
An Investigation of the Association between 3D Spinal Alignment and Fibromyalgia
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
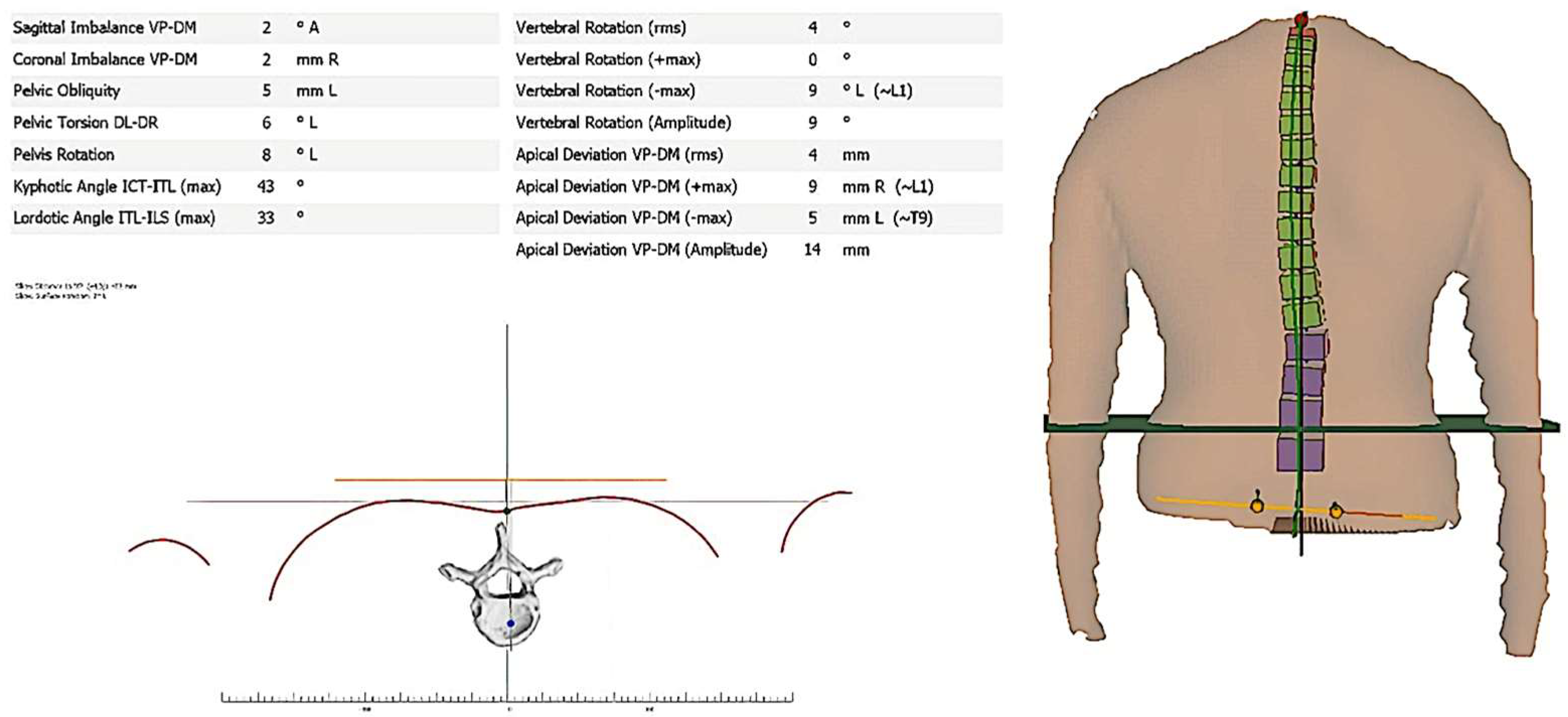
2.1. 3D Posture Measurement Using a Formetric System
2.2. Kyphotic Angle
2.3. Lordotic Angle
2.4. Sagittal Imbalance or Trunk Inclination
2.5. Coronal Imbalance
2.6. Vertebral Rotation
2.7. Fibromyalgia Impact Questionnaire (FIQ)
2.8. Sample Size Determination
2.9. Data Analysis
3. Results
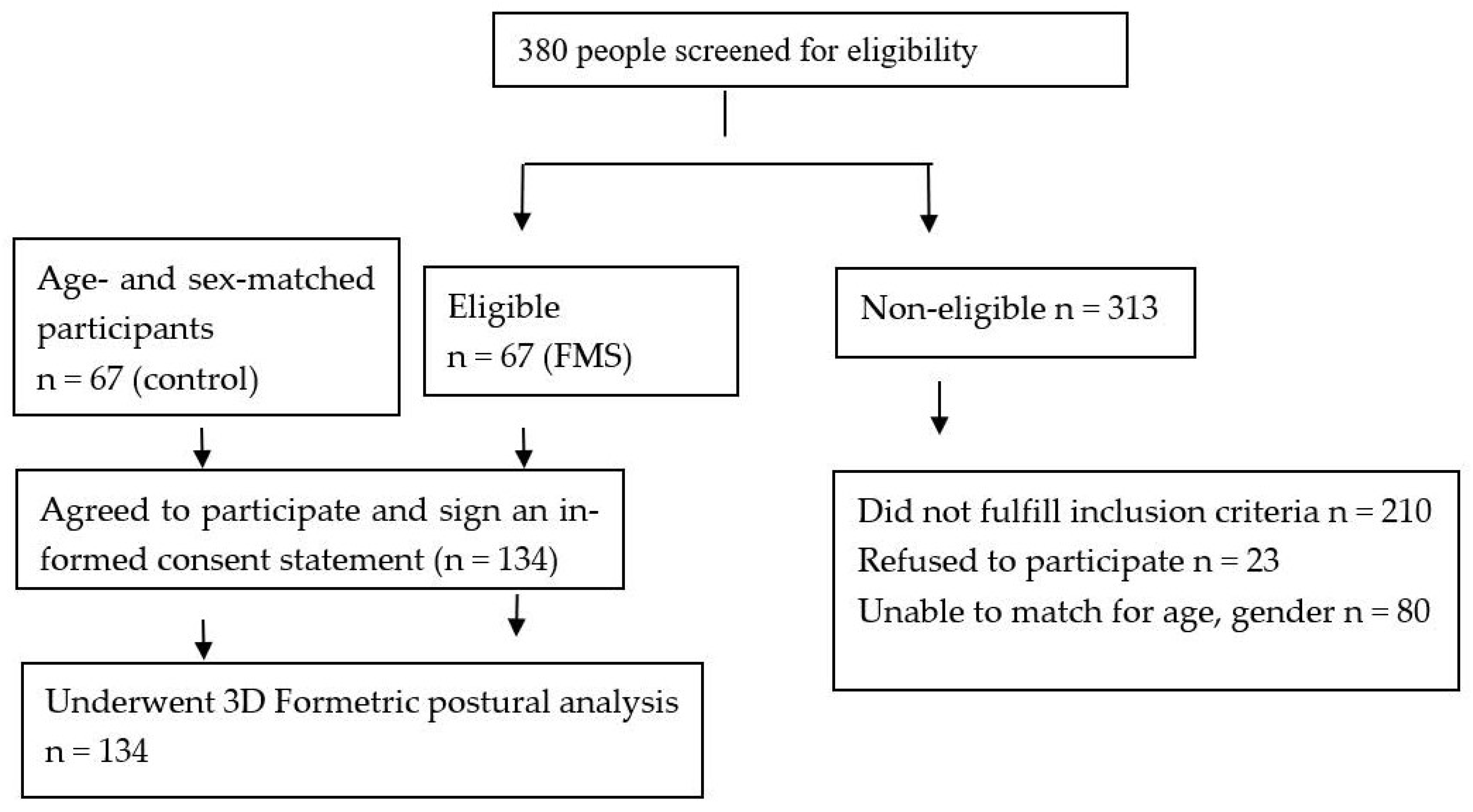
3.1. Sample Characteristics
3.2. Formetric Postural Variables between Group Differences
3.3. Binary Logistic Regressions
3.4. Odds Ratios between Having FMS and Posture Variables
4. Discussion
4.1. Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3D | Three-dimensional |
| FMS | Fibromyalgia syndrome |
| ICT-ITL | Cervicothoracic transition point (ICT)-thoracolumbar transition point (ITL) max |
| ITL-ILS | Thoracic-lumbar inflection point (ITL)-lumbar-sacral inflection point (ILS) max |
| RMS | Root mean square |
References
- Apkarian, A.V. Definitions of Nociception, Pain, and Chronic Pain with Implications Regarding Science and Society. Neurosci. Lett. 2019, 702, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia Pathogenesis and Treatment Options Update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Jahan, F.; Nanji, K.; Qidwai, W.; Qasim, R. Oman Medical Specialty Board Fibromyalgia Syndrome: An Overview of Pathophysiology, Diagnosis and Management. Oman Med. J. 2012, 27, 192. [Google Scholar] [CrossRef] [PubMed]
- Cuyul-Vásquez, I.; Araya-Quintanilla, F.; Gutiérrez-Espinoza, H. Comment on Siracusa et Al. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar]
