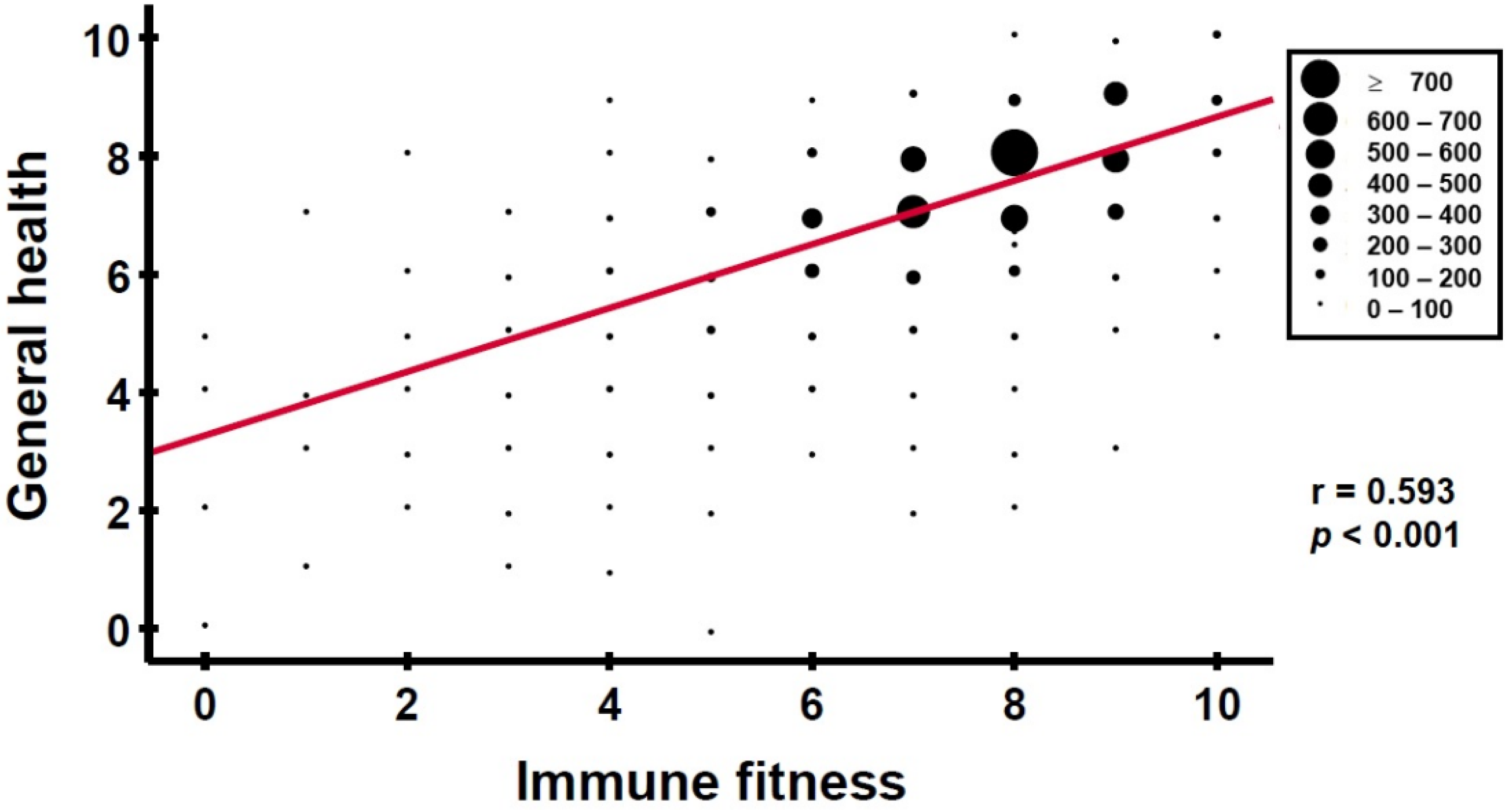
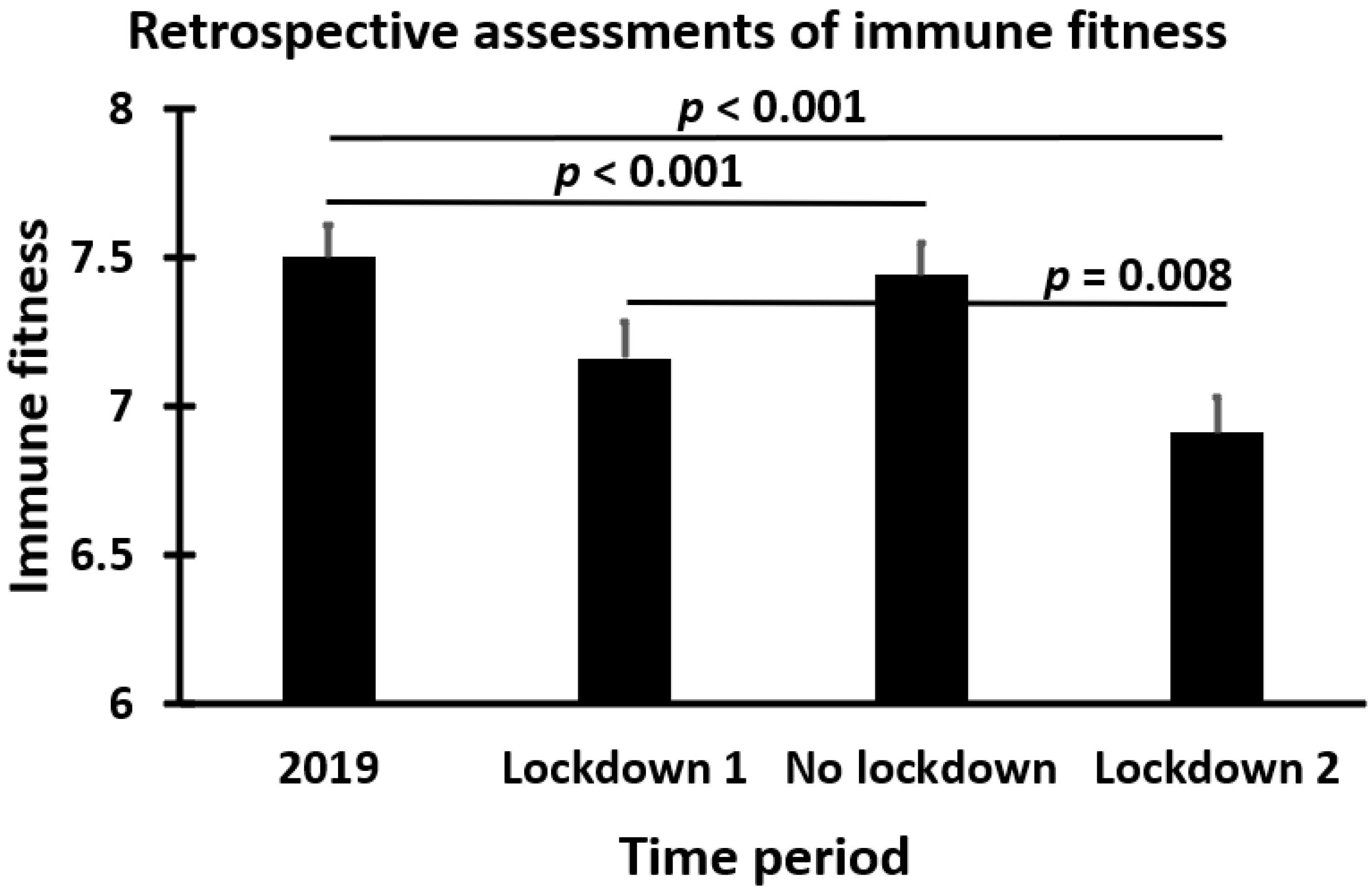
2. Assessment of Immune Fitness
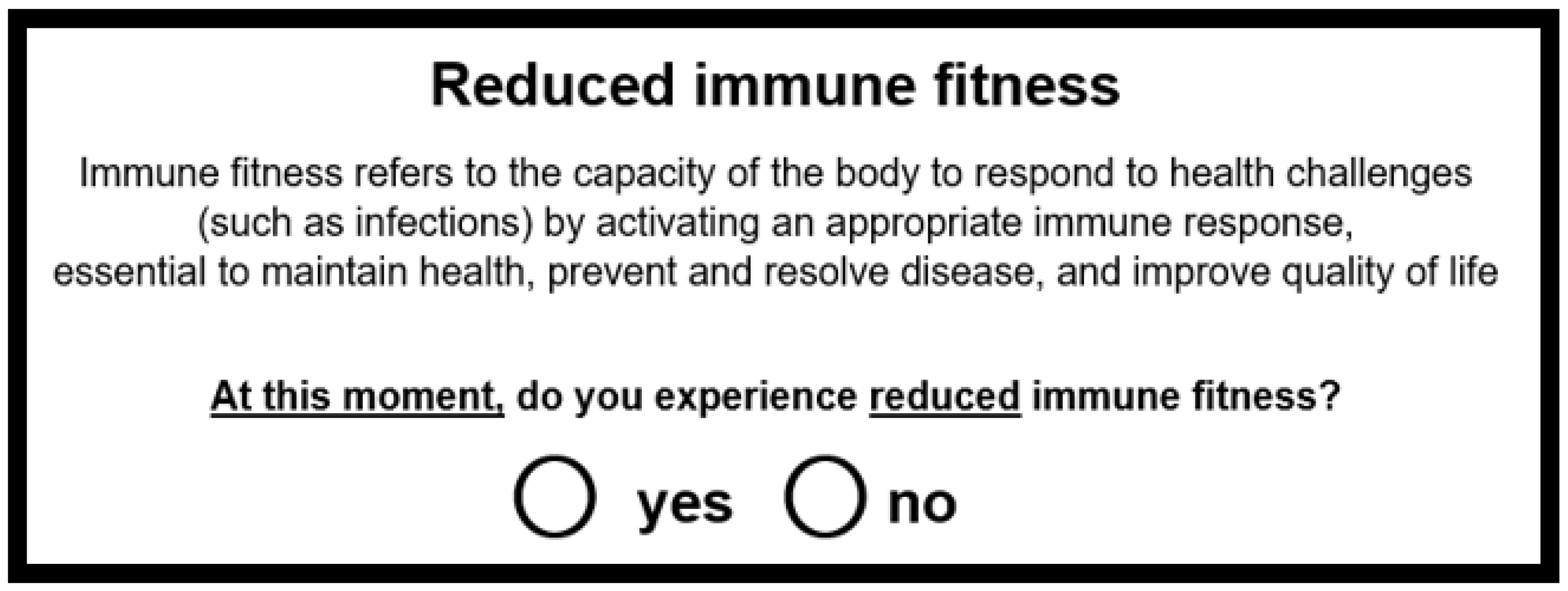
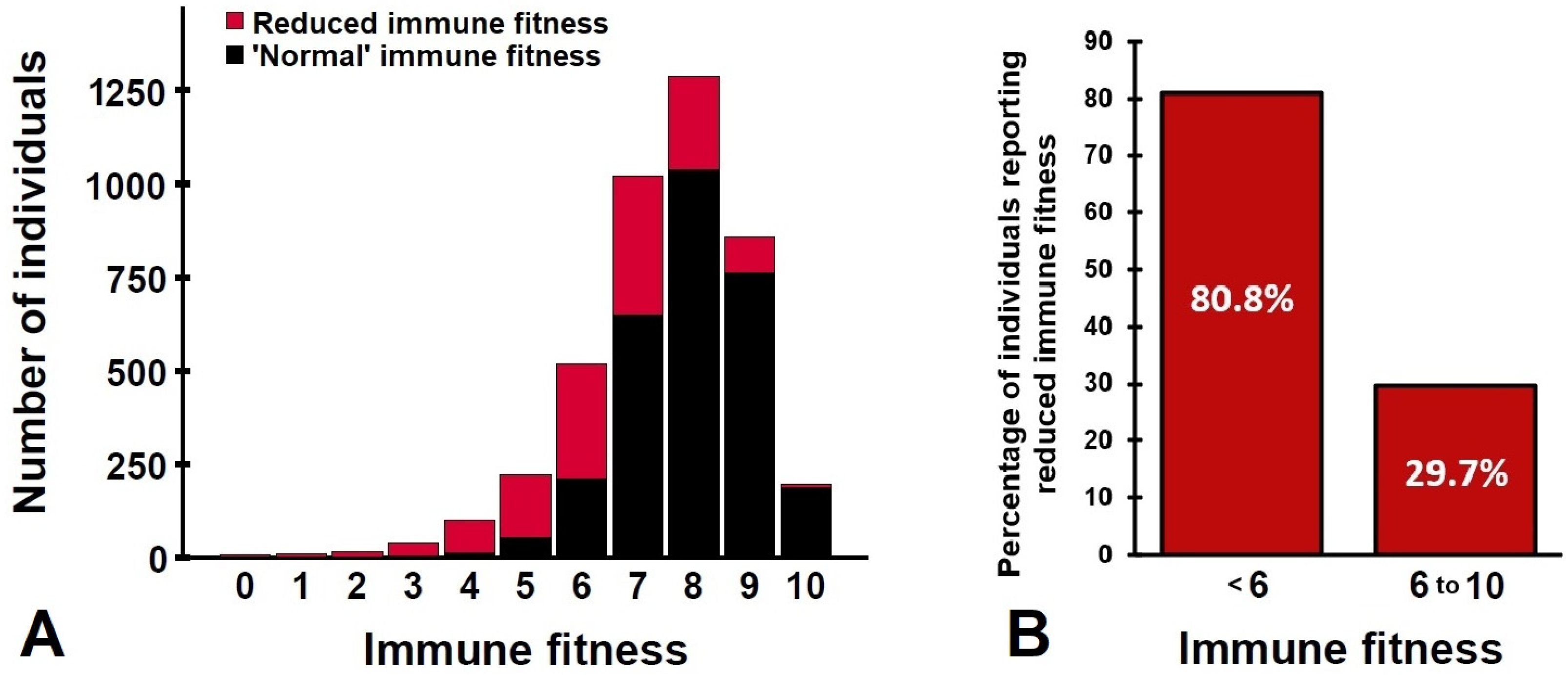
3. Reduced Immune Fitness
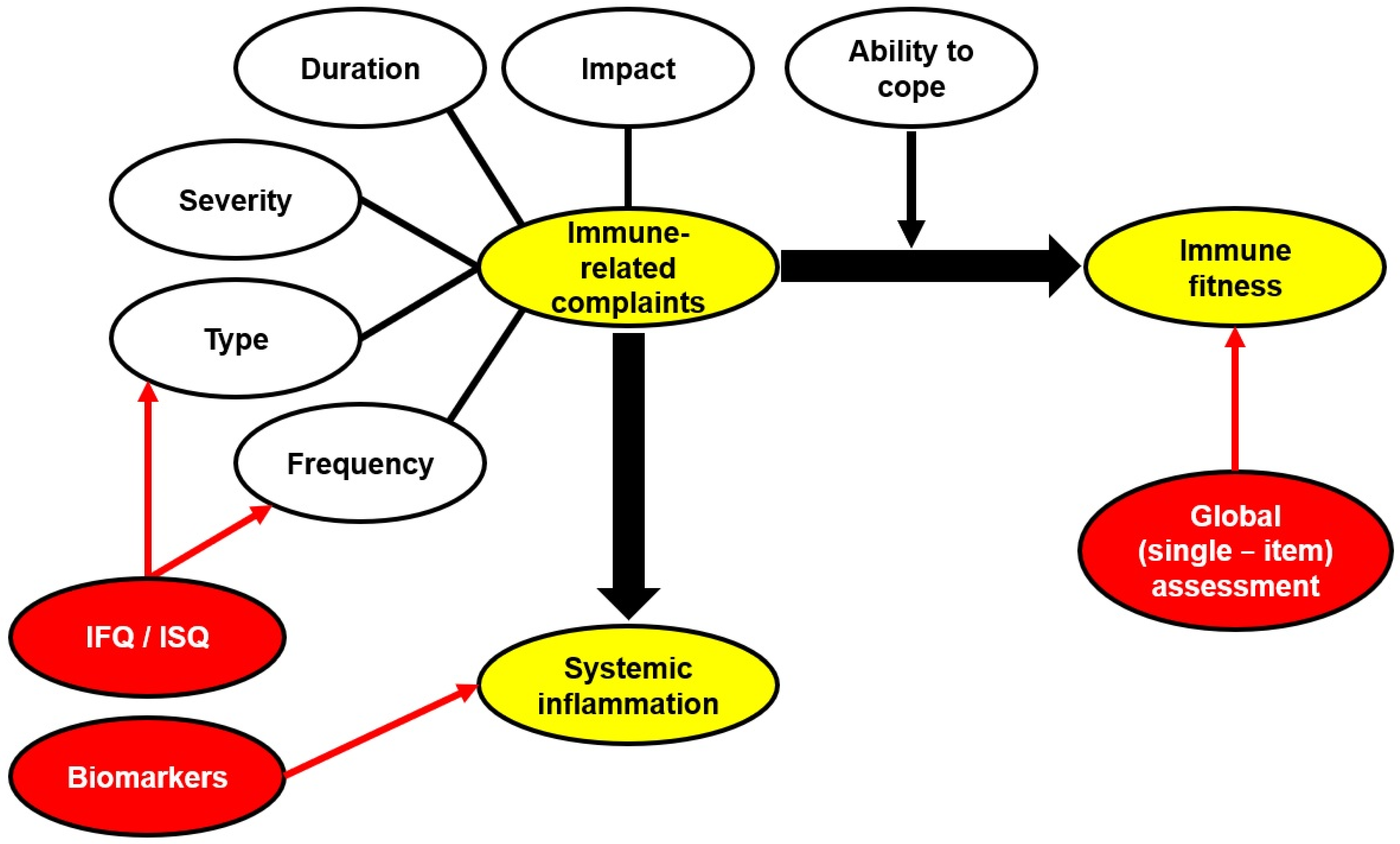
4. Multiple-Item Scales to Assess Immune Functioning: The IFQ and ISQ
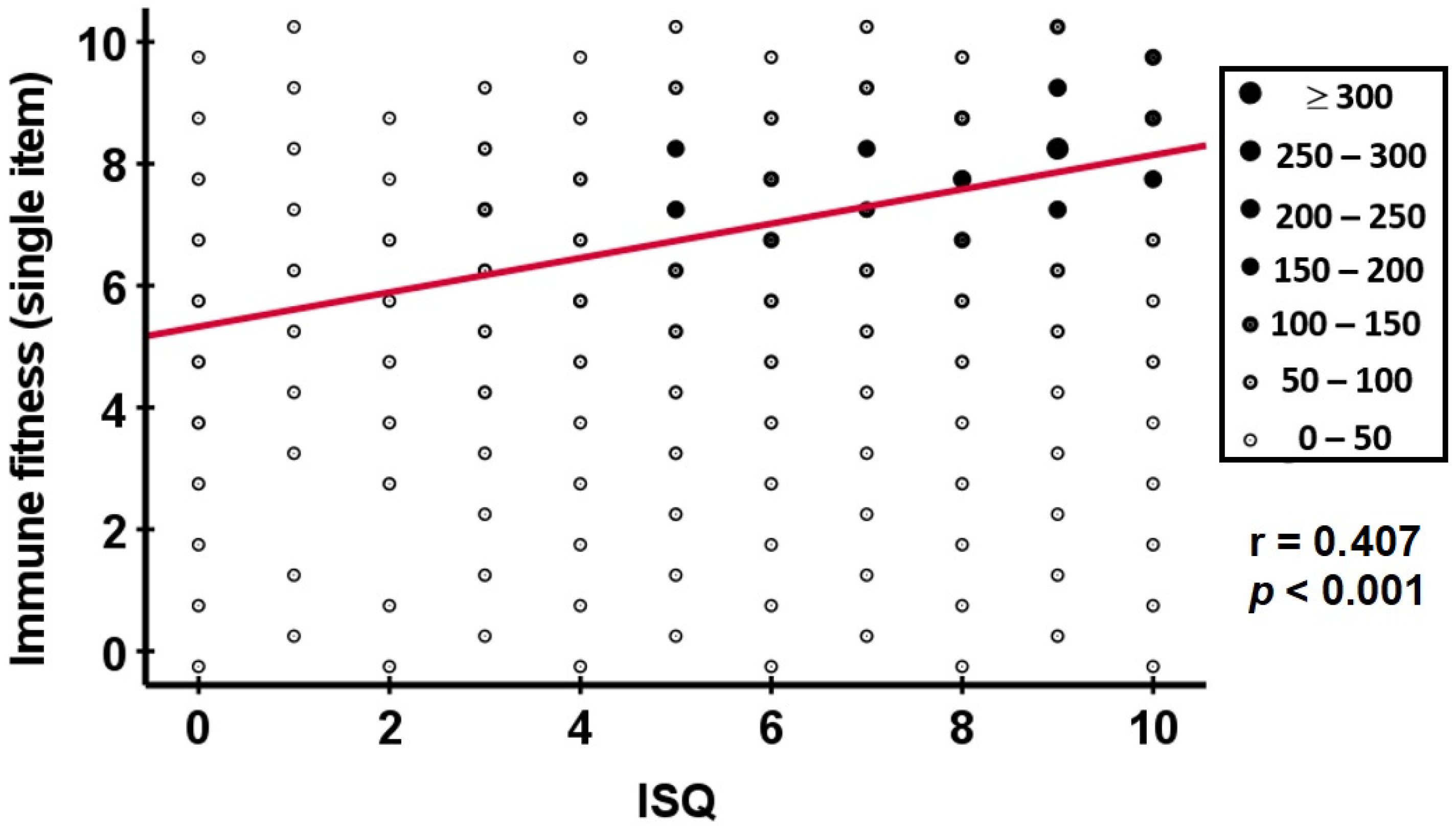
5. Comparison of the Single-Item Assessment of Immune Fitness and the ISQ
6. Biomarkers of Immune Fitness?
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Unwin, N.; Alberti, K.G.M.M. Chronic non-communicable diseases. Ann. Trop. Med. Parasitol. 2006, 100, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Ogoina, D.; Onyemelukwe, G.C. The role of infections in the emergence of noncommunicable diseases (NCDs): Compelling needs for novel strategies in the developing world. J. Infect. Public Health 2009, 2, 14–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 30 March 2022).
- Kiani, P.; Balikji, J.; Kraneveld, A.D.; Garssen, J.; Bruce, G.; Verster, J.C. Pandemic preparedness: The importance of adequate immune fitness. J. Clin. Med. 2022, 11, 2442. [Google Scholar] [CrossRef]
