
Can the Norton Scale Score Be Used as an Adjunct Tool for Implantable Defibrillator Patient Selection? A Retrospective Single-Center Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Cohort Population
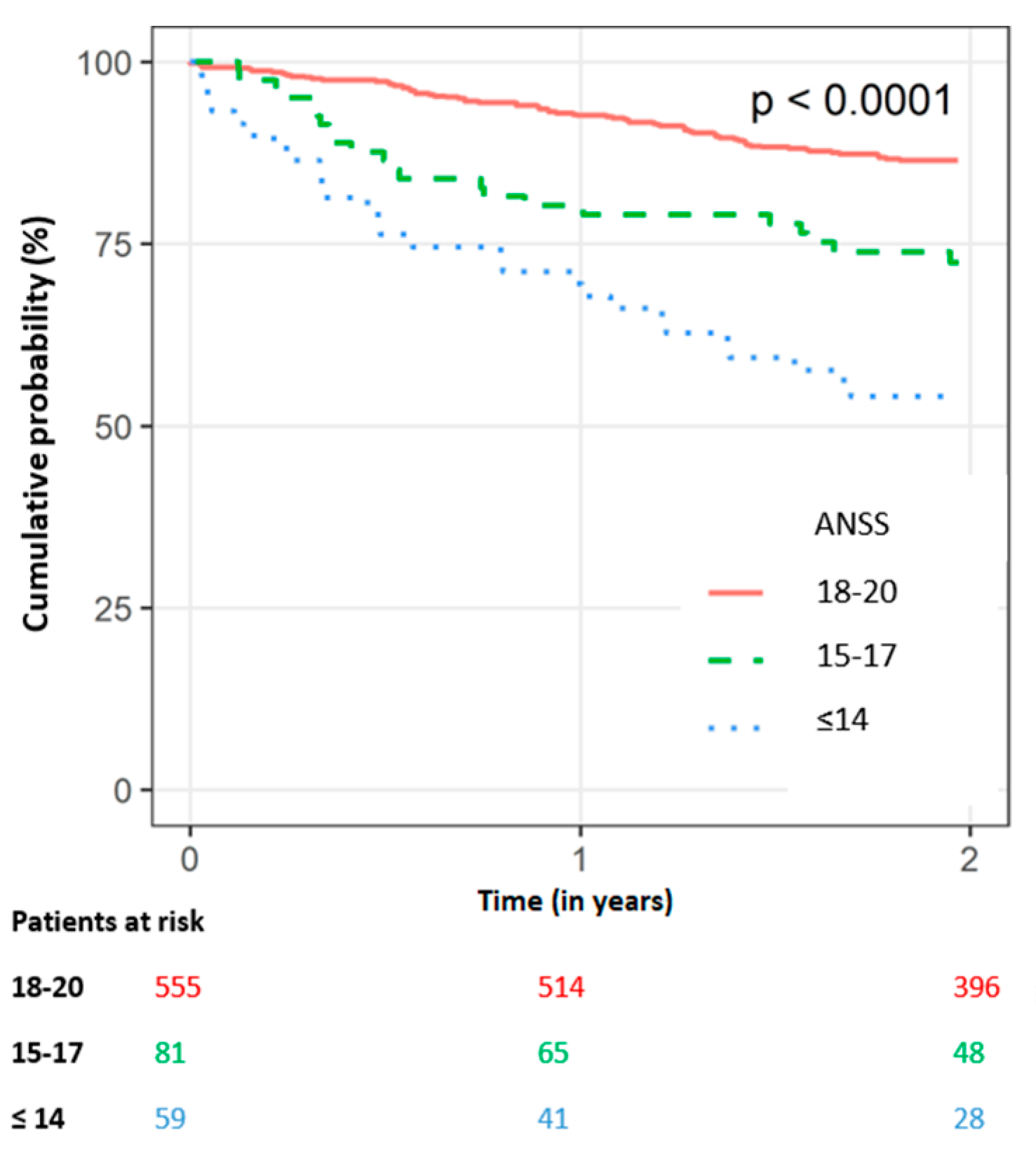
3.2. All-Cause Mortality
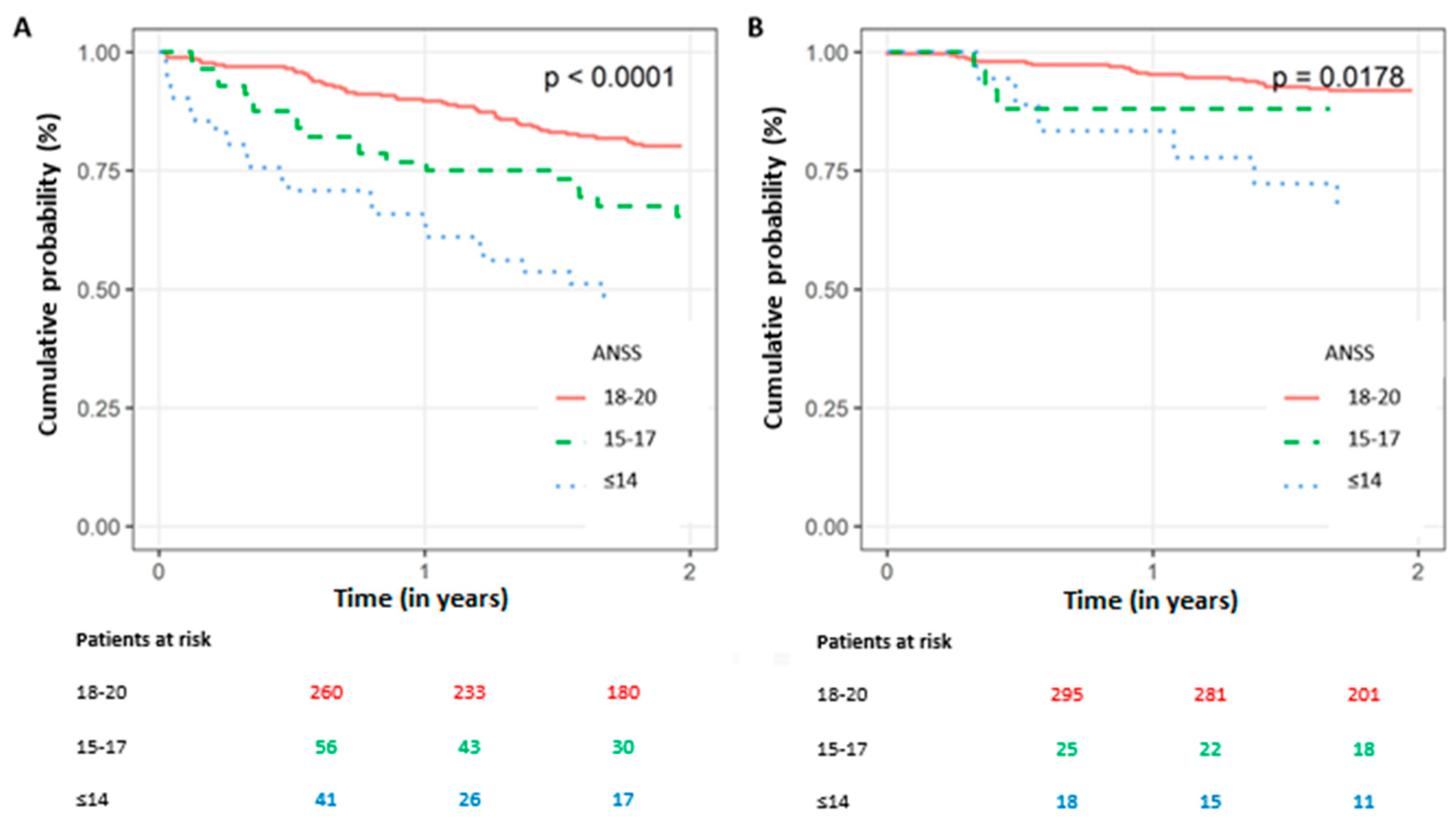
3.3. Patients Not Receiving Appropriate ICD Therapy
3.4. Association with Known Predictors of Poor Prognosis
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L. Prophylactic Implantation of a Defibrillator in Patients with Myocardial Infarction and Reduced Ejection Fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Amiodarone or an Implantable Cardioverter-Defibrillator for Congestive Heart Failure. N. Engl. J. Med. 2005, 352, 225–237. [Google Scholar] [CrossRef]
- McAnulty, J.; Halperin, B.; Kron, J.; Larsen, G.; Raitt, M.; Swenson, R.; Florek, R.; Marchant, C.; Hamlin, M.; Heywood, G.; et al. A Comparison of Antiarrhythmic-Drug Therapy with Implantable Defibrillators in Patients Resuscitated from near-Fatal Ventricular Arrhythmias. N. Engl. J. Med. 1997, 337, 1576–1583. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) With the Special Contributio. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Heinzel, F.R.; Gaita, F.; Juanatey, J.R.G.; Le Heuzey, J.Y.; Potpara, T.; Svendsen, J.H.; Vos, M.A.; Anker, S.D.; Coats, A.J.; et al. European Heart Rhythm Association/Heart Failure Association Joint Consensus Document on Arrhythmias in Heart Failure, Endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Eur. J. Heart Fail. 2015, 17, 848–874. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.; Blom, N.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C. 2022 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Developed by the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Stevenson, L.W.; Desai, A.S. Selecting Patients for Discussion of the ICD as Primary Prevention for Sudden Death in Heart Failure. J. Card. Fail. 2006, 12, 407–412. [Google Scholar] [CrossRef]
- Buxton, A.E.; Lee, K.L.; Hafley, G.E.; Pires, L.A.; Fisher, J.D.; Gold, M.R.; Josephson, M.E.; Lehmann, M.H.; Prystowsky, E.N. Limitations of Ejection Fraction for Prediction of Sudden Death Risk in Patients With Coronary Artery Disease. Lessons From the MUSTT Study. J. Am. Coll. Cardiol. 2007, 50, 1150–1157. [Google Scholar] [CrossRef] [Green Version]
