
Effect of Age on Heart Rate Variability in Patients with Mitral Valve Prolapse: An Observational Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Information
2.2. Study Population
2.3. HRV Evaluation
2.4. Time Domain (TD)
- SDNN (ms): standard deviation of the NN interval time series.
- RMSSD (ms): square root of the mean squared differences of successive NN intervals.
- NN50: number of pairs of successive NN (R-R) intervals that differ by >50 ms.
- pNN50 (arbitrary units): proportion derived by dividing the number of interval differences of successive NN intervals > 50 ms by the total number of NN intervals.
2.5. Frequency Domain (FD)
- Equal to the TD indices, the following standardized HRV indices from the Task Force Guideline of the FD were extracted:
- Total power (ms2): total power of the power spectral density in the range of frequencies between 0 and 0.4 Hz.
- VLF (ms2; very low frequency): a band of power spectrum range between 0.0033 and 0.04 Hz.
- LF (ms2): power in the “low”-frequency band (0.04–0.15 Hz).
- HF (ms2): power in the “high”-frequency band (0.15–0.4 Hz).
- LF/HF (arbitrary units): ratio between LF and HF.
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. HRV Parameters between the MVP and Control Groups
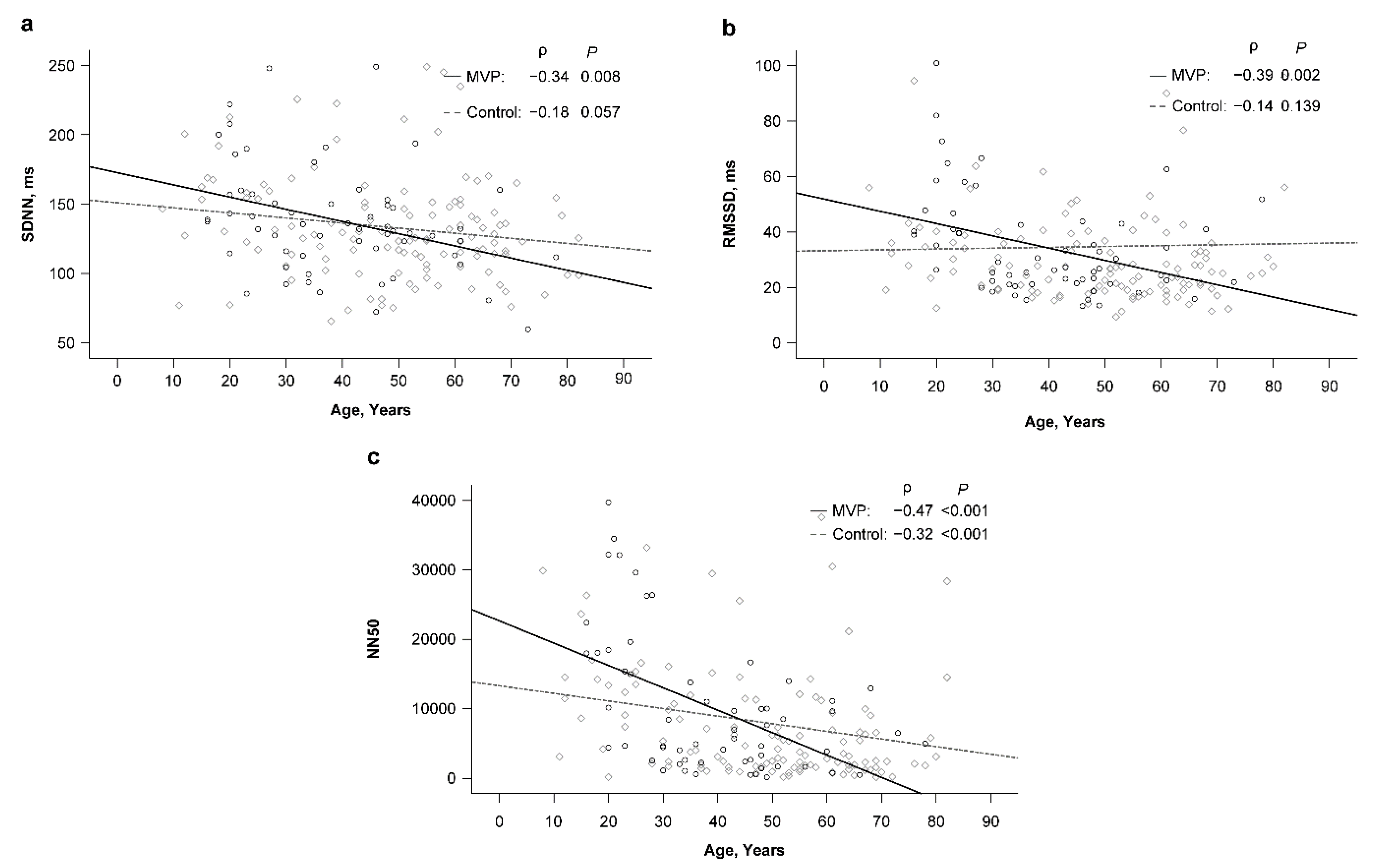
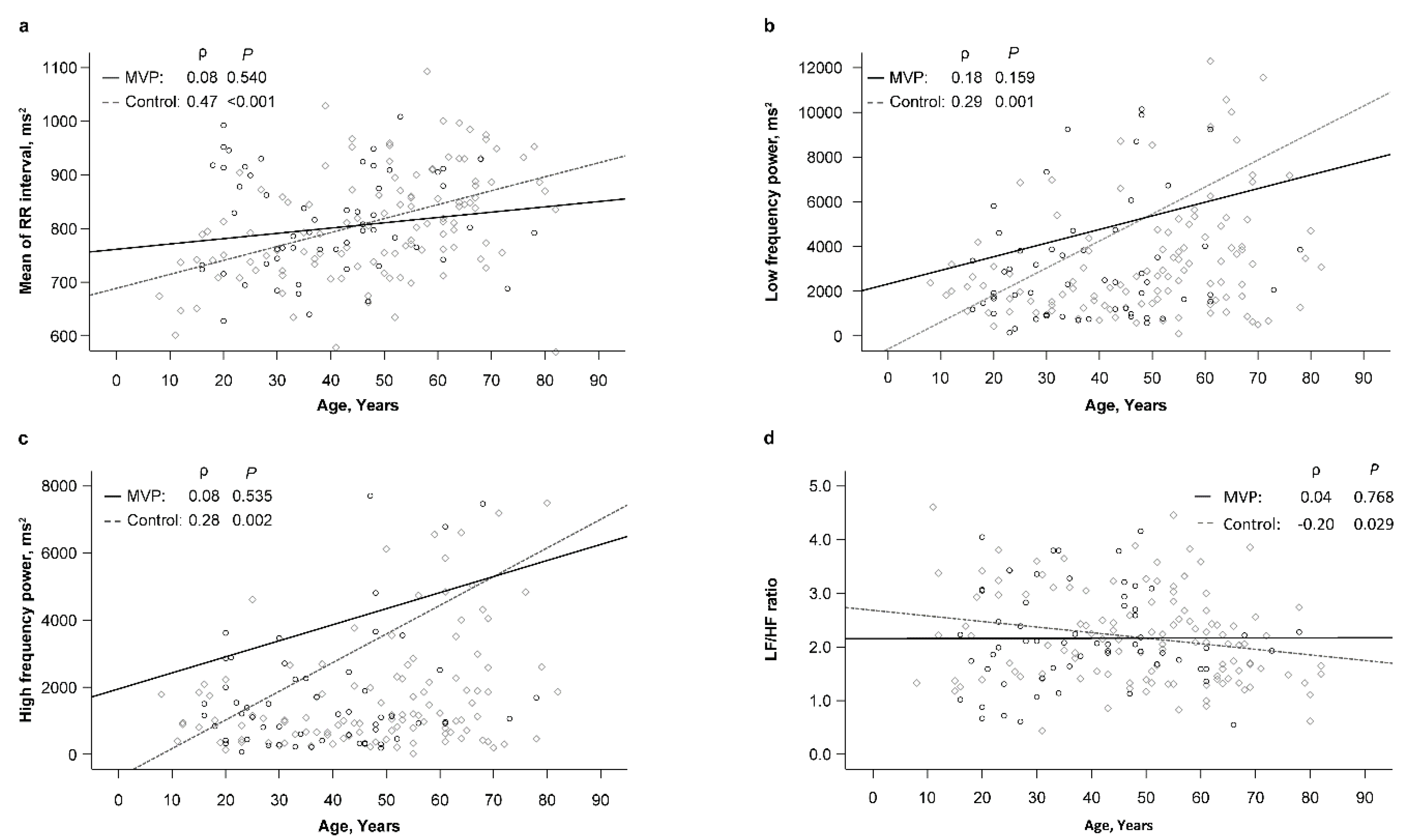
3.3. Relationship between Age and HRV Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zuppiroli, A.; Mori, F.; Favilli, S.; Barchielli, A.; Corti, G.; Montereggi, A.; Dolara, A. Arrhythmias in mitral valve prolapse: Relation to anterior mitral leaflet thickening, clinical variables, and color doppler echocardiographic parameters. Am. Heart J. 1994, 128, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Turker, Y.; Ozaydın, M.; Acar, G.; Ozgul, M.; Hoscan, Y.; Varol, E.; Dogan, A.; Erdogan, D.; Yucel, H. Predictors of ventricular arrhythmias in patients with mitral valve prolapse. Int. J. Cardiovasc. Imaging 2010, 26, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Erkal, Z.; Bayar, N.; Koklu, E.; Cagırcı, G.; Arslan, S.; Guven, R. Supraventricular arrhythmia in mitral valve prolapse: Predictive value of P-wave dispersion and atrial conduction time. Herz 2022, 47, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Hayek, E.; Gring, C.N.; Griffin, B.P. Mitral valve prolapse. Lancet 2005, 365, 507–518. [Google Scholar] [CrossRef]
