
Laparoscopic Fluorescence Guided Detection of Uterine Niche—The Next Step in Surgical Diagnosis and Treatment



Abstract
:1. Introduction
2. Materials and Methods
3. Results
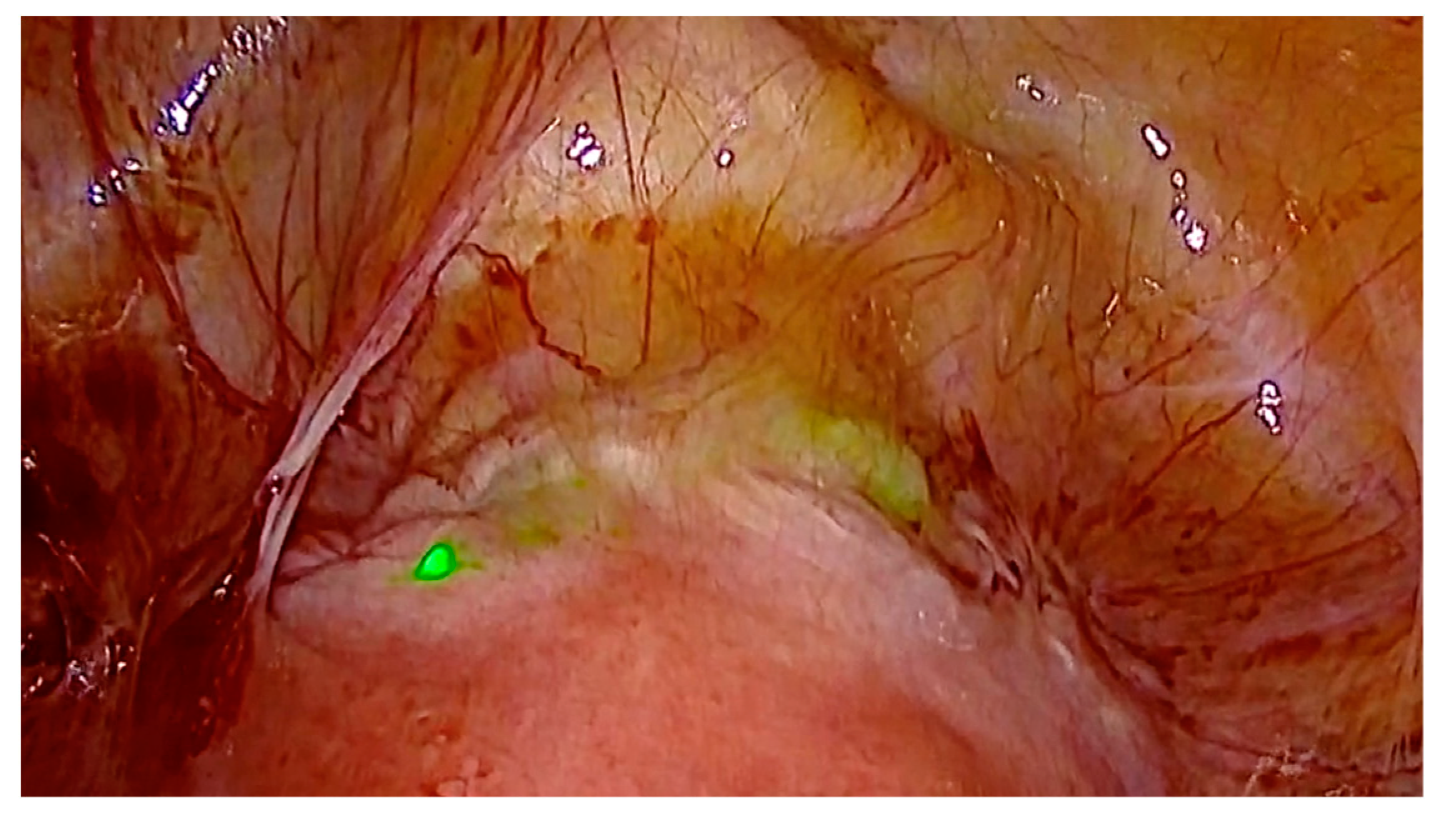
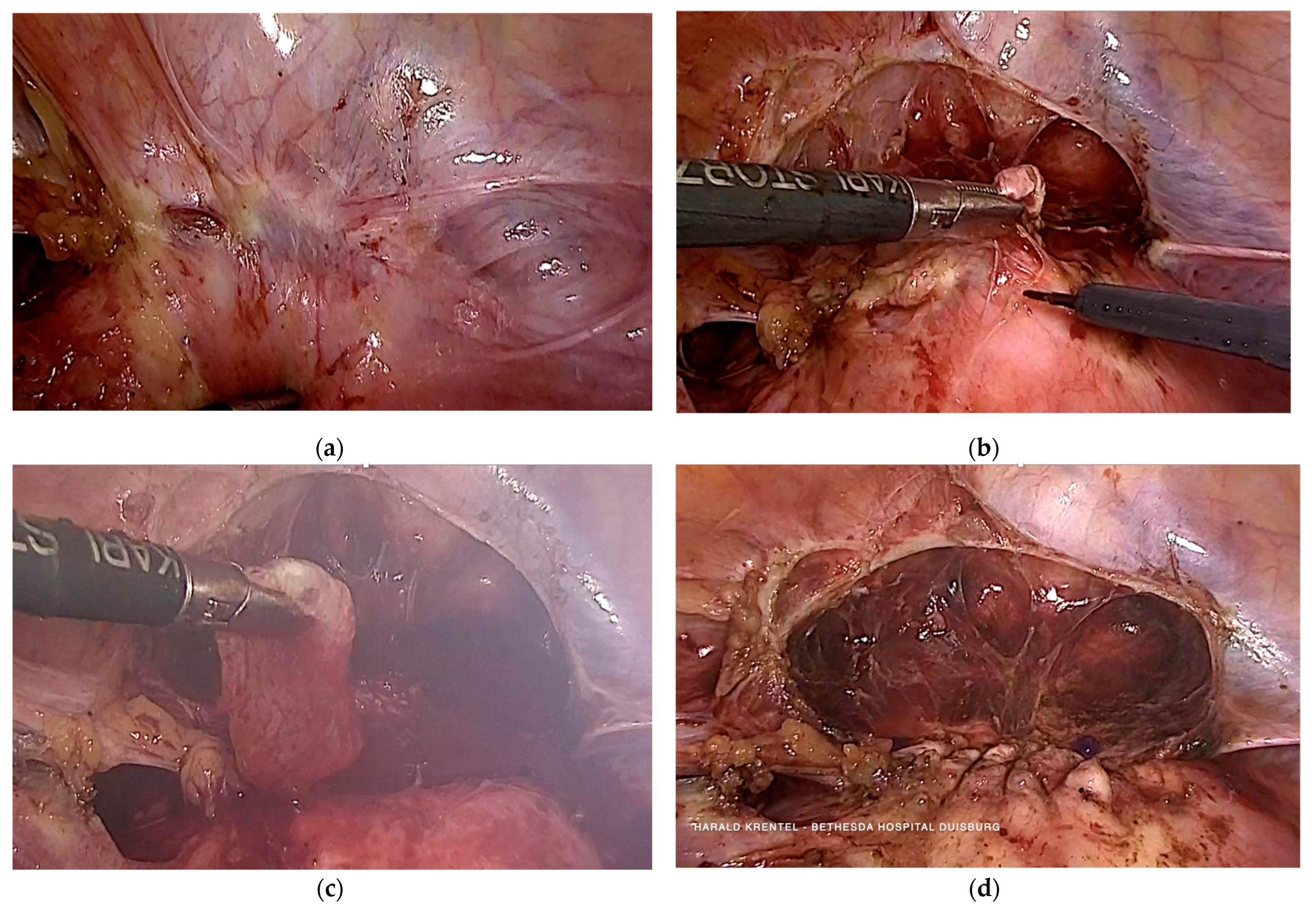
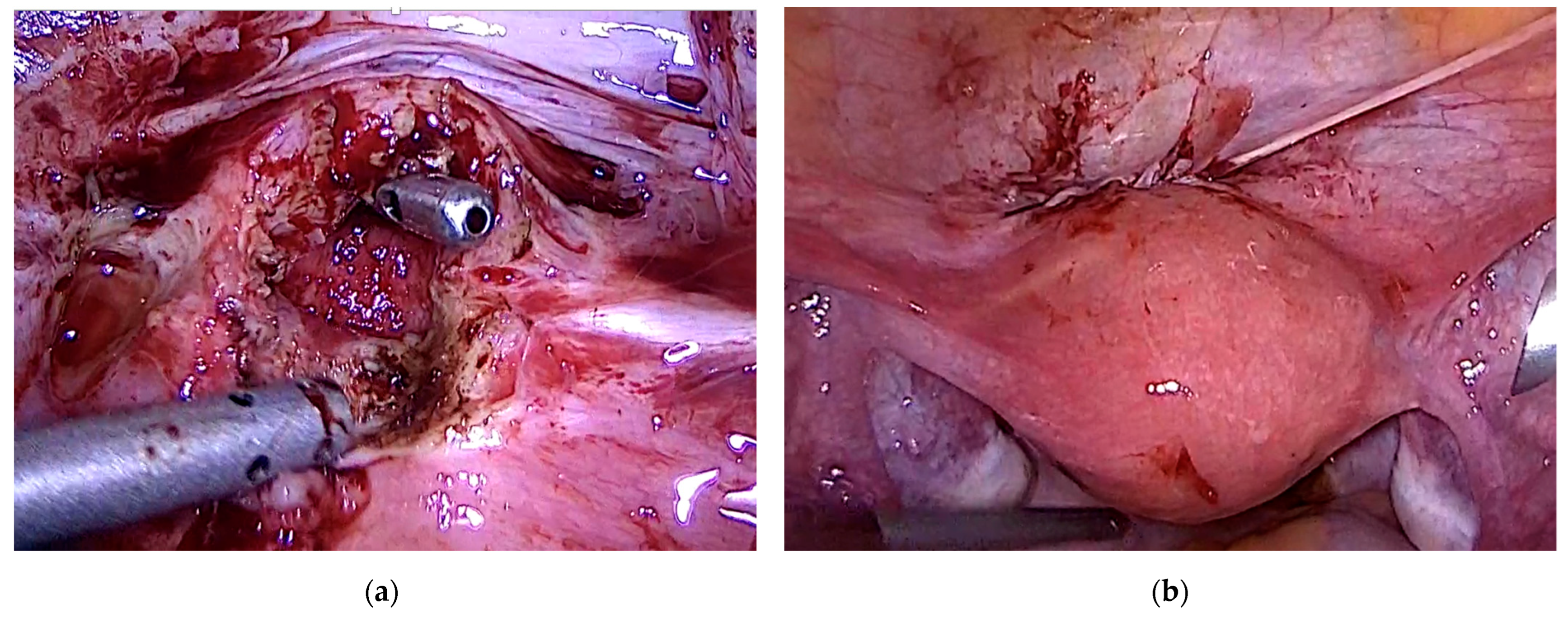
3.1. Case 1—Symptomatic Niche—Laparoscopic Treatment with ICG Niche Detection
3.2. Case 2—Niche Pregnancy—Combined Hysteroscopic and Laparoscopic Treatment
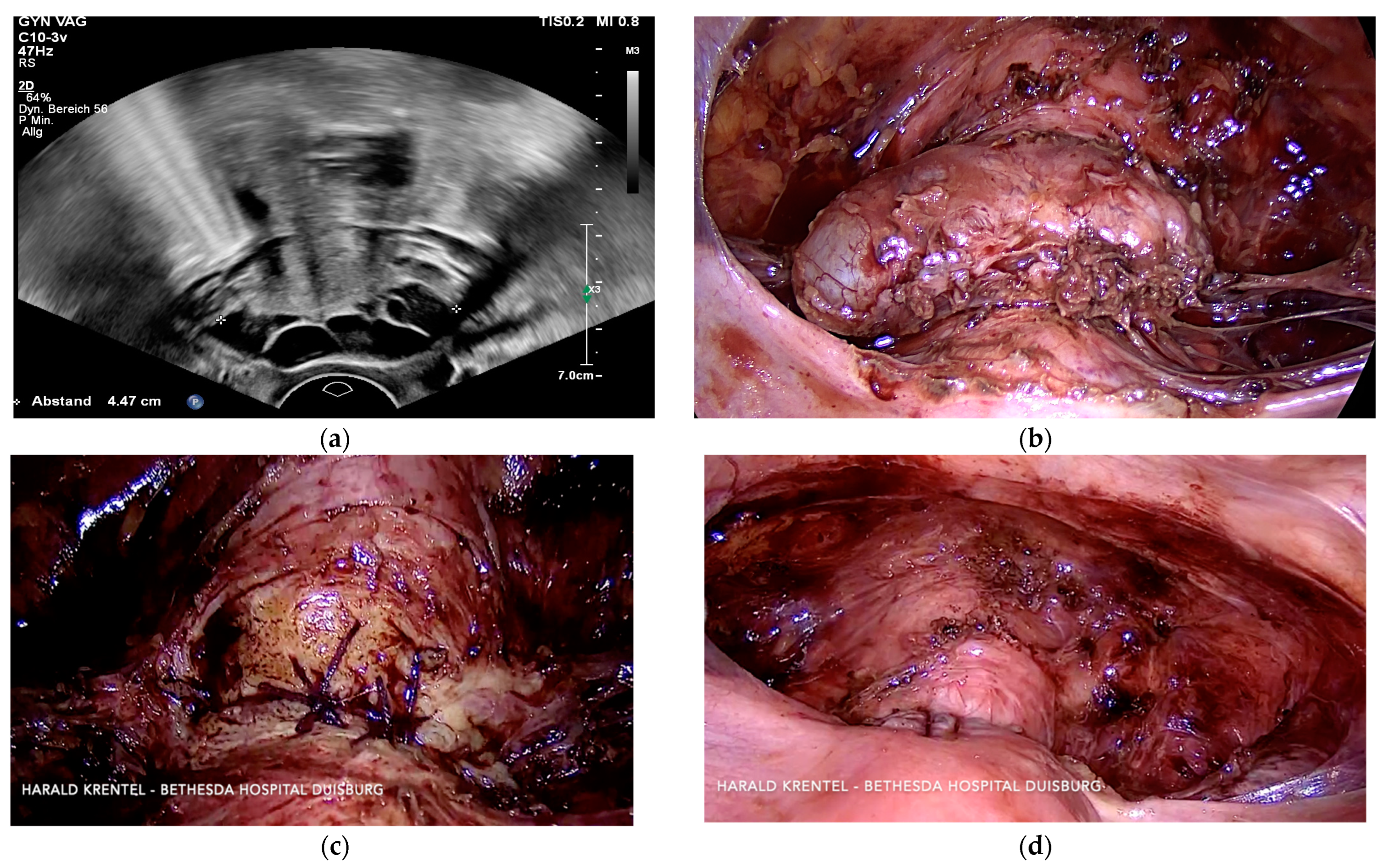
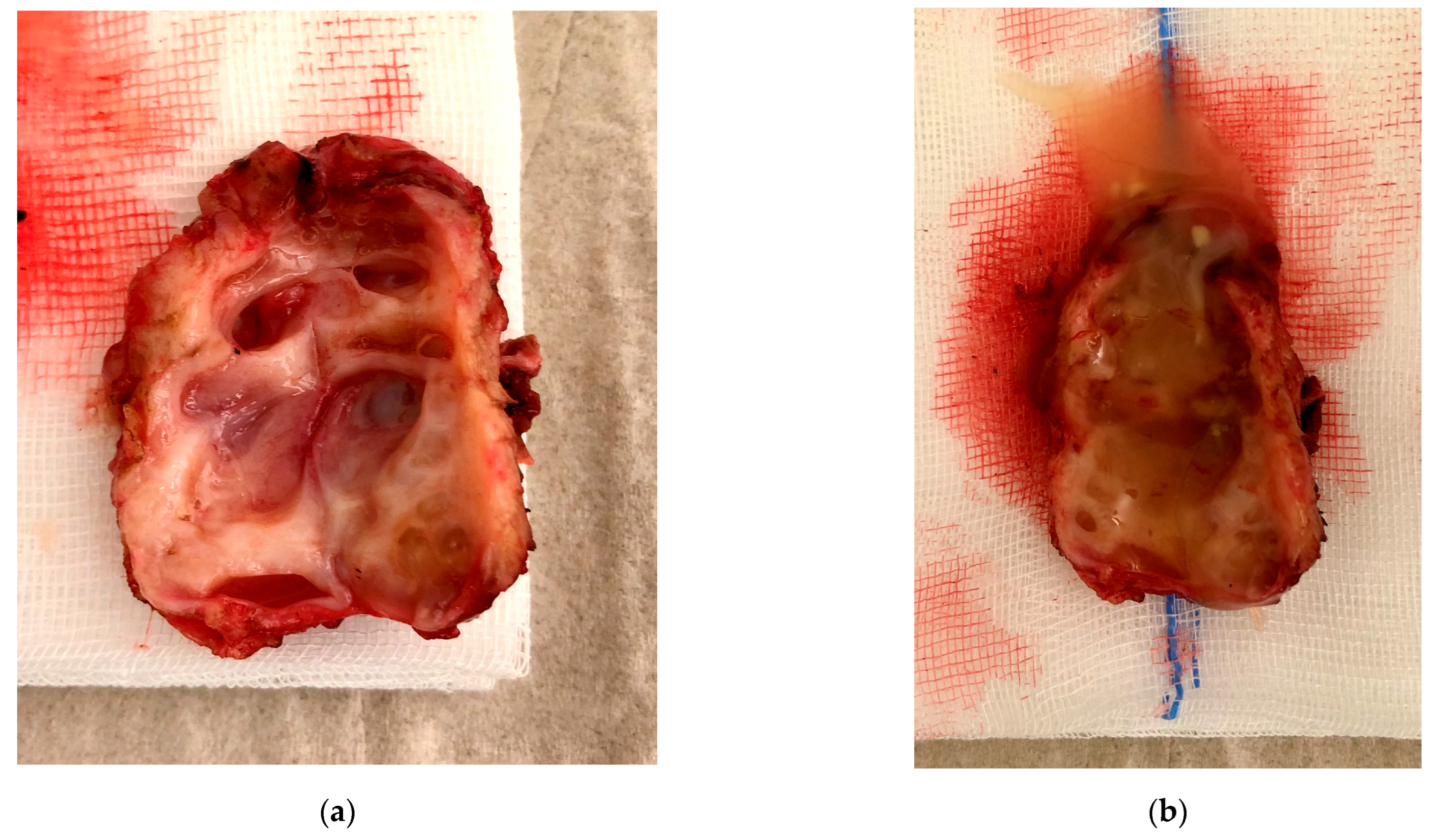
3.3. Case 3—Niche Placentation Failure—Emergency Hysterectomy
3.4. Case 4—Niche Pregnancy—Laparoscopic Subtotal Hysterectomy
3.5. Case 5—Niche Pregnancy—Laparoscopic Resection and Repair
3.6. Case 6—Niche Pregnancy—Combined Hysteroscopic and Laparoscopic Treatment
3.7. Case 7—Symptomatic Niche—Laparoscopic Treatment
3.8. Case 8—Symptomatic Niche—Laparoscopic Treatment
3.9. Case 9 —Symptomatic Isthmozele—Laparoscopic Treatment
4. Discussion