- Fishman, G.I.; Chugh, S.S.; Dimarco, J.P.; Albert, C.M.; Anderson, M.E.; Bonow, R.O.; Buxton, A.E.; Chen, P.S.; Estes, M.; Jouven, X.; et al. Sudden Cardiac Death Prediction and Prevention: Report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation 2010, 122, 2335–2348. [Google Scholar] [CrossRef]
- Sabbag, A.; Suleiman, M.; Laish-Farkash, A.; Samania, N.; Kazatsker, M.; Goldenberg, I.; Glikson, M.; Beinart, R. Contemporary Rates of Appropriate Shock Therapy in Patients Who Receive Implantable Device Therapy in a Real-World Setting: From the Israeli ICD Registry. Hear. Rhythm 2015, 12, 2426–2433. [Google Scholar] [CrossRef]
- Koller, M.T.; Schaer, B.; Wolbers, M.; Sticherling, C.; Bucher, H.C.; Osswald, S. Death Without Prior Appropriate Implantable Cardioverter-Defibrillator Therapy. Circulation 2008, 117, 1918–1926. [Google Scholar] [CrossRef] [Green Version]
- Disertori, M.; Quintarelli, S.; Mazzola, S.; Favalli, V.; Narula, N.; Arbustini, E. The Need to Modify Patient Selection to Improve the Benefits of Implantable Cardioverter-Defibrillator for Primary Prevention of Sudden Death in Non-Ischaemic Dilated Cardiomyopathy. Europace 2013, 15, 1693–1701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldenberg, I.; Vyas, A.K.; Hall, W.J.; Moss, A.J.; Wang, H.; He, H.; Zareba, W.; McNitt, S.; Andrews, M.L. Risk Stratification for Primary Implantation of a Cardioverter-Defibrillator in Patients With Ischemic Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 2008, 51, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaura, A.; Sunderland, N.; Kamdar, R.; Petzer, E.; McDonagh, T.; Murgatroyd, F.; Dhillon, P.; Scott, P. Identifying Patients with Less Potential to Benefit from Implantable Cardioverter-Defibrillator Therapy: Comparison of the Performance of Four Risk Scoring Systems. J. Interv. Card. Electrophysiol. 2017, 49, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.Y.; Orkaby, A.R.; Rosenberg, M.A.; Driver, J.A. Frailty, Implantable Cardioverter Defibrillators, and Mortality: A Systematic Review. J. Gen. Intern. Med. 2019, 34, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Šateková, L.; Žiaková, K.; Zeleníková, R. Predictive Validity of the Braden Scale, Norton Scale, and Waterlow Scale in the Czech Republic. Int. J. Nurs. Pract. 2017, 23, e12499. [Google Scholar] [CrossRef] [Green Version]