- Toomer, K.A.; Yu, M.; Fulmer, D.; Guo, L.; Moore, K.S.; Moore, R.; Drayton, K.D.; Glover, J.; Peterson, N.; Ramos-Ortiz, S.; et al. Primary cilia defects causing mitral valve prolapse. Sci. Transl. Med. 2019, 11, eaax0290. [Google Scholar] [CrossRef] [Green Version]
- Qurat-ul-Ain, J. Mitral Valve Prolapse. Medscape 2022. Available online: http://emedicine.medscape.com/article/155494-overview (accessed on 23 March 2022).
- Watkins, P.C. Treatment of symptomatic mitral valve prolapse syndrome and dysautonomia. Cardiol Rev 1997, 5, 208–212. [Google Scholar] [CrossRef]
- Styres, K.S. The phenomenon of dysautonomia and mitral valve prolapse. J. Am. Acad. Nurse Pract. 1994, 6, 11–15. [Google Scholar] [CrossRef]
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular neural regulation explored in the frequency domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.; Camm, A.J. Heart rate variability. Clin. Cardiol. 1990, 13, 570–576. [Google Scholar] [CrossRef]
- Bigger, J.T.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Kleiger, R.E.; Rottman, J.N. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 1992, 85, 164–171. [Google Scholar] [CrossRef]
- Bigger, J.T.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Schneider, W.J.; Stein, P.K. RR variability in healthy, middle-aged persons compared with patients with chronic coronary heart disease or recent acute myocardial infarction. Circulation 1995, 91, 1936–1943. [Google Scholar] [CrossRef] [PubMed]
- Molgaard, H.; Sorensen, K.E.; Bjerregard, P. Attenuated 24-h heart rate variability in apparently healthy subjects, subsequently suffering sudden cardiac death. Clin. Auton Res. 1991, 1, 223–233. [Google Scholar] [CrossRef]
- Saul, J.P.; Arai, Y.; Berger, R.D.; Lilly, L.S.; Colucci, W.S.; Cohen, R.J. Assessment of autonomic regulation in chronic congestive heart failure by heart rate spectral analysis. Am. J. Cardiol. 1988, 61, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Weise, F.; Heydenreich, F.; Runge, U. Heart rate fluctuations in diabetic patients with cardiac vagal dysfunction: A spectral analysis. Diabet Med. 1988, 5, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, B.; Gundersen, H.J.G. Analysis of heart rate variations in patients with multiple sclerosis. A simple measure of autonomic nervous disturbances using an ordinary ECG. J. Neurol. Neurosurg Psychiatry 1978, 41, 417–419. [Google Scholar] [CrossRef] [Green Version]