- Hendriksen, P.A.; Garssen, J.; Bijlsma, E.Y.; Engels, F.; Bruce, G.; Verster, J.C. COVID-19 lockdown-related changes in mood, health and academic functioning. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1440–1461. [Google Scholar] [CrossRef]
- Donners, A.A.M.T.; Tromp, M.D.P.; Garssen, J.; Roth, T.; Verster, J.C. Perceived immune status and sleep: A survey among Dutch students. Sleep Disord. 2015, 2015, 721607. [Google Scholar] [CrossRef] [Green Version]
- Otten, L.; De Kruijff, D.; Mackus, M.; Garssen, J.; Verster, J. Attention Deficit Hyperactivity Disorder (ADHD) and the dietary intake of fiber and fats. Eur. Neuropsychopharmacol. 2016, 26, S726. [Google Scholar] [CrossRef]
- Mackus, M.; de Kruijff, D.; Otten, L.S.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. The 2D:4D digit ratio as a biomarker for autism spectrum disorder. Autism Res. Treat. 2017, 2017, 1048302. [Google Scholar] [CrossRef] [Green Version]
- Fernstrand, A.M.; Bury, D.; Garssen, J.; Verster, J.C. Dietary intake of fibers: Differential effects in men and women on general health and perceived immune functioning. Food Nutr. Res. 2017, 61, 1297053. [Google Scholar] [CrossRef] [Green Version]
- Van Schrojenstein Lantman, M.; Otten, L.S.; Mackus, M.; de Kruijff, D.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Huls, H.; Abdulahad, S.; Mackus, M.; Van de Loo, A.J.A.E.; Roehrs, T.; Roth, T.; Verster, J.C. Inclusion and Exclusion Criteria of Clinical Trials for Insomnia. J. Clin. Med. 2018, 7, 206. [Google Scholar] [CrossRef]
