
Correlating Ocular Physiology and Visual Function with Mild Cognitive Loss in Senior Citizens in Taiwan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Subjects
2.2. Research Materials
2.3. Data Analysis and Statistical Analysis
3. Results
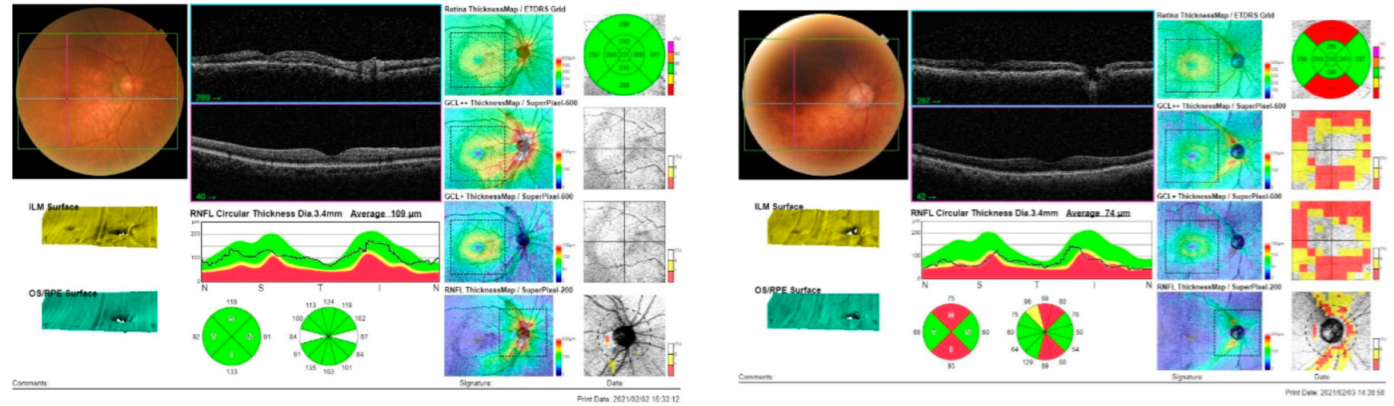
3.1. Ocular Physiology between ACE-Abnormal and ACE-Normal Groups
3.2. Visual Functions between ACE-Abnormal and ACE-Normal Groups
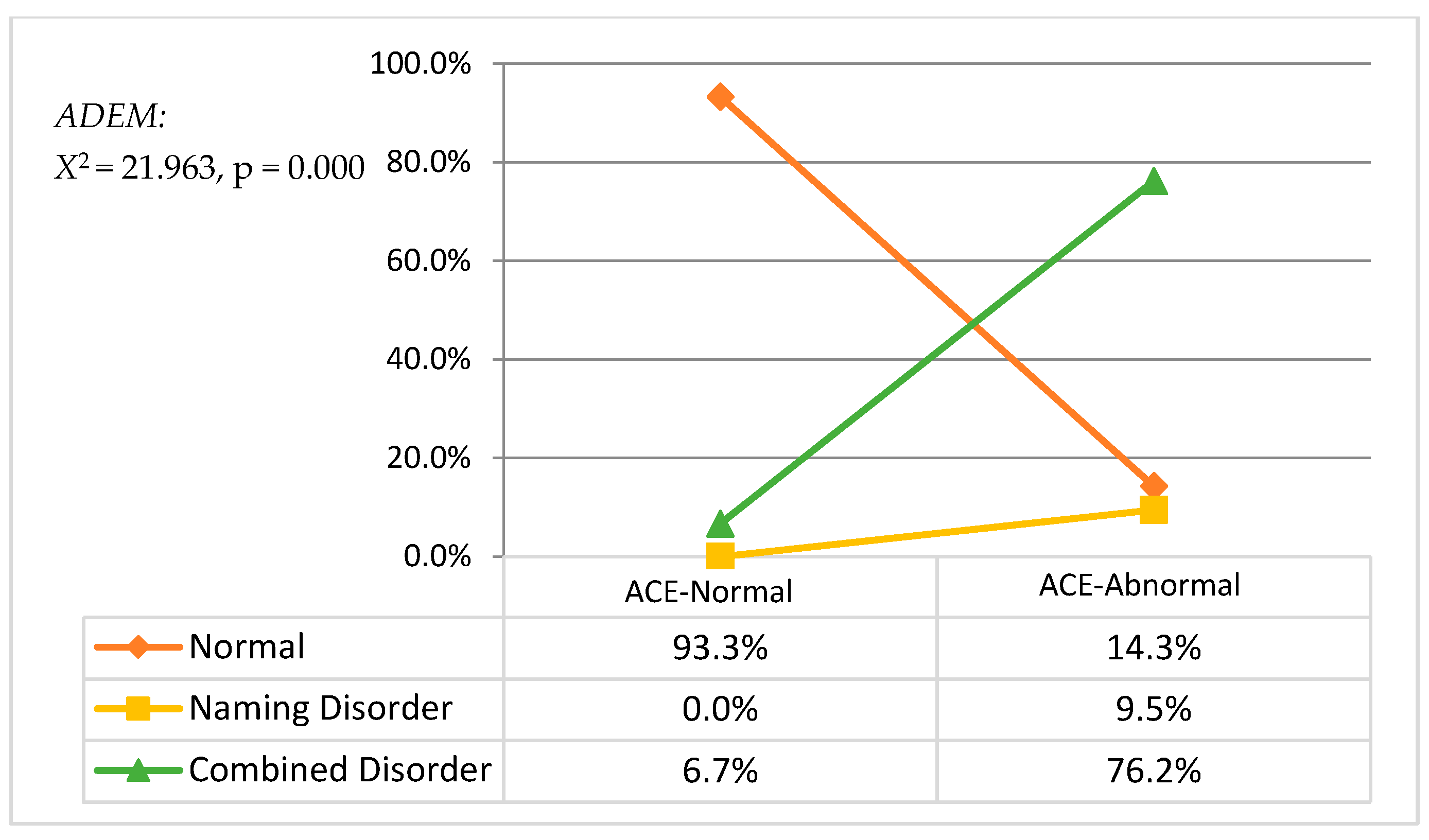
3.2.1. ACE Cognitive Function and ADEM Eye Movement
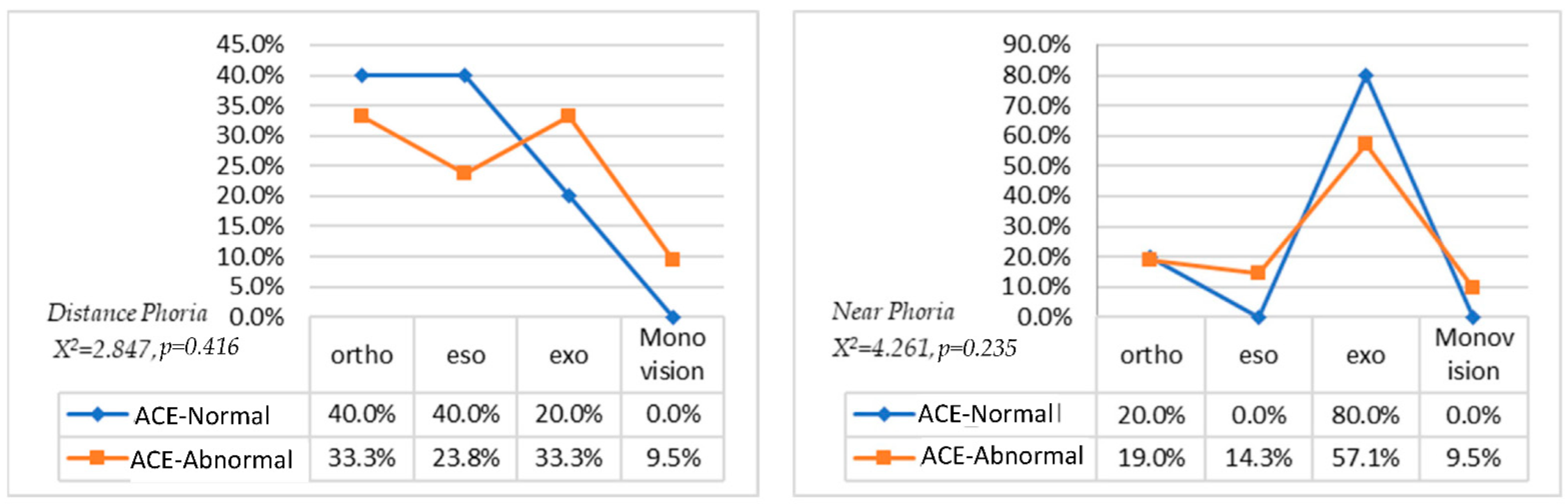
3.2.2. ACE Cognitive Function and Phoria
3.3. Indicator for Cognitive Function
3.3.1. Linear Regression Analysis on Significant Variables