- Makofsky, B.H.W.; Goldstein, L.B. The Role of Body Posture in Musculoskeletal Pain Syndromes. Pract. Pain Manag. 2011, 3, 31. [Google Scholar]
- Lennon, J.; Shealy, N.; Cady, R.; Matta, W.; Cox, R.S.W. Postural and Respiratory Modulation of Autonomic Function, Pain and Health. Am. J. Pain Manag. 1994, 4, 36–39. [Google Scholar]
- Cameron, M.H.; Monroe, L.G. Physical Rehabilitation: Evidence-Based Examination, Evaluation, and Intervention; Saunders Elsevier: St Louis, MO, USA, 2007; p. 953. [Google Scholar]
- Raine, S.; Twomey, L. Attributes and qualities of human posture and their relationship to dysfunction or musculoskeletal pain. Crit. Rev. Phys. Rehabil. Med. 1994, 6, 409–437. [Google Scholar]
- Fernandez-de-las-Penas, C.; Alonso-Blanco, C.; Cuadrado, M.L.; Gerwin, R.D.; Pareja, J.A. Trigger Points in the Suboccipital Muscles and Forward Head Posture in Tension-Type Headache. Headache J. Head Face Pain 2006, 46, 454–460. [Google Scholar] [CrossRef]
- Moustafa, I.M.; Shousha, T.M.; Harrison, D.E. An investigation of 3D spinal alignment in cervicogenic headache. Musculoskelet. Sci. Pract. 2021, 51, 102284. [Google Scholar] [CrossRef] [PubMed]
- Evcik, D.; Aksoy, O. Relationship Between Head Posture and Temporomandibular Dysfunction Syndrome. J. Musculoskelet. Pain 2010, 12, 19–24. [Google Scholar] [CrossRef]
- Gonzalez, H.E.; Manns, A. Forward Head Posture: Its Structural and Functional Influence on the Stomatognathic System, a Conceptual Study. Cranio 1996, 14, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.F.; Domenech, M.A.; Fischer, J.R. Usefulness of Posture Training for Patients with Temporomandibular Disorders. J. Am. Dent. Assoc. 