- Kariniemi, V.; Ammälä, P. Short-term variability of fetal heart rate during pregnancies with normal and insufficient placental function. Am. J. Obstet. Gynecol. 1981, 139, 33–37. [Google Scholar] [CrossRef]
- Yeragani, V.K. Heart rate and blood pressure variability: Implications for psychiatric research. Neuropsychobiology 1995, 32, 182–191. [Google Scholar] [CrossRef]
- Boudoulas, H. Mitral valve prolapse: Etiology, clinical presentation and neuroendocrine function. J. Heart Valve Dis. 1992, 1, 175–188. [Google Scholar]
- Davies, A.O.; Mares, A.; Pool, J.L.; Taylor, A.A. Mitral valve prolapse with symptoms of beta-adrenergic hypersensitivity. Beta 2-adrenergic receptor supercoupling with desensitization on isoproterenol exposure. Am. J. Med. 1987, 82, 193–201. [Google Scholar] [CrossRef]
- Boudoulas, H.; Reynolds, J.C.; Mazzaferri, E.; Wooley, C.F. Metabolic studies in mitral valve prolapse syndrome. A neuroendocrine-cardiovascular process. Circulation 1980, 61, 1200–1205. [Google Scholar] [CrossRef] [Green Version]
- Barlow, J.B.; Pocock, W.A. Mitral valve prolapse, the specific billowing mitral leaflet syndrome, or an insignificant non-ejection systolic click. Am. Heart J. 1979, 97, 277–285. [Google Scholar] [CrossRef]
- Boudoulas, H.; Reynolds, J.C.; Mazzaferri, E.; Wooley, C.F. Mitral valve prolapse syndrome: The effect of adrenergic stimulation. J. Am. Coll. Cardiol. 1983, 2, 638–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strano, S.; De Castro, S.; Ferrucci, A.; Mazzei, A.; Urani, C.; Giannantoni, P.; Marcheselli, A.; Massimo Ciavarella, G.; Calcagnini, G.; Cerutti, S. Modification of the sympatho-vagal interaction in mitral valve prolapse syndrome. Evaluation of heart rate variability by spectrum analysis. Cardiologia 1992, 37, 755–760. [Google Scholar] [PubMed]
- Keller, K.M.; Howlett, S.E. Sex differences inthe biology and pathology of the aging heart. Can. J. Cardiol. 2016, 32, 1065–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namazi, H.; Baleanu, D.; Krejcar, O. Age-based analysis of heart rate variability (HRV) for patients with congestive heart failure. Fractals 2021, 29, 2150135. [Google Scholar] [CrossRef]
- Garavaglia, L.; Gulich, D.; Defeo, M.M.; Thomas, M.J.; Irurzun, I.M. The effect of age on the heart rate variability of healthy subjects. PLoS ONE 2021, 16, e0255894. [Google Scholar] [CrossRef]
- Jensen-Urstad, K.; Storck, N.; Bouvier, F.; Ericson, M.; Lindblad, L.E.; Jensen-Urstad, M. Heart rate variability in healthy subjects is related to age and gender. Acta Physiol. Scand 1997, 160, 235–241. [Google Scholar] [CrossRef]