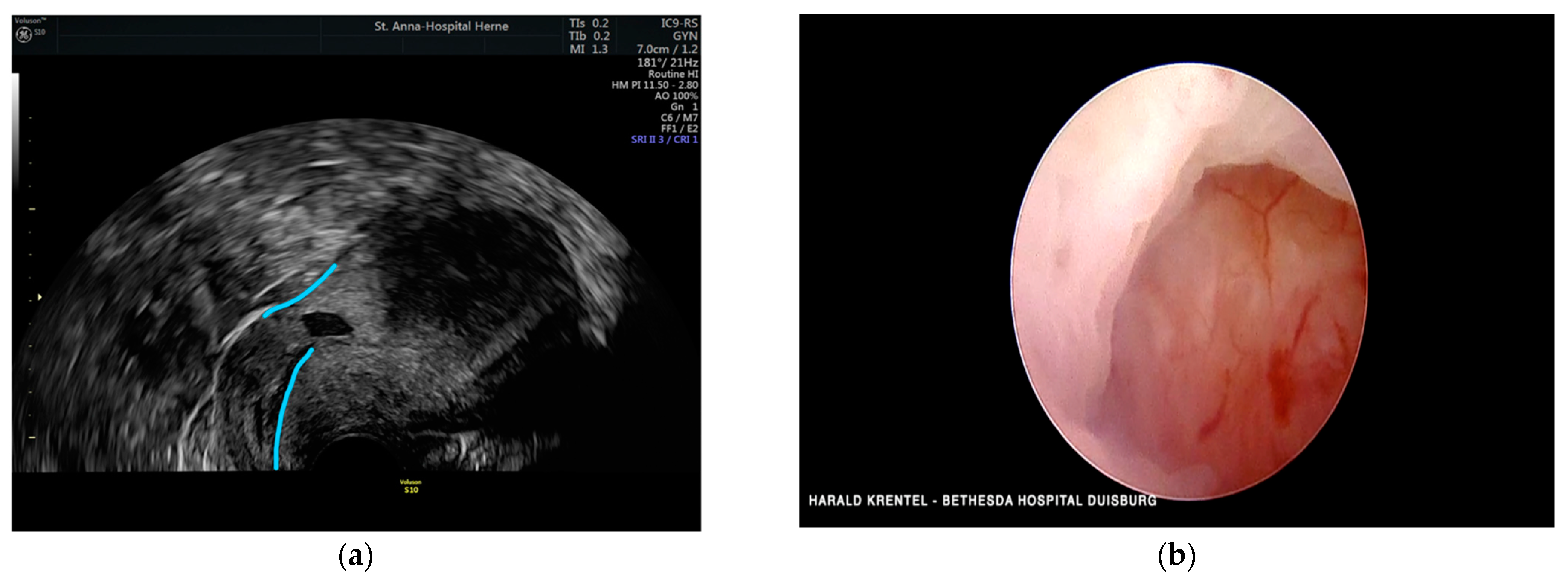
4.1. Niche Detection with Fluorescence Guided Laparoscopy
4.2. Uterine Niche—Is a Treatment Necessary?
4.3. Uterine Niche and Adenomyosis
4.4. Uterine Niche Pregnancy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kulshrestha, V.; Agarwal, N.; Kachhawa, G. Post-Caesarean Niche (Isthmocele) in Uterine Scar: An Update. J. Obstet. Gynaecol. India 2020, 70, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Bij de Vaate, A.J.; van der Voet, L.F.; Naji, O.; Witmer, M.; Veersema, S.; Brölmann, H.A.; Bourne, T.; Huirne, J.A. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: Systematic review. Ultrasound Obstet. Gynecol. 2014, 43, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, C.; Falik, R.; Li, A. Surgical management of niche, isthmocele, uteroperitoneal fistula, or cesarean scar defect: A critical rebirth in the medical literature. Fertil. Steril. 