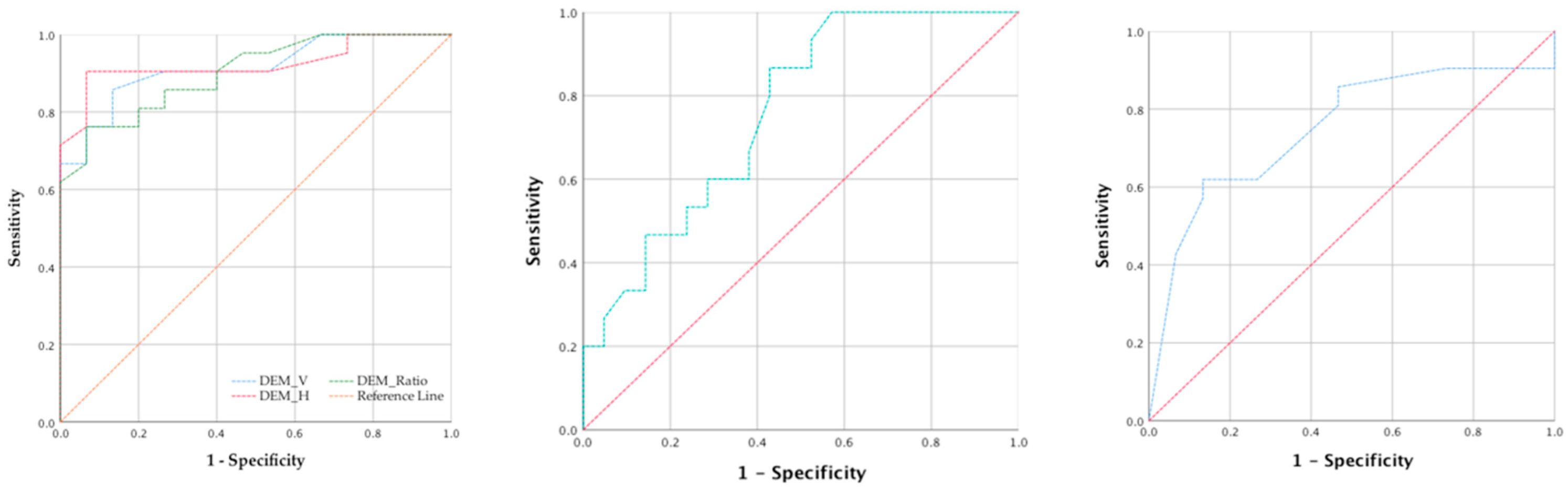
3.3.2. ROC Curve Analysis about Significant Variables
4. Discussion
- In terms of visual physiology, the macular pigment density of the ACE-abnormal group was significantly lower than that of the ACE-normal group, and there was a significant difference in the peripheral thickness of the macular (the superior, inferior, and temporal of the outer macular layer) between the normal and the abnormal groups. Previous studies have indicated that the superior and inferior layers are the most obvious [32] in patients with cognitive impairment. Our results further indicated the outer and inferior macular layers as having excellent discrimination ability in predicting cognitive states under the linear regression and ROC curve. Fundus examination of patients can therefore be used to effectively detect the developing decline of the cognitive state [33,34]. According to the previous studies and the results of this study, we can assume that the thinning of the ganglion cell layer leads to the disappearance of neurons, thereby affecting the dorsal and the ventral pathways; in addition, these neural changes contribute to age-related losses of low-level visual functions and even higher-order visual perceptions, including face perception [35], motion processing [36,37,38], and reading speed [39].