2000, 131, 202–210. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Cook, T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys. Ther. 2000, 80, 276–291. [Google Scholar] [CrossRef] [Green Version]
- Bullock, M.P.; Foster, N.E.; Wright, C.C. Shoulder Impingement: The Effect of Sitting Posture on Shoulder Pain and Range of Motion. Man. Ther. 2005, 10, 28–37. [Google Scholar] [CrossRef]
- McMaster, M.J.; Glasby, M.A.; Singh, H.; Cunningham, S. Lung Function in Congenital Kyphosis and Kyphoscoliosis. J. Spinal Disord. Tech. 2007, 20, 203–208. [Google Scholar] [CrossRef]
- Kapreli, E.; Vourazanis, E.; Billis, E.; Oldham, J.A.; Strimpakos, N. Respiratory Dysfunction in Chronic Neck Pain Patients. A Pilot Study. Cephalalgia 2009, 29, 701–710. [Google Scholar] [CrossRef]
- Christie, H.J.; Kumar, S.; Warren, S.A. Postural Aberrations in Low Back Pain. Arch. Phys. Med. Rehabil. 1995, 76, 218–224. [Google Scholar] [CrossRef]
- Cacciatore, T.W.; Horak, F.B.; Henry, S. Improvement in Automatic Postural Coordination Following Alexander Technique Lessons in a Person with Low Back Pain. Phys. Ther. 2005, 85, 565. [Google Scholar] [CrossRef] [Green Version]
- Nemmers, T. The Influence of the forward Head Posture on Balance, Fall Self-Efficacy, and Physical Activity Level in Community-Dwelling Women Age 60 and Older; and the Relationship of These Variables to Self-Reported Fall History. Ph.D. Thesis, Oklahoma State University, Stillwater, OK, USA, 2006. Available online: https://hdl.handle.net/11244/7521 (accessed on 29 October 2022).