2017, 107, 69–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, M.T.; Osias, J.; Velasco, A.; Charles, R.; Nezhat, C. Laparoscopic repair of a uteroperitoneal fistula. JSLS 2003, 7, 367–369. [Google Scholar] [CrossRef] [Green Version]
- Mashiach, R.; Burke, Y.Z. Optimal Isthmocele Management: Hysteroscopic, Laparoscopic, or Combination. J. Minim. Invasive Gynecol. 2021, 28, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Di Spiezio Sardo, A.; Saccone, G.; McCurdy, R.; Bujold, E.; Bifulco, G.; Berghella, V. Risk of Cesarean scar defect following single- vs. double-layer uterine closure: Systematic review and meta-analysis of randomized controlled trials. Ultrasound Obstet. Gynecol. 2017, 50, 578–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchand, G.J.; Masoud, A.; King, A.; Ruther, S.; Brazil, G.; Ulibarri, H.; Parise, J.; Arroyo, A.; Coriell, C.; Goetz, S.; et al. Effect of single- and double-layer cesarean section closure on residual myometrial thickness and isthmocele—A systematic review and meta-analysis. Turk J. Obstet. Gynecol. 2021, 18, 322–332. [Google Scholar] [CrossRef] [PubMed]
- de Luget, C.D.; Becchis, E.; Fernandez, H.; Donnez, O.; Quarello, E. Can uterine niche be prevented? J. Gynecol. Obstet. Hum. Reprod. 2021, 51, 102299. [Google Scholar] [CrossRef] [PubMed]
- Tanos, V.; Toney, Z.A. Uterine scar rupture—Prediction, prevention, diagnosis, and management. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 59, 115–131. [Google Scholar] [CrossRef] [PubMed]
- Di Spiezio Sardo, A.; Zizolfi, B.; Calagna, G.; Giampaolino, P.; Paolella, F.; Bifulco, G. Hysteroscopic Isthmoplasty: Step-by-Step Technique. J. Minim. Invasive Gynecol. 2018, 25, 338–339. [Google Scholar] [CrossRef] [PubMed]
- Karampelas, S.; Salem Wehbe, G.; de Landsheere, L.; Badr, D.A.; Tebache, L.; Nisolle, M. Laparoscopic Isthmocele Repair: Efficacy and Benefits before and after Subsequent Cesarean Section. J. Clin. Med. 2021, 10, 5785. [Google Scholar] [CrossRef] [PubMed]