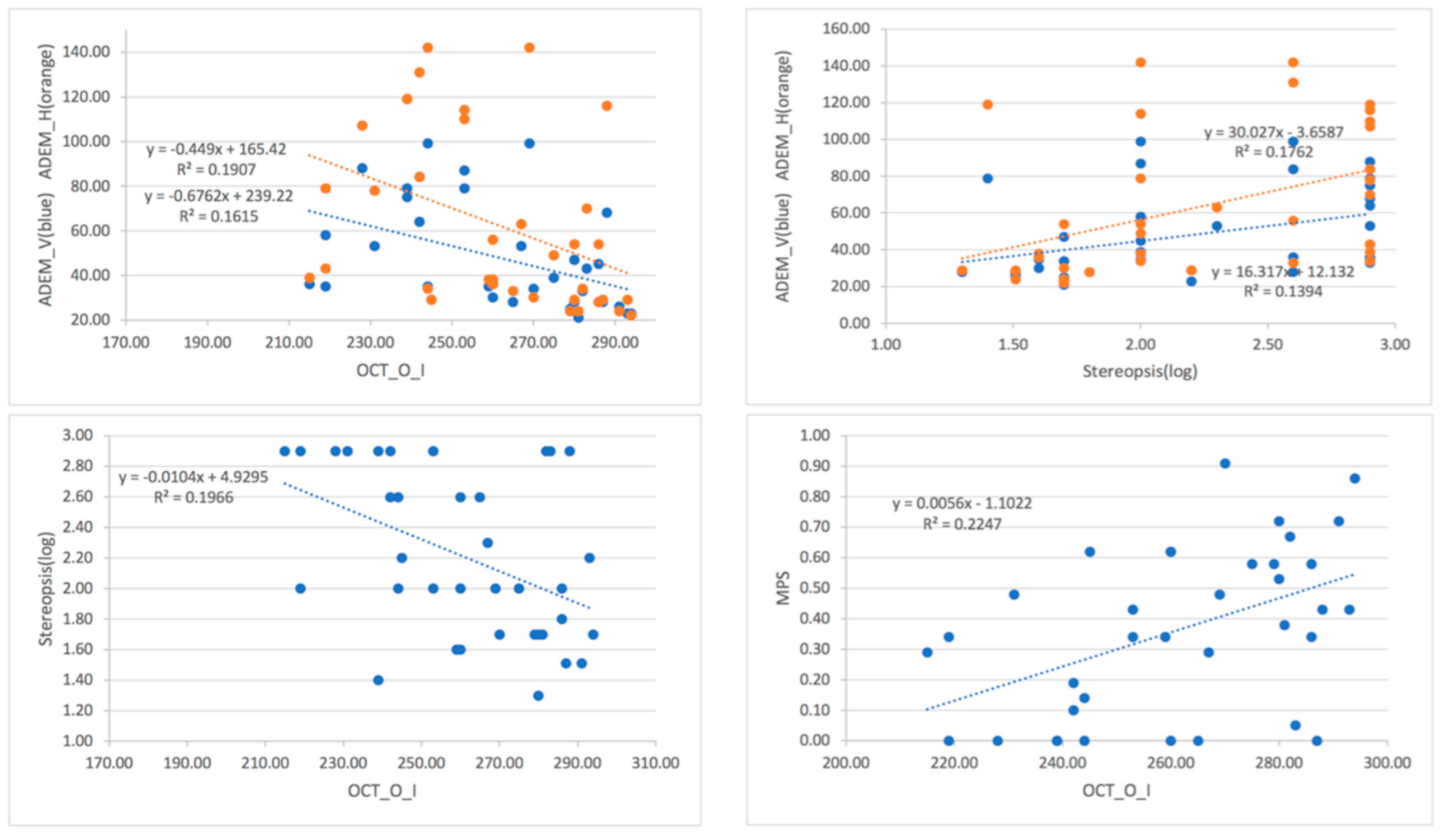
- Moreover, linear regression indicated that ADEM, stereopsis, and macular thinness interact to some extent. For example, ADEM-V, ADEM-H, and stereopsis appeared in the cognitive function of language comprehension and language fluency, presumably because the ADEM measurement can be classified as a group of naming disorders or a combined disorder [25]. When it comes to stereopsis, the reason it is correlated with language comprehension and language fluency might be traced back to the pyramid of binocular vision development [40,41].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kukull, W.-A.; Bowen, J.-D. Dementia epidemiology. Med. Clin. N. Am. 2002, 86, 573–590. [Google Scholar] [CrossRef]
- Guerreiro, R.; Bras, J. The age factor in Alzheimer’s disease. Genome Med. 2015, 7, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crous-Bou, M.; Minguillón, C.; Gramunt, N.; Molinuevo, J.L. Alzheimer’s Disease Prevention: From Risk Factors to Early Intervention. Alzheimer’s Res. Ther. 2017, 9, 71. [Google Scholar] [CrossRef]
- Pirozzolo, F.J.; Hansch, E.C. Oculomotor Reaction Time in Dementia Reflects Degree of Cerebral Dysfunction. Science 1981, 214, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Pelak, V.S. Ocular Motility of Aging and Dementia. Curr. Neurol. Neurosci. Rep. 2010, 10, 440–447. [Google Scholar] [CrossRef]
- Leinonen, H.; Lipponen, A.; Gurevicius, K.; Tanila, H. Normal Amplitude of Electroretinography and Visual Evoked Potential Responses in AβPP/PS1 Mice. J. Alzheimer’s Dis. 2016, 51, 21–26. [Google Scholar] [CrossRef]
- Armstrong, R.A. Alzheimer’s disease and the eye. J. Optom. 2009, 2, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, R.; Kergoat, H. Oculo-visual changes and clinical considerations affecting older patients with dementia. Ophthalmic Physiol. Opt. 2015, 35, 352–376. [Google Scholar] [CrossRef]
- Willard, A.; Lueck, C. Ocular motor disorders. Curr. Opin. Neurol. 2014, 27, 75–82. [Google Scholar] [CrossRef]
- Katz, B.; Rimmer, S. Ophthalmologic manifestations of Alzheimer’s disease. Surv. Ophthalmol. 1989, 34, 31–43. [Google Scholar] [CrossRef]
- Leat, S.J.; Chan, L.L.; Maharaj, P.-D.; Hrynchak, P.K.; Mittelstaedt, A.; Machan, C.M.; Irving, E.L. Binocular Vision and Eye Movement Disorders in Older Adults. Investig. Opthalmol. Vis. Sci. 2013, 54, 3798–3805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaido, M.; Fukui, M.; Kawashima, M.; Negishi, K.; Tsubota, K. Relationship between visual function and cognitive function in the elderly: A cross-sectional observational study. PLoS ONE 2020, 15, e0233381. [Google Scholar] [CrossRef] [PubMed]