- Hiemeyer, K.; Lutz, R.; Menninger, H. Dependence of tender points upon posture: A key to the understanding of fibromyalgia syndrome. J. Man. Med. 1990, 5, 169–174. [Google Scholar]
- Keller, T.S.; Harrison, D.E.; Colloca, C.J.; Harrison, D.D.; Janik, T.J. Prediction of Osteoporotic Spinal Deformity. Spine 2003, 28, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Tabard-Fougère, A.; Bonnefoy-Mazure, A.; Hanquinet, S.; Lascombes, P.; Armand, S.; Dayer, R. Validity and Reliability of Spine Rasterstereography in Patients with Adolescent Idiopathic Scoliosis. Spine 2017, 42, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Krott, N.L.; Wild, M.; Betsch, M. Meta-Analysis of the Validity and Reliability of Rasterstereographic Measurements of Spinal Posture. Eur. Spine J. 2020, 29, 2392–2401. [Google Scholar] [CrossRef] [PubMed]
- Frerich, J.M.; Hertzler, K.; Knott, P.; Mardjetko, S. Comparison of Radiographic and Surface Topography Measurements in Adolescents with Idiopathic Scoliosis. Open Orthop. J. 2012, 6, 261–265. [Google Scholar] [CrossRef]
- Harrison, D.D.; Harrison, D.E.; Janik, T.J.; Cailliet, R.; Haas, J. Do alterations in vertebral and disc dimensions affect an elliptical model of thoracic kyphosis? Spine 2003, 28, 463–469. [Google Scholar] [CrossRef] [PubMed]
- El-Naby, M.A.; Hefny, M.A.; Fahim, A.E.; Awadalla, M.A. Validation of an adapted arabic version of fibromyalgia syndrome impact questionnaire. Rheumatol. Int. 2013, 33, 2561–2567. [Google Scholar] [CrossRef]
- Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Espí-López, G.V.; Cortés-Amador, S.; Pascual, E.; Serra-Añó, P. Impaired Trunk Posture in Women with Fibromyalgia. Spine 2018, 43, 1536–1542. [Google Scholar] [CrossRef]
- Sempere-Rubio, N.; López-Pascual, J.; Aguilar-Rodríguez, M.; Cortés-Amador, S.; Espí-López, G.; Villarrasa-Sapiña, I.; Serra-Añó, P. Characterization of Postural Control Impairment in Women with Fibromyalgia. PLoS ONE 2018, 13, e0196575. [Google Scholar] [CrossRef] [Green Version]
- Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Inglés, M.; Izquierdo-Alventosa, R.; Serra-Añó, P. Physical Condition Factors That Predict a Better Quality of Life in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2019, 16, 3173. [Google Scholar] [CrossRef] [Green Version]
- Toprak Celenay, S.; Mete, O.; Coban, O.; Oskay, D.; Erten, S. Trunk Position Sense, Postural Stability, and Spine Posture in Fibromyalgia. Rheumatol. Int. 2019, 39, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Czaprowski, D.; Stoliński, L.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-Structural Misalignments of Body Posture in the Sagittal Plane. Scoliosis Spinal Disord. 2018, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.D.; King, L.A.; Mist, S.D.; Bennett, R.M.; Horak, F.B. Postural Control Deficits in People with Fibromyalgia: A Pilot Study. Arthritis Res. Ther. 2011, 13, R127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.D.; Horak, F.B.; Winters-Stone, K.; Irvine, J.M.; Bennett, R.M. Fibromyalgia Is Associated with Impaired Balance and Falls. J. Clin. Rheumatol. 2009, 15, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Moustafa, I.M.; Diab, A.A. The Addition of Upper Cervical Manipulative Therapy in the Treatment of Patients with Fibromyalgia: A Randomized Controlled Trial. Rheumatol. Int. 2015, 35, 1163–1174. [Google Scholar] [CrossRef]