- AbdullGaffar, B.; Almulla, A. A Histopathologic Approach to Uterine Niche: What to Expect and to Report in Hysteroscopy-Resected Isthmocele Specimens. Int. J. Surg. Pathol. 2021, 30, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Karpathiou, G.; Chauleur, C.; Dridi, M.; Baillard, P.; Corsini, T.; Dumollard, J.M.; Peoc’H, M. Histologic Findings of Uterine Niches. Am. J. Clin. Pathol. 2020, 154, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Birch Petersen, K.; Hoffmann, E.; Rifbjerg Larsen, C.; Svarre Nielsen, H. Cesarean scar pregnancy: A systematic review of treatment studies. Fertil. Steril. 2016, 105, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maheux-Lacroix, S.; Li, F.; Bujold, E.; Nesbitt-Hawes, E.; Deans, R.; Abbott, J. Cesarean Scar Pregnancies: A Systematic Review of Treatment Options. J. Minim. Invasive Gynecol. 2017, 24, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.L.; Chen, Y.M.; Zeng, W.; Meng, Y.; Jiang, L. Local Methotrexate Injection Followed by Dilation and Curettage for Cesarean Scar Pregnancy: A Prospective Non randomized Study. Front. Med. 2022, 8, 800610. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Cao, Y.; Zhou, L.; Yang, H.; Wu, S.; Li, L. Evaluation of the necessity of laparoscopic repair of a uterine scar defect for cesarean scar pregnancy. J. Int. Med. Res. 2022, 50, 3000605211070753. [Google Scholar] [CrossRef] [PubMed]
- Morlando, M.; Buca, D.; Timor-Tritsch, I.; Cali, G.; Palacios-Jaraquemada, J.; Monteagudo, A.; Khalil, A.; Cennamo, C.; La Manna, V.; Liberati, M.; et al. Reproductive outcome after cesarean scar pregnancy: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2020, 99, 1278–1289. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Number of C-Sections | Niche Related Issue | Treatment | Histopathology of the Niche | |
|---|---|---|---|---|---|
| Case 1 | 34 | 2 | Bleeding disorder, dysuria, dyspareunia | Laparoscopic ICG niche detection and resection | Adenomyosis |