- Sulzer, T.A.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Early life exposome pressure on later life immune fitness: A layman’s perspective. Eur. Neuropsychopharmacol. 2019, 29, S204–S205. [Google Scholar] [CrossRef]
- Kiani, P.; Merlo, A.; Saeed, H.M.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.D.; Severeijns, N.R.; Sips, A.S.M.; Scholey, A.; et al. Immune fitness, and the psychosocial and health consequences of the COVID-19 pandemic lockdown in The Netherlands: Methodology and design of the CLOFIT study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199–218. [Google Scholar] [CrossRef] [PubMed]
- Balikji, J.; Hoogbergen, M.M.; Garssen, J.; Verster, J.C. Self-reported impaired wound healing in young adults and their susceptibility to experiencing immune-related complaints. J. Clin. Med. 2022, 11, 980. [Google Scholar] [CrossRef]
- Hendriksen, P.A.; Kiani, P.; Garssen, J.; Bruce, G.; Verster, J.C. Living alone or together during lockdown: Association with mood, immune fitness and experiencing COVID-19 symptoms. Psychol. Res. Behav. Manag. 2021, 14, 1947–1957. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Arnoldy, L.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Scholey, A. The impact of having a holiday or work in Fiji on perceived immune fitness. Tour. Hosp. 2021, 2, 95–112. [Google Scholar] [CrossRef]
- Balikji, S.; Mackus, M.; Brookhuis, K.; Garssen, J.; Kraneveld, A.D.; Roth, T.; Verster, J.C. The association of sleep, perceived immune functioning, and irritable bowel syndrome. J. Clin. Med. 2018, 7, 238. [Google Scholar] [CrossRef] [Green Version]
- Abdulahad, S.; Huls, H.; Balikji, S.; van de Loo, A.J.A.E.; Roth, T.; Verster, J.C. Irritable bowel syndrome, immune fitness and insomnia: Results from an online survey among people with sleep complaints. Sleep Vigil. 2019, 3, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Merlo, A.; Severeijns, N.R.; Benson, S.; Scholey, A.; Garssen, J.; Bruce, G.; Verster, J.C. Mood and changes in alcohol consumption in young adults during COVID-19 lockdown: A model explaining associations with perceived immune fitness and experiencing COVID-19 symptoms. Int. J. Environ. Res. Public Health 2021, 18, 10028. [Google Scholar] [CrossRef]
- Kiani, P.; Mulder, K.E.W.; Balikji, J.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Pandemic preparedness: Maintaining adequate immune fitness by attaining a normal, healthy bodyweight. J. Clin. Med. 2022, 11, 3933. [Google Scholar] [CrossRef]