- Müller, A.; Hartmann, M.; Eich, W. Health Care Utilization in Patients with Fibromyalgia Syndrome (FMS). Schmerz 2000, 14, 77–83. [Google Scholar] [CrossRef]
- Cramer, H.; Mehling, W.E.; Saha, F.J.; Dobos, G.; Lauche, R. Postural Awareness and Its Relation to Pain: Validation of an Innovative Instrument Measuring Awareness of Body Posture in Patients with Chronic Pain. BMC Musculoskelet. Disord. 2018, 19, 109. [Google Scholar] [CrossRef] [Green Version]
- Mannerkorpi, K.; Ahlmén, M.; Ekdahl, C. Six- and 24-Month Follow-up of Pool Exercise Therapy and Education for Patients with Fibromyalgia. Scand. J. Rheumatol. 2002, 31, 306–310. [Google Scholar] [CrossRef]
- Imagama, S.; Hasegawa, Y.; Matsuyama, Y.; Sakai, Y.; Ito, Z.; Hamajima, N.; Ishiguro, N. Influence of sagittal balance and physical ability associated with exercise on quality of life in middle-aged and elderly people. Arch. Osteoporos. 2011, 6, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Simons, D.G.; Travell, J.G.; Simons, L.S. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual, 2nd ed.; Hardcover; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1998; p. 1056. [Google Scholar]
- Hiemeyer, K.; Lutz, R.; Menninger, H. Generalisiertes Auftreten von Schmerzhaften Druckpunkten an Sehnen Und Muskeln Beim Habituellen Rundräcken Ein Beitrag Zur Diskussion Um Das Fibromyalgiesyndrom (FMS). Aktuelle Rheumatol. 1989, 14, 193–201. [Google Scholar] [CrossRef]
- Moustafa, I.M. Does improvement towards a normal cerivcal sagittal configuration aid in the management of fibromyalgia syndrome. A randomized controlled trial. Bull. Fac. Ph. Ther. Cairo Univers. 2013, 18, 29–41. [Google Scholar]
- Veldhuizen, A.G.; Wever, D.J.; Webb, P.J. The Aetiology of Idiopathic Scoliosis: Biomechanical and Neuromuscular Factors. Eur. Spine J. 2000, 9, 178–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigo, M.; Quera-Salvá, G.; Villagrasa, M. Sagittal Configuration of the Spine in Girls with Idiopathic Scoliosis: Progressing Rather than Initiating Factor. Stud. Health Technol. Inform. 2006, 123, 90–94. [Google Scholar] [PubMed]
- De Jonge, T.; Dubousset, J.F.; Illés, T. Sagittal Plane Correction in Idiopathic Scoliosis. Spine 2002, 27, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Dobosiewicz, K.; Durmala, J.; Jendrzejek, H.; Czernicki, K. Influence of Method of Asymmetric Trunk Mobilization on Shaping of a Physiological Thoracic Kyphosis in Children and Youth Suffering from Progressive Idiopathic Scoliosis. Stud. Health Technol. Inform. 2002, 91, 348–351. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Fibromyalgia Group (n = 67) | Control Group (n = 67) |
|---|---|---|
| Age (years) | 46.4 ± 9 | 46.5 ± 9.1 |
| Weight (kg) | 75 ± 9 | 80 ± 10 |
| Gender (%) | ||
| Male | 12 | 12 |
| Female | 55 | 55 |
| Body mass index mean (SD), Kg/m2 | ||
| Graduation | ||
| Primary school | 5 (7.5%) | 2 (3%) |
| Secondary school | 10 (14.9%) | 8 (11.9%) |
| Advanced technical colleague certificate | 10 (14.9%) | 15 (22.4%) |