- Shannon, D.C.; Carley, D.W.; Benson, H. Aging of modulation of heart rate. Am. J. Physiol. 1987, 253, H874–H877. [Google Scholar] [CrossRef]
- Schwartz, J.B.; Gibb, W.J.; Tran, T. Aging effects on heart rate variation. J. Gerontol. 1991, 46, M99–M106. [Google Scholar] [CrossRef]
- Yeragani, V.K.; Pohl, R.; Berger, R.; Balon, R.; Srinivasan, K. Relationship between age and heart rate variability in supine and standing postures: A study of spectral analysis of heart rate. Pediatr. Cardiol. 1994, 15, 14–20. [Google Scholar] [CrossRef]
- Levine, R.A.; Stathogiannis, E.; Newell, J.B.; Harrigan, P.; Weyman, A.E. Reconsideration of echocardiographic standards for mitral valve prolapse: Lack of association between leaflet displacement isolated to the apical four chamber view and independent echocardiographic evidence of abnormality. J. Am. Coll. Cardiol. 1988, 11, 1010–1019. [Google Scholar] [CrossRef]
- Levine, R.A.; Triulzi, M.O.; Harrigan, P.; Weyman, A.E. The relationship of mitral annular shape to the diagnosis of mitral valve prolapse. Circulation 1987, 75, 756–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marek, M.J.; Thomas, B.A.; John, C.; Robert, E.K.; Alberto, M.; Arthur, J.M.; Peter, J.S. Heart rate variability: Standards of measurement, physiologic interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Gaffney, F.A.; Karlsson, E.S.; Campbell, W.; Schutte, J.E.; Nixon, J.V.; Willerson, J.T.; Blomqvist, C.G. Autonomic dysfunction in women with mitral valve prolapse syndrome. Circulation 1979, 59, 894–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochiadakis, G.E.; Parthenakis, F.I.; Zuridakis, E.G.; Rombola, A.T.; Chrysostomakis, S.I.; Vardas, P.E. Is there increased sympathetic activity in patients with mitral valve prolapse? Pacing Clin. Electrophysiol. 1996, 19, 1872–1876. [Google Scholar] [CrossRef]
- Lenders, J.W.M.; Fast, J.H.; Blankers, J.; de Boo, T.; Lemmens, W.A.; Thien, T. Normal sympathetic neural activity in patients with mitral valve prolapse. Clin. Cardiol. 1986, 9, 177–182. [Google Scholar] [CrossRef]
- Abhishekh, H.A.; Nisarga, P.; Kisan, R.; Meghana, A.; Chandran, S.; Trichur Raju, S.; Sathyaprabha, T.N. Influence of age and gender on autonomic regulation of heart. J. Clin. Monit Comput. 2013, 27, 259–264. [Google Scholar] [CrossRef]