- Verster, J.C.; Anogeianaki, A.; Kruisselbrink, L.D.; Alford, C.; Stock, A.-K. Relationship of alcohol hangover and physical endurance performance: Walking the Samaria Gorge. J. Clin. Med. 2020, 9, 114. [Google Scholar] [CrossRef]
- Hendriksen, P.A.; Merlo, A.; Garssen, J.; Bijlsma, E.Y.; Engels, F.; Bruce, G.; Verster, J.C. The impact of COVID-19 lockdown on academic functioning and mood: Data from Dutch pharmacy students, PhD candidates and post-docs. Data 2021, 6, 120. [Google Scholar] [CrossRef]
- Reed, P.; Vile, R.; Osborne, L.A.; Romano, M.; Truzoli, R. Problematic internet usage and immune function. PLoS ONE 2015, 10, e0140692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, D.P.; Hillier, V.F. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Mackus, M.; de Kruijff, D.; Otten, L.S.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Differential gender effects in the relationship between perceived immune functioning and autism spectrum disorder scores. Int. J. Environ. Res. Public Health 2017, 14, 409. [Google Scholar] [CrossRef] [Green Version]
- Wilod Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Kraneveld, A.D.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef] [Green Version]
- Borchert, K. User Manual: Immune Status Questionnaire ISQ. Millisecond Software. 2022. Available online: https://www.millisecond.com/download/library/v6/isq/isq.manual (accessed on 6 October 2022).
- Alghamdi, B.S.; Alatawi, Y.; Alshehri, F.S.; Tayeb, H.O.; Tarazi, F.I. Relationship Between Public Mental Health and Immune Status During the COVID-19 Pandemic: Cross-Sectional Data from Saudi Arabia. Risk Manag. Healthc Policy 2021, 14, 1439–1447. [Google Scholar] [CrossRef]
- Nesari, T.; Kadam, S.; Vyas, M.; Huddar, V.G.; Prajapati, P.K.; Rajagopala, M.; More, A.; Rajagopala, S.K.; Bhatted, S.K.; Yadav, R.K.; et al. AYURAKSHA, a prophylactic Ayurvedic immunity boosting kit reducing positivity percentage of IgG COVID-19 among frontline Indian Delhi police personnel: A non-randomized controlled intervention trial. Front. Public Health 2022, 10, 920126. [Google Scholar] [CrossRef]
- Koyun, A.H.; Hendriksen, P.A.; Kiani, P.; Merlo, A.; Balikji, J.; Stock, A.-K.; Verster, J.C. COVID-19 lockdown effects on mood, alcohol consumption, academic functioning, and perceived immune fitness: Data from young adults in Germany. Data 2022, 7, 125. [Google Scholar] [CrossRef]