| University diploma | 32 (47.8%) | 30 (44.8%) |
| Others | 10 (14.9%) | 12 (17.9%) |
| Marital status (%) | ||
| Single | 5 (7.5%) | 4 (6%) |
| Married | 55 (82.1%) | 57 (85%) |
| Separated, divorced, or widowed | 7 (10.4%) | 6 (9%) |
| Pain duration | ||
| 1–5 y | 20 (29.9%) | Asymptomatic |
| >5 y | 47 (70.1%) | Asymptomatic |
| 3D Formetric Measurement | Mean | ±SD | SEM | Cohen’s d | 95% CI | p-Value | |
|---|---|---|---|---|---|---|---|
| Kyphotic angle ICT-ITL (max) (deg.) | FMS | 74.1 | 4.75 | 0.58 | 6.8 | [14.3–19.04] | <0.001 |
| Control | 57.4 | 8.41 | 1.02 | ||||
| Lordotic angle ITL-ILS (max) (deg.) | FMS | 45.1 | 5.71 | 0.69 | 4.3 | [1.9–4.9] | <0.001 |
| Control | 41.5 | 2.46 | 0.30 | ||||
| Sagittal imbalance (mm) | FMS | 9.53 | 2.77 | 0.33 | 2.3 | [4.1–5.7] | <0.001 |
| Control | 4.5 | 1.89 | 0.23 | ||||
| Coronal imbalance (mm) | FMS | 8.04 | 3.19 | 0.39 | 2.4 | [3.6–5.6] | <0.001 |
| Control | 3.22 | 1.37 | 0.16 | ||||
| vertebral rotation (rms) (deg.) | FMS | 9.5 | 1.86 | 0.22 | 1.8 | [3.5–4.7] | <0.001 |
| Control | 5.3 | 1.75 | 0.21 |
| Variables in the Equation | ||||||||
|---|---|---|---|---|---|---|---|---|
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% CI for EXP(B) | ||
| Lower | Upper | |||||||
| Sagittal imbalance (mm) | 0.437 | 0.236 | 3.409 | 1 | 0.005 | 1.547 | 0.973 | 2.459 |
| vertebral rotation (rms) (degrees) | 2.069 | 0.851 | 5.914 | 1 | 0.015 | 7.919 | 1.494 | 41.970 |
| Kyphotic ICT−ITL (max) (degrees) | 0.569 | 0.275 | 4.273 | 1 | 0.039 | 1.766 | 1.030 | 3.029 |
| Coronal imbalance (mm) | −0.188 | 0.313 | 0.360 | 1 | 0.549 | 0.829 | 0.449 | 1.530 |
| Lordotic angle (degrees) | 0.472 | 0.326 | 2.105 | 1 | 0.147 | 1.604 | 0.847 | 3.035 |
| Constant | −52.309 | 21.782 | 5.767 | 1 | 0.016 | 0.000 | ||
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% Confidence Interval for B | |||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | ||||
| 1 | Constant | −2.043 | 0.214 | −9.562 | <0.001 | −2.466 | −1.620 | |
| Kyphotic ICT−ITL (max) (deg.) | 0.021 | 0.003 | 0.459 | 8.462 | <0.001 | 0.016 | 0.026 | |
| sagittal imbalance (mm) | 0.024 | 0.009 | 0.166 | 2.739 | 0.005 | 0.007 | 0.042 | |
| vertebral rotation (deg.) | 0.078 | 0.011 | 0.430 | 7.197 | <0.001 | 0.057 | 0.099 | |
| Lordotic angle (deg.) | 0.010 | 0.004 | 0.092 | 2.206 | 0.029 | 0.001 | 0.019 | |
| Coronal imbalance (mm) | −0.007 | 0.010 | −0.046 | −0.688 | 0.493 | −0.026 | 0.013 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahbouch, A.; Moustafa, I.M.; Shousha, T.; Arumugam, A.; Oakley, P.; Harrison, D.E. An Investigation of the Association between 3D Spinal Alignment and Fibromyalgia. J. Clin. Med. 2023, 12, 218. https://doi.org/10.3390/jcm12010218
Ahbouch A, Moustafa IM, Shousha T, Arumugam A, Oakley P, Harrison DE. An Investigation of the Association between 3D Spinal Alignment and Fibromyalgia. Journal of Clinical Medicine. 2023; 12(1):218. https://doi.org/10.3390/jcm12010218
Chicago/Turabian StyleAhbouch, Amal, Ibrahim M. Moustafa, Tamer Shousha, Ashokan Arumugam, Paul Oakley, and Deed E. Harrison. 2023. "An Investigation of the Association between 3D Spinal Alignment and Fibromyalgia" Journal of Clinical Medicine 12, no. 1: 218. https://doi.org/10.3390/jcm12010218