- Norton, D.; Exton-Smith, A.N.; McLaren, R. An Investigation of Geriatric Nursing Problems in Hospital. Br. J. Psychiatry 1963, 109, 152–153. [Google Scholar] [CrossRef]
- Silber, H.; Shiyovich, A.; Gilutz, H.; Ziedenberg, H.; Abu Tailakh, M.; Plakht, Y. Decreased Norton’s Functional Score Is an Independent Long-Term Prognostic Marker in Hospital Survivors of Acute Myocardial Infarction. Soroka Acute Myocardial Infarction II (SAMI-II) Project. Int. J. Cardiol. 2017, 228, 694–699. [Google Scholar] [CrossRef]
- Rabinovitz, E.; Finkelstein, A.; Ben Assa, E.; Steinvil, A.; Konigstein, M.; Shacham, Y.; Yankelson, L.; Banai, S.; Justo, D.; Leshem-Rubinow, E. Norton Scale for Predicting Prognosis in Elderly Patients Undergoing Trans-Catheter Aortic Valve Implantation: A Historical Prospective Study. J. Cardiol. 2016, 67, 519–525. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, I.; Moss, A.J.; McNitt, S.; Zareba, W.; Andrews, M.L.; Hall, W.J.; Greenberg, H.; Case, R.B. Relations Among Renal Function, Risk of Sudden Cardiac Death, and Benefit of the Implanted Cardiac Defibrillator in Patients With Ischemic Left Ventricular Dysfunction. Am. J. Cardiol. 2006, 98, 485–490. [Google Scholar] [CrossRef]
- Cuculich, P.S.; Sánchez, J.M.; Kerzner, R.; Greenberg, S.L.; Sengupta, J.; Chen, J.; Faddis, M.N.; Gleva, M.J.; Smith, T.W.; Lindsay, B.D. Poor Prognosis for Patients with Chronic Kidney Disease despite ICD Therapy for the Primary Prevention of Sudden Death. PACE—Pacing Clin. Electrophysiol. 2007, 30, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Reilly, E.F.; Karakousis, G.C.; Schrag, S.P.; Stawicki, S. Pressure Ulcers in the Intensive Care Unit: The “forgotten” Enemy. OPUS 12 Sci. 2007, 1, 17–30. [Google Scholar]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Circulation 2018, 138, e272–e391. [Google Scholar] [CrossRef] [Green Version]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajduk, A.M.; Gurwitz, J.H.; Tabada, G.; Masoudi, F.A.; Magid, D.J.; Greenlee, R.T.; Sung, S.H.; Cassidy-Bushrow, A.E.; Liu, T.I.; Reynolds, K.; et al. Influence of Multimorbidity on Burden and Appropriateness of Implantable Cardioverter-Defibrillator Therapies. J. Am. Geriatr. Soc. 2019, 67, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.; Boveda, S.; Defaye, P.; Sadoul, N.; Narayanan, K.; Perier, M.