- Ikram, M.K.; Cheung, C.Y.; Wong, T.Y.; Chen, C.P. Retinal pathology as biomarker for cognitive impairment and Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2012, 83, 917–922. [Google Scholar] [CrossRef]
- Iseri, P.K.; Altintas, O.; Tokay, T.; Yüksel, N. Relationship between Cognitive Impairment and Retinal Morphological and Visual Functional Abnormalities in Alzheimer Disease. J. Neuro-Ophthalmol. 2006, 26, 18–24. [Google Scholar] [CrossRef]
- Ito, Y.; Sasaki, M.; Takahashi, H.; Nozaki, S.; Matsuguma, S.; Motomura, K.; Ui, R.; Shikimoto, R.; Kawasaki, R.; Yuki, K.; et al. Quantitative Assessment of the Retina Using OCT and Associations with Cognitive Function. Ophthalmology 2020, 127, 107–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenti, D.A. Alzheimer’s disease and glaucoma: Imaging the biomarkers of neurodegenerative disease. Int. J. Alzheimer’s Dis. 2011, 2010, 793931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bambo, M.P.; Garcia-Martin, E.; Pinilla, J.; Herrero, R.; Satue, M.; Otin, S.; Fuertes, I.; Marques, M.L.; Pablo, L.E. Detection of retinal nerve fiber layer degeneration in patients with Alzheimer’s disease using optical coherence tomography: Searching new biomarkers. Acta Ophthalmol. 2014, 92, e581–e582. [Google Scholar] [CrossRef]
- Johnson, E.J. A possible role for lutein and zeaxanthin in cognitive function in the elderly. Am. J. Clin. Nutr. 2012, 96, 1161S–1165S. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-I.; Kang, B.-H. Decreased retinal thickness in patients with Alzheimer’s disease is correlated with disease severity. PLoS ONE 2019, 14, e0224180. [Google Scholar] [CrossRef] [Green Version]
- Paquet, C.; Boissonnot, M.; Roger, F.; Dighiero, P.; Gil, R.; Hugon, J. Abnormal retinal thickness in patients with mild cognitive impairment and Alzheimer’s disease. Neurosci. Lett. 2007, 420, 97–99. [Google Scholar] [CrossRef]
- Sunjic-Alic, A.; Zebenholzer, K.; Gall, W. Reporting of Studies Conducted on Austrian Claims Data. In Navigating Healthcare Through Challenging Times; IOS Press: Amsterdam, The Netherlands, 2021; pp. 62–69. [Google Scholar]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Bruno, D.; Schurmann Vignaga, S. Addenbrooke’s cognitive examination III in the diagnosis of dementia: A critical review. Neuropsychiatr. Dis. Treat. 2019, 15, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Sampredo, A.; Richman, J.; Pardo, M.J. The adult developmental eye movement test (A-DEM): A tool for saccadic evaluation in adults. J. Behav. Optom. 2003, 4, 1–5. [Google Scholar]
- Garzia, R.P.; Richman, J.E.; Nicholson, S.B.; Gaines, C.S. A new visual-verbal saccade test: The Developmental Eye Movement test (DEM). J. Am. Optom. Assoc. 1990, 61, 124–135. [Google Scholar] [PubMed]