- Boudreau, P.; Yeh, W.H.; Dumont, G.A.; Boivin, D.B. A circadian rhythm in heart rate variability contributes to the increased cardiac sympathovagal response to awakening in the morning. Chronobiol. Int. 2012, 29, 757–768. [Google Scholar] [CrossRef]
- Vigo, D.E.; Guinjoan, S.M.; Scaramal, M.; Siri, L.N.; Cardinali, D.P. Wavelet transform shows age-related changes of heart rate variability within independent frequency components. Auton Neurosci. 2005, 123, 94–100. [Google Scholar] [CrossRef]
- Langer, S.F.J.; Lambertz, M.; Langhorst, P.; Schmidt, H.D. Interbeat interval variability in isolated working rat hearts at various dynamic conditions and temperatures. Res. Exp. Med. (Berl) 1999, 199, 1–19. [Google Scholar] [CrossRef]
- Scheuer, D.A.; Mifflin, S.W. Glucocorticoids modulate baroreflex control of renal sympathetic nerve activity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 280, R1440–R1449. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before Propensity Score Matching | After Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Variable | MVP (n = 60) | Control (n = 120) | p-Value | MVP (n = 52) | Control (n = 52) | p-Value |
| age, year | 39.0 ± 15.4 | 48.9 ± 18.1 | <0.001 | 41.5 ± 15.0 | 39.8 ± 18.5 | 0.621 |
| female | 46 (76.7) | 80 (66.7) | 0.227 | 41 (78.8) | 40 (76.9) | 1.000 |
| heart rate, bpm | 77.0 ± 8.1 | 77.1 ± 9.9 | 0.946 | 77.9 ± 7.9 | 79.4 ± 11.0 | 0.427 |
| smoking | 11 (18.3) | 12 (10.0) | 0.154 | 6 (11.5) | 6 (11.5) | 1.000 |
| coffee | 10 (16.7) | 28 (23.3) | 0.338 | 10 (19.2) | 11 (21.2) | 1.000 |
| insomnia | 6 (10.0) | 10 (8.3) | 0.783 | 5 (9.6) | 5 (9.6) | 1.000 |
| syncope | 6 (10.0) | 18 (15.0) | 0.486 | 5 (9.6) | 7 (13.5) | 0.760 |
| Before Propensity Score Matching | After Propensity Score Matching | |||||
|---|---|---|---|---|---|---|
| Variable | MVP (n = 60) | Control (n = 120) | p-value | MVP (n = 52) | Control (n = 52) | p-Value |
| SDNN, ms | 132.2 [113.1, 156.9] | 127.3 [112.0, 153.4] | 0.386 | 130.6 [111.7, 147.3] | 130.2 [113.9, 158.8] | 0.480 |
| RMSSD, ms | 27.3 [21.5, 42.6] | 26.9 [19.1, 37.6] | 0.215 | 26.3 [21.3, 39.5] | 27.8 [20.1, 41.9] | 0.616 |
| NN50 | 6504 [2567, 14,964] | 4230 [1722, 11,281] | 0.077 | 4926 [2275, 11,003] | 7363 [2103, 14,239] | 0.384 |
| PNN50, % | 6.3 [2.3, 14.9] | 4.5 [1.7, 11.4] | 0.119 | 4.8 [2.1, 11.1] | 6.4 [2.1, 12.9] | 0.470 |
| RR interval | ||||||
| mean, ms2 | 796.1 [732.1, 905.4] | 805.1 [738.2, 886.4] | 0.813 | 785.8 [730.0, 874.8] | 766.2 [735.2, 858.1] | 0.833 |