-C.; Klug, D.; Fauchier, L.; Leclercq, C.; Babuty, D.; et al. Early Mortality after Implantable Cardioverter Defibrillator: Incidence and Associated Factors. Int. J. Cardiol. 2020, 301, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Parkash, R.; Stevenson, W.G.; Epstein, L.M.; Maisel, W.H. Predicting Early Mortality after Implantable Defibrillator Implantation: A Clinical Risk Score for Optimal Patient Selection. Am. Heart J. 2006, 151, 397–403. [Google Scholar] [CrossRef]
- Kramer, D.B.; Friedman, P.A.; Kallinen, L.M.; Morrison, T.B.; Crusan, D.J.; Hodge, D.O.; Reynolds, M.R.; Hauser, R.G. Development and Validation of a Risk Score to Predict Early Mortality in Recipients of Implantable Cardioverter-Defibrillators. Hear. Rhythm 2012, 9, 42–46. [Google Scholar] [CrossRef]
- Kraaier, K.; Scholten, M.F.; Tijssen, J.G.P.; Theuns, D.A.M.J.; Jordaens, L.J.L.M.; Wilde, A.A.M.; van Dessel, P.F.H.M. Early Mortality in Prophylactic Implantable Cardioverter-Defibrillator Recipients: Development and Validation of a Clinical Risk Score. EP Eur. 2014, 16, 40–46. [Google Scholar] [CrossRef]
- Younis, A.; Goldberger, J.J.; Kutyifa, V.; Zareba, W.; Polonsky, B.; Klein, H.; Aktas, M.K.; Huang, D.; Daubert, J.; Estes, M.; et al. Predicted Benefit of an Implantable Cardioverter-Defibrillator: The MADIT-ICD Benefit Score. Eur. Heart J. 2021, 42, 1676–1684. [Google Scholar] [CrossRef]
- Bansal, N.; Szpiro, A.; Reynolds, K.; Smith, D.H.; Magid, D.J.; Gurwitz, J.H.; Masoudi, F.; Greenlee, R.T.; Tabada, G.H.; Sung, S.H.; et al. Long-Term Outcomes Associated With Implantable Cardioverter Defibrillator in Adults With Chronic Kidney Disease. JAMA Intern. Med. 2018, 178, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Jukema, J.W.; Timal, R.J.; Rotmans, J.I.; Hensen, L.C.R.; Buiten, M.S.; de Bie, M.K.; Putter, H.; Zwinderman, A.H.; van Erven, L.; Straaten, M.J.K.; et al. Prophylactic Use of Implantable Cardioverter-Defibrillators in the Prevention of Sudden Cardiac Death in Dialysis Patients. Circulation 2019, 139, 2628–2638. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Overall | ANSS ≤ 14 | ANSS 15–17 | ANSS 18–20 | p Value |