- Tarantino, V.; Tasca, I.; Giannetto, N.; Mangano, G.R.; Turriziani, P.; Oliveri, M. Impact of Perceived Stress and Immune Status on Decision-Making Abilities during COVID-19 Pandemic Lockdown. Behav. Sci. 2021, 11, 167. [Google Scholar] [CrossRef]
- Maulana, G.F.; Arovah, N.I. The psychometric evaluation of the immune status questionnaire in Indonesia. East. J. Med. 2022, 27, 380–388. [Google Scholar] [CrossRef]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J.C. The impact of raw fermented milk products on perceived health and mood among Dutch adults. Nutr. Food Sci. 2019, 49, 1195–1206. [Google Scholar] [CrossRef]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J.C. Effect of raw milk consumption on perceived health, mood and immune functioning among US adults with a poor and normal health: A retrospective questionnaire based study. Complement. Ther. Med. 2019, 47, 102196. [Google Scholar] [CrossRef] [PubMed]
- Van Oostrom, E.C.; Mulder, K.E.W.; Verheul, M.C.E.; Hendriksen, P.A.; Thijssen, S.; Kraneveld, A.D.; Vlieg-Boerstra, B.; Garssen, J.; Verster, J.C. A healthier diet is associated with greater immune fitness. PharmaNutrition 2022, 21, 100306. [Google Scholar] [CrossRef]
- US FDA. Guidance for Industry. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims. December 2009. Available online: https://www.fda.gov/media/77832/download (accessed on 16 February 2020).