- Suchoff, I.B.; Kapoor, N.; Waxman, R.; Ference, W. The occurrence of ocular and visual dysfunctions in an acquired brain-injured patient sample. J. Am. Optom. Assoc. 1999, 70, 301–308. [Google Scholar] [PubMed]
- Sampedro, A.G.; Richman, J.E.; Pardo, M.S. The Adult Developmental Eye Movement Test (A–DEM). J. Behav. Optom. 2003, 14, 101–105. [Google Scholar]
- Gené-Sampedro, A.; Monteiro, P.M.L.; Bueno-Gimeno, I.; Gene-Morales, J.; Piñero, D.P. Validation of a modified version of the adult developmental eye movement test. Sci. Rep. 2021, 11, 19759. [Google Scholar] [CrossRef]
- Stringham, J.M.; Garcia, P.V.; Smith, P.A.; McLin, L.N.; Foutch, B.K. Macular Pigment and Visual Performance in Glare: Benefits for Photostress Recovery, Disability Glare, and Visual Discomfort. Investig. Opthalmol. Vis. Sci. 2011, 52, 7406–7415. [Google Scholar] [CrossRef] [Green Version]
- Hammond, B.R.; Fletcher, L.M.; Elliott, J.G. Glare Disability, Photostress Recovery, and Chromatic Contrast: Relation to Macular Pigment and Serum Lutein and Zeaxanthin. Investig. Opthalmol. Vis. Sci. 2013, 54, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.W.; Su, K.C.; Lu, F.C.; Cheng, H.M.; Cheng, C.Y. Visual Function and Visual Perception among Senior Citizens with Mild Cognitive Impairment in Taiwan. Healthcare 2022, 10, 20. [Google Scholar] [CrossRef]
- Murueta-Goyena, A.; Del Pino, R.; Galdós, M.; Arana, B.; Acera, M.; Carmona-Abellán, M.; Fernández-Valle, T.; Tijero, B.; Lucas-Jiménez, O.; Ojeda, N.; et al. Retinal Thickness Predicts the Risk of Cognitive Decline in Parkinson Disease. Ann. Neurol. 2021, 89, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Cunha, L.P.; Lopes, L.C.; Costa-Cunha, L.V.; Costa, C.F.; Pires, L.A.; Almeida, A.L.; Monteiro, M.L. Macular Thickness Measurements with Frequency Domain-OCT for Quantification of Retinal Neural Loss and its Correlation with Cognitive Impairment in Alzheimer’s Disease. PLoS ONE 2016, 11, e0153830. [Google Scholar]
- Mammadova, N.; Neppl, T.K.; Denburg, N.L.; West Greenlee, M.H. Reduced Retinal Thickness Predicts Age-Related Changes in Cognitive Function. Front. Aging Neurosci. 2020, 12, 81. [Google Scholar] [CrossRef] [Green Version]
- Konar, Y.; Bennett, P.J.; Sekuler, A.B. Effects of aging on face identification and holistic face processing. Vis. Res. 2013, 88, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Bennett, P.J.; Sekuler, R.; Sekuler, A.B. The effects of aging on motion detection and direction identification. Vis. Res. 2007, 47, 799–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betts, L.R.; Taylor, C.P.; Sekuler, A.B.; Bennett, P.J. Aging reduces