|---|---|---|---|---|---|
| Study Population | n = 695 | n = 59 | n = 81 | n = 555 | |
| Age at procedure (years) ± SD | 66 ± 14 | 70 ± 14 | 70 ± 12 | 65 ± 14 | 0.001 |
| Female (%) | 106 (15) | 10 (17) | 14 (17) | 82 (15) | 0.783 |
| ANSS (median (IQR)) | 19 (18–20) | 12 (10–14) | 17 (16–17) | 19 (19–20) | <0.001 |
| High clinical risk * (%) | 357 (51) | 41 (70) | 56 (69) | 260 (47) | <0.001 |
| De-novo ICD implantation (%) | 461 (66) | 42 (71) | 52 (65) | 367 (67) | 0.734 |
| Prior myocardial infarction (%) | 262 (38) | 19 (32) | 33 (41) | 210 (38) | 0.546 |
| Congestive heart failure (%) | 345 (50) | 37 (62) | 49 (61) | 259 (47) | 0.008 |
| Atrial fibrillation (%) | 200 (29) | 22 (37) | 28 (35) | 150 (27) | 0.128 |
| Prior CVA (%) | 80 (12) | 17 (29) | 16 (20) | 47 (9) | <0.001 |
| Prior TIA (%) | 19 (0.03) | 1 (2) | 1 (1) | 17 (3) | 0.560 |
| Dyslipidemia (%) | 321 (46) | 28 (48) | 37 (46) | 256 (46) | 0.990 |
| Currently on dialysis (%) | 3 (0.004) | 1 (2) | 1 (1) | 1 (0.2) | 0.123 |
| Hypertension (%) | 358 (52) | 31 (53) | 47 (59) | 280 (51) | 0.430 |
| Diabetes mellitus (%) | 235 (34) | 29 (49) | 35 (44) | 171 (31) | 0.003 |
| Smoker (%) | 165 (24) | 13 (22) | 19 (24) | 133 (24) | 0.931 |
| BMI (kg/m2), ±SD | 27 ± 5 | 27 ± 6 | 27 ± 5 | 27 ± 5 | 0.707 |
| GFR MDRD (mL/min/1.73 m2), ±SD | 65 ± 32 | 66 ± 59 | 61 ± 26 | 66 ± 28 | 0.462 |
| Serum creatinine (mg/dL), ±SD | 1.3 ± 0.7 | 1.5 ± 1 | 1.4 ± 0.9 | 1.3 ± 0.6 | 0.024 |
| Hemoglobin (g/dL), ±SD | 13 ± 2 | 11 ± 2 | 12 ± 2 | 13 ± 2 | <0.001 |
| Serum albumin (g/dL), ±SD | 4 ± 0.5 | 3 ± 0.6 | 4 ± 0.5 | 4 ± 0.4 | <0.001 |
| LV ejection fraction (%), ±SD | 32 ± 14 | 33 ± 14 | 32 ± 14 | 32 ± 14 | 0.851 |
| ACE inhibitors (%) | 453 (65) | 39 (66) | 51 (63) | 363 (65) | 0.900 |
| Aldosterone antagonists (%) | 422 (61) | 37 (63) | 58 (72) | 327 (59) | 0.087 |
| Beta-blockers (%) | 185 (27) | 17 (29) | 17 (21) | 151 (27) | 0.459 |
| Antiarrhythmics: | |||||
| Class IB (%) | 27 (4) | 3 (5) | 4 (5) | 20 (4) | 0.746 |
| Class IC (%) | 23 (3) | 2 (3) | 3 (4) | 18 (3) | 0.976 |
| Class III (%) | 330 (47) | 35 (59) | 36 (44) | 259 (47) | 0.152 |
| Salicylic acid (%) | 13 (2) | 0 (0) | 1 (1) | 12 (2) | 0.458 |