- Verster, J.C.; Sandalova, E.; Garssen, J.; Bruce, G. The use of single-item ratings versus traditional multiple-item questionnaires to assess mood and health. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Becht, N.N.; Hoepel, S.J.W.; Garssen, J.; Verster, J.C. Perceived immune fitness, depression, and dietary zinc intake. Neurosci. Appl. 2022, in press. [CrossRef]
- Kananen, L.; Enroth, L.; Raitanen, J.; Jylhävä, J.; Bürkle, A.; Moreno-Villanueva, M.; Bernhardt, J.; Toussaint, O.; Grubeck-Loebenstein, B.; Malavolta, M.; et al. Self-rated health in individuals with and without disease is associated with multiple biomarkers representing multiple biological domains. Sci. Rep. 2011, 11, 6139. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Historical review of cytokines. Eur. J. Immunol. 2011, 37 (Suppl. 1), S34–S45. [Google Scholar] [CrossRef] [Green Version]
- Petrie, K.J.; Booth, R.J.; Elder, H.; Cameron, L.D. Psychological influences on the perception of immune function. Psychol. Med. 1999, 29, 391–397. [Google Scholar] [CrossRef]
- Liang, J.; Shaw, B.A.; Krause, N.; Bennett, J.M.; Kobayashi, E.; Fukaya, T.; Sugihara, Y. How Does Self-Assessed Health Change With Age? A Study of Older Adults in Japan. J. Gerontol. Ser. B 2005, 60, S224–S232. [Google Scholar] [CrossRef] [Green Version]
- Bowling, A. Do older and younger people differ in their reported well-being? A national survey of adults in Britain. Fam. Pract. 2011, 28, 145–155. [Google Scholar] [CrossRef]
- Briscoe, M.E. Sex differences in perception of illness and expressed life satisfaction. Psychol. Med. 1978, 8, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Sood, R.; Jenkins, S.M.; Sood, A.; Clark, M.M. Gender Differences in Self-perception of Health at a Wellness Center. Am. J. Health Behav. 2019, 43, 1129. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Different Aspects of Immune-Related Complaints | Immune Fitness (Single-Item) | Reduced Immune Fitness (Yes/No) | IFQ/ISQ | |
|---|---|---|---|---|
| 1 | Type and number | √ | √ | √ |
| 2 | Frequency | √ | √ | √ |
| 3 | Severity | √ | √ | X |
| 4 | Duration | √ | √ | X |
| 5 | Impact | √ | √ | X |
| 6 | Ability to cope | √ | √ | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verster, J.C.; Kraneveld, A.D.; Garssen, J. The Assessment of Immune Fitness. J. Clin. Med. 2023, 12, 22. https://doi.org/10.3390/jcm12010022
Verster JC, Kraneveld AD, Garssen J. The Assessment of Immune Fitness. Journal of Clinical Medicine. 2023; 12(1):22. https://doi.org/10.3390/jcm12010022
Chicago/Turabian StyleVerster, Joris C., Aletta D. Kraneveld, and Johan Garssen. 2023. "The Assessment of Immune Fitness" Journal of Clinical Medicine 12, no. 1: 22. https://doi.org/10.3390/jcm12010022