center-surround antagonism in visual motion pro-cessing. Neuron 2005, 45, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, R.; Monacelli, A.; Duffy, C.J. Visual Motion Event Related Potentials Distinguish Aging and Alzheimer’s Disease. J. Alzheimer’s Dis. 2013, 36, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Owsley, C. Aging and vision. Vis. Res. 2011, 51, 1610–1622. [Google Scholar] [CrossRef] [Green Version]
- Scheiman, M.; Wick, B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Xi, J.; Jia, W.-L.; Feng, L.-X.; Lu, Z.-L.; Huang, C.-B. Perceptual Learning Improves Stereoacuity in Amblyopia. Investig. Opthalmol. Vis. Sci. 2014, 55, 2384–2391. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ACE-Abnormal N = 21/M (SD) | ACE-Normal N = 15/M (SD) | Levene F Value | t | p | |
|---|---|---|---|---|---|
| ACE Total score | 63.00 (12.64) | 88.93 (3.51) | 19.24 | −8.93 | 0.000 ** |
| ACE Attention | 13.57 (3.71) | 17.40 (0.91) | 19.21 | −4.54 | 0.000 ** |
| ACE Memory | 14.05 (2.78) | 22.60 (2.20) | 0.07 | −9.89 | 0.000 ** |
| ACE Language fluency | 5.14 (2.73) | 9.33 (1.99) | 2.66 | −5.06 | 0.000 ** |
| ACE Language comprehension | 19.95 (4.40) | 25.13 (0.83) | 20.53 | −5.27 | 0.000 ** |
| ACE Visuospatial | 10.29 (2.24) | 14.47 (1.19) | 4.03 | −6.58 | 0.000 ** |
| ACE-Abnormal N = 21/M (SD) | ACE-Normal N = 15/M (SD) | Levene F Value | t | p | |
|---|---|---|---|---|---|
| MPS | 0.27 (0.22) | 0.49(0.30) | 1.17 | −2.50 | 0.02 * |
| OCT-Center-Fovea | 250.05 (35.55) | 257.07(26.01) | 0.11 | −0.65 | 0.52 |
| OCT-Inner-Temporal | 296.52 (27.12) | 311.40(18.63) | 1.74 | −1.83 | 0.08 |
| OCT-Inner-Superior | 305.52 (27.79) | 330.00(20.04) | 1.23 | −2.91 | 0.01 * |
| OCT-Inner-Nasal | 310.29 (26.84) | 324.93(24.54) | 0.10 | −1.67 | 0.10 |
| OCT-Inner-Inferior | 301.14 (24.63) | 320.53(18.30) | 0.74 | −2.58 | 0.01 ** |
| OCT-Outer-Temporal | 251.00 (32.74) | 270.40(13.55) | 4.84 | −2.44 | 0.02 * |
| OCT-Outer-Superior | 260.15 (34.32) | 293.13(24.52) | 1.85 | −3.16 | 0.003 ** |
| OCT-Outer-Nasal | 278.38 (26.63) | 307.13(16.32) | 2.96 | −3.70 | 0.001 ** |
| OCT-Outer-Inferior | 252.95 (23.70) | 273.07(16.78) | 2.73 | −2.82 | 0.008 ** |
| ACE-Abnormal N = 21/M (SD) | ACE-Normal N = 15/M (SD) | Levene F Value | t | p | |
|---|---|---|---|---|---|
| ADEM_V | 60.86 (23.42) | 30.20 (6.50) | 27.51 | 5.70 | 0.000 ** |
| ADEM_H | 84.38 (37.41) | 31.87 (8.03) | 33.45 | 6.24 | 0.000 ** |
| ADEM_Ratio | 1.35 (0.20) | 1.06 (0.12) | 5.07 | 5.63 | 0.000 ** |
| Stereo | 2.40 (0.55) | 1.93 (0.41) | 4.23 | 2.95 | 0.006 ** |
| Contrast sensitivity | 1.37 (0.38) | 1.25 (0.00) | 7.45 | 1.45 | 0.16 |
| Dependent Variables | R | R2 | Adjusted R2 | SE | Change Value | F | Sig. | |||