| Case 2 | 31 | 2 | Niche pregnancy, 6 weeks after IVF Pelvic pain and vaginal bleeding | Hysteroscopic resection, second look laparoscopy with scar resection and suture | Chorionic villi, decidua, adenomyosis |
| Case 3 | 40 | 1 | Niche pregnancy with placenta increta and uterine rupture, 13 weeks | Emergency hysterectomy | Placenta praevia, Placenta increta, uterine fibroids, no adenomyosis |
| Case 4 | 39 | 2 | Niche pregnancy, 8 weeks, dysmenorrhea, vaginal bleeding | Subtotal hysterectomy with scar resection (patients wish) | Chorionic villi, decidua, adenomyosis |
| Case 5 | 40 | 3 | Niche pregnancy, 7 weeks of gestation | Laparoscopic resection and repair | Chorionic villi, decidua, no adenomyosis |
| Case 6 | 43 | 1 | Niche pregnancy, 9 weeks, IVF | Hysteroscopic resection second look laparoscopy with resection and repair | Chorionic villi, decidua, no adenomyosis |
| Case 7 | 27 | 1 | Dysmenorrhea and pelvic pain, subfertility | Laparoscopic niche resection and suturing | Adenomyosis |
| Case 8 | 31 | 1 | Bleeding disorder, dysmenorrhea | Laparoscopic niche repair | Adenomyosis |
| Case 9 | 36 | 2 | Large symptomatic isthmocele | Laparoscopic resection and repair | No adenomyosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krentel, H.; Lauterbach, L.-K.; Mavrogiannis, G.; De Wilde, R.L. Laparoscopic Fluorescence Guided Detection of Uterine Niche—The Next Step in Surgical Diagnosis and Treatment. J. Clin. Med. 2022, 11, 2657. https://doi.org/10.3390/jcm11092657
Krentel H, Lauterbach L-K, Mavrogiannis G, De Wilde RL. Laparoscopic Fluorescence Guided Detection of Uterine Niche—The Next Step in Surgical Diagnosis and Treatment. Journal of Clinical Medicine. 2022; 11(9):2657. https://doi.org/10.3390/jcm11092657
Chicago/Turabian StyleKrentel, Harald, Lisa-Kathrin Lauterbach, Georgios Mavrogiannis, and Rudy Leon De Wilde. 2022. "Laparoscopic Fluorescence Guided Detection of Uterine Niche—The Next Step in Surgical Diagnosis and Treatment" Journal of Clinical Medicine 11, no. 9: 2657. https://doi.org/10.3390/jcm11092657