| VLF, ms2 | 2958 [1482, 4958] | 2815 [1773, 4636] | 0.844 | 2747 [1427, 4972] | 2804 [1922, 4704] | 0.644 |
| LF, ms2 | 2402 [1191, 4655] | 2729 [1540, 5096] | 0.381 | 2448 [1191, 4724] | 2361 [1540, 4681] | 0.805 |
| HF, ms2 | 1179 [522, 2613] | 1168 [658, 2680] | 0.603 | 1179 [522, 2787] | 1046 [626, 2485] | 0.969 |
| Total, ms2 | 6449 [3238, 11,540] | 7151 [4172, 12,800] | 0.455 | 6449 [3238, 12,074] | 6884 [4113, 12,061] | 0.673 |
| LF/HF ratio | 2.05 [1.60, 2.80] | 2.08 [1.46, 2.79] | 0.999 | 2.05 [1.60, 2.86] | 2.03 [1.42, 2.99] | 0.828 |
| Variable | Regression coefficient of MVP (95% CI) * | p-Value |
|---|---|---|
| SDNN, ms | 3.6 (−8.6, 15.8) | 0.560 |
| RMSSD, ms | −1.5 (−7.3, 4.2) | 0.602 |
| NN50 | 38.3 (−2494.6, 2571.2) | 0.976 |
| PNN50, % | 0.35 (−2.49, 3.19) | 0.810 |
| RR interval | ||
| mean, ms2 | 5.6 (−36.2, 47.4) | 0.792 |
| VLF, ms2 | 246.1 (−749.4, 1241.5) | 0.626 |
| LF, ms2 | −81.5 (−1128.5, 965.4) | 0.878 |
| HF, ms2 | −79.1 (−713.7, 555.5) | 0.806 |
| Total, ms2 | −229.5 (−2821.7, 2362.7) | 0.861 |
| LF/HF ratio | −0.10 (−0.51, 0.32) | 0.653 |
| MVP | Control | |||
|---|---|---|---|---|
| Variable | ρ | p-Value | ρ | p-Value |
| SDNN, ms | −0.34 | 0.008 | −0.18 | 0.057 |
| RMSSD, ms | −0.39 | 0.002 | −0.14 | 0.139 |
| NN50 | −0.47 | <0.001 | −0.32 | <0.001 |
| PNN50, % | −0.46 | <0.001 | −0.24 | 0.008 |
| RR interval | ||||
| mean, ms2 | 0.08 | 0.540 | 0.47 | <0.001 |
| VLF, ms2 | 0.09 | 0.500 | 0.17 | 0.062 |
| LF, ms2 | 0.18 | 0.159 | 0.29 | 0.001 |
| HF, ms2 | 0.08 | 0.535 | 0.28 | 0.002 |
| Total, ms2 | 0.12 | 0.353 | 0.27 | 0.003 |
| LF/HF ratio | 0.04 | 0.768 | −0.20 | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.-K.; Huang, S.-Y.; Lee, C.-h.; Yang, I.-F.; Yang, T.-F.; Wang, Y.-M. Effect of Age on Heart Rate Variability in Patients with Mitral Valve Prolapse: An Observational Study. J. Clin. Med. 2023, 12, 165. https://doi.org/10.3390/jcm12010165
Huang J-K, Huang S-Y, Lee C-h, Yang I-F, Yang T-F, Wang Y-M. Effect of Age on Heart Rate Variability in Patients with Mitral Valve Prolapse: An Observational Study. Journal of Clinical Medicine. 2023; 12(1):165. https://doi.org/10.3390/jcm12010165
Chicago/Turabian StyleHuang, Jau-Kang, Shiang-Yun Huang, Chih-hsien Lee, Ing-Fang Yang, Ten-Fang Yang, and Yun-Ming Wang. 2023. "Effect of Age on Heart Rate Variability in Patients with Mitral Valve Prolapse: An Observational Study" Journal of Clinical Medicine 12, no. 1: 165. https://doi.org/10.3390/jcm12010165