|---|---|---|---|---|---|---|---|---|---|---|
| R2 Change | F Change | p for F Change | ||||||||
| ACE total score | 1. ADEM-H | 0.841 | 0.707 | 0.698 | 9.03 | 0.707 | 79.638 | 0.000 | 79.638 | 0.000 ** |
| 2. 1 + Stereopsis | 0.890 | 0.792 | 0.779 | 7.72 | 0.085 | 13.158 | 0.001 | 61.069 | 0.000 ** | |
| 3. 2 + OCT-O-I | 0.906 | 0.821 | 0.804 | 7.29 | 0.029 | 4.946 | 0.034 | 47.382 | 0.000 ** | |
| ACE attention | 1. ADEM-V | 0.824 | 0.679 | 0.670 | 2.00 | 0.679 | 69.930 | 0.000 | 69.930 | 0.000 ** |
| 2. 1 + OCT-O-I | 0.846 | 0.716 | 0.699 | 1.91 | 0.037 | 4.178 | 0.049 | 40.422 | 0.000 ** | |
| ACE memory | 1. ADEM-Ratio | 0.825 | 0.681 | 0.672 | 2.85 | 0.681 | 70.564 | 0.000 | 70.564 | 0.000 ** |
| 2. 1 + OCT-O-I | 0.900 | 0.810 | 0.698 | 2.23 | 0.129 | 21.633 | 0.000 | 68.159 | 0.000 ** | |
| ACE language fluency | 1. ADEM-H | 0.674 | 0.455 | 0.438 | 2.35 | 0.455 | 27.538 | 0.000 | 27.538 | 0.000 ** |
| 2. 1 + Stereopsis | 0.745 | 0.555 | 0.528 | 2.15 | 0.101 | 7.238 | 0.011 | 19.990 | 0.000 ** | |
| ACE language | 1. ADEM-V | 0.777 | 0.603 | 0.591 | 2.75 | 0.603 | 50.216 | 0.000 | 50.216 | 0.000 ** |
| 2. 1 + Stereopsis | 0.825 | 0.681 | 0.661 | 2.51 | 0.077 | 7.729 | 0.009 | 34.092 | 0.000 ** | |
| ACE visuospatial | 1. ADEM-H | 0.662 | 0.438 | 0.421 | 2.16 | 0.438 | 25.721 | 0.000 | 25.721 | 0.000 ** |
| Variable | AUC | SE | p | 95%CI | Sensitivity | Specificity | Cut-Off Point | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| ADEM_V | 0.914 | 0.047 | 0.000 ** | 0.823 | 1.00 | 0.857 | 0.867 | 35.5 |
| ADEM_H | 0.924 | 0.047 | 0.000 ** | 0.831 | 1.00 | 0.905 | 0.933 | 38.5 |
| ADEM_Ratio | 0.902 | 0.049 | 0.000 ** | 0.806 | 0.997 | 0.762 | 0.933 | 1.21 |
| OCT_O_I | 0.795 | 0.079 | 0.009 ** | 0.604 | 0.913 | 1 | 0.429 | 243 |
| Stereopsis | 0.794 | 0.084 | 0.012 * | 0.585 | 0.913 | 0.857 | 0.733 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, K.-C.; Cheng, H.-M.; Chu, Y.; Lu, F.-C.; Tsai, L.-H.; Cheng, C.-Y. Correlating Ocular Physiology and Visual Function with Mild Cognitive Loss in Senior Citizens in Taiwan. J. Clin. Med. 2022, 11, 2624. https://doi.org/10.3390/jcm11092624
Su K-C, Cheng H-M, Chu Y, Lu F-C, Tsai L-H, Cheng C-Y. Correlating Ocular Physiology and Visual Function with Mild Cognitive Loss in Senior Citizens in Taiwan. Journal of Clinical Medicine. 2022; 11(9):2624. https://doi.org/10.3390/jcm11092624
Chicago/Turabian StyleSu, Kuo-Chen, Hong-Ming Cheng, Yu Chu, Fang-Chun Lu, Lung-Hui Tsai, and Ching-Ying Cheng. 2022. "Correlating Ocular Physiology and Visual Function with Mild Cognitive Loss in Senior Citizens in Taiwan" Journal of Clinical Medicine 11, no. 9: 2624. https://doi.org/10.3390/jcm11092624