| Univariable Model | Multivariable Model | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (year) | 1.03 | 1.02–1.05 | <0.001 | 1.02 | 1.00–1.03 | 0.018 |
| Gender (Female) | 0.73 | 0.46–1.16 | 0.179 | |||
| CHF | 2.98 | 2.14–4.14 | <0.001 | 2.15 | 1.52–3.04 | <0.001 |
| DM | 1.66 | 1.23–2.25 | <0.001 | |||
| Renal Disease | 2.85 | 2.11–3.84 | <0.001 | 1.89 | 1.37–2.61 | <0.001 |
| Prior CVA | 1.54 | 1.02–2.32 | 0.040 | |||
| ANSS | ||||||
| High (18–20) (reference) | 1 | 1 | — | |||
| Intermediate (15–17) | 1.78 | 1.17–2.70 | 0.007 | 1.57 | 1.03–2.39 | 0.036 |
| Low (≤14) | 3.21 | 2.15–4.79 | <0.001 | 2.39 | 1.59–3.60 | <0.001 |
| Univariable Models | Multivariable Model | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (year) | 1.04 | 1.03–1.06 | <0.001 | 1.02 | 1.01–1.04 | 0.010 |
| Gender (Female) | 0.68 | 0.40–1.17 | 0.163 | |||
| CHF | 3.31 | 2.23–4.89 | 0.001 | 2.22 | 1.47–3.36 | <0.001 |
| DM | 1.76 | 1.25–2.48 | 0.001 | |||
| Renal Disease | 3.37 | 2.38–4.75 | <0.001 | 2.12 | 1.46–3.07 | <0.001 |
| Prior CVA | 1.69 | 1.08–2.65 | 0.023 | |||
| ANSS | ||||||
| High (18–20) (reference) | 1 | — | — | 1 | — | — |
| Intermediate (15–17) | 1.88 | 1.17–3.00 | 0.009 | 1.58 | 0.98–2.53 | 0.058 |
| Low (≤14) | 3.27 | 2.06–5.18 | <0.001 | 2.29 | 1.44–3.77 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ben Asher Kestin, S.; Israel, A.; Leshem, E.; Milman, A.; Sabbag, A.; Goldengerg, I.; Nof, E.; Beinart, R. Can the Norton Scale Score Be Used as an Adjunct Tool for Implantable Defibrillator Patient Selection? A Retrospective Single-Center Cohort Study. J. Clin. Med. 2023, 12, 214. https://doi.org/10.3390/jcm12010214
Ben Asher Kestin S, Israel A, Leshem E, Milman A, Sabbag A, Goldengerg I, Nof E, Beinart R. Can the Norton Scale Score Be Used as an Adjunct Tool for Implantable Defibrillator Patient Selection? A Retrospective Single-Center Cohort Study. Journal of Clinical Medicine. 2023; 12(1):214. https://doi.org/10.3390/jcm12010214
Chicago/Turabian StyleBen Asher Kestin, Shir, Ariel Israel, Eran Leshem, Anat Milman, Avi Sabbag, Ilan Goldengerg, Eyal Nof, and Roy Beinart. 2023. "Can the Norton Scale Score Be Used as an Adjunct Tool for Implantable Defibrillator Patient Selection? A Retrospective Single-Center Cohort Study" Journal of Clinical Medicine 12, no. 1: 214. https://doi.org/10.3390/jcm12010214