
Impact of Renal Replacement Therapy on Mortality and Renal Outcomes in Critically Ill Patients with Acute Kidney Injury: A Population-Based Cohort Study in Korea between 2008 and 2015

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
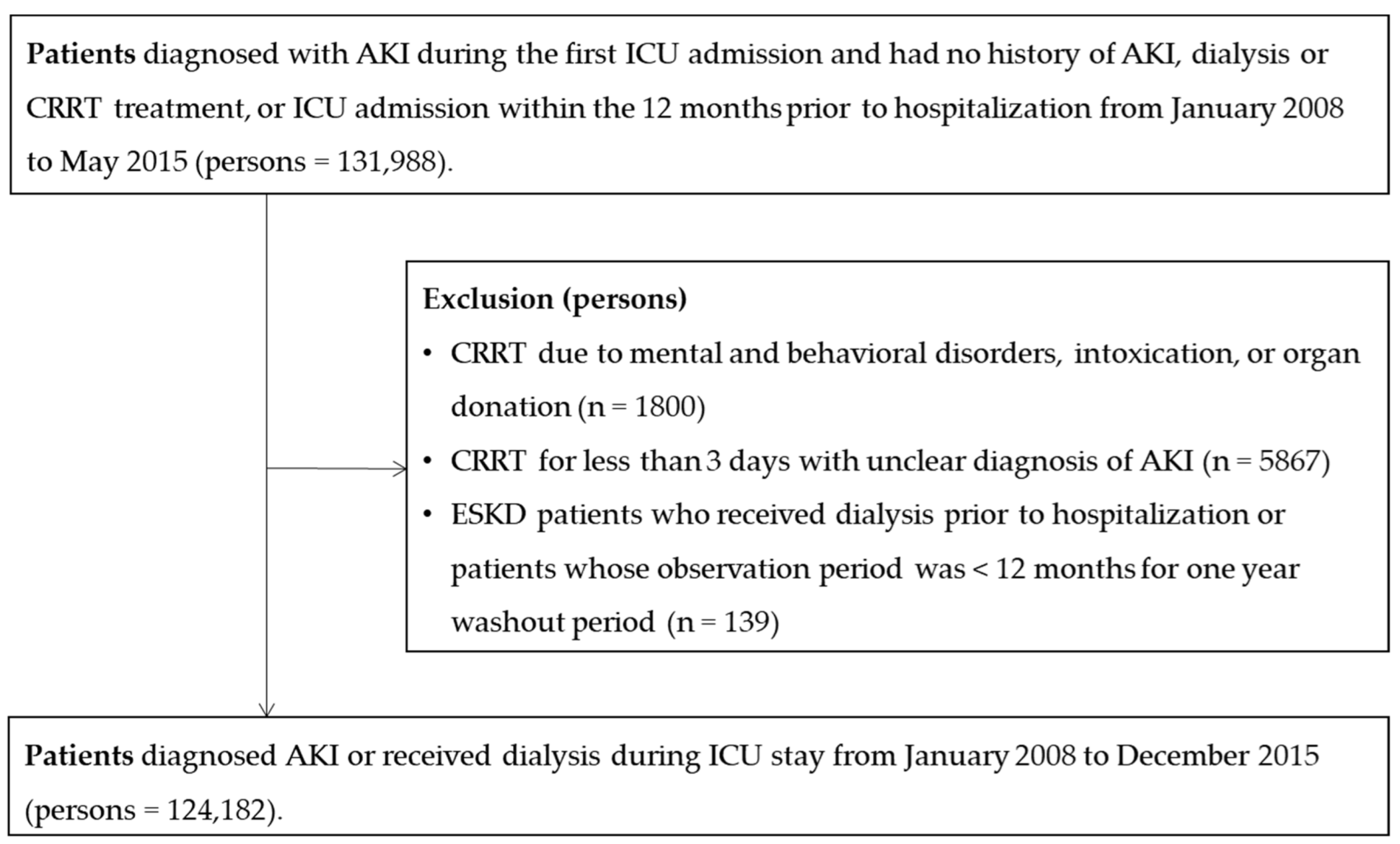
2.2. Study Population
2.3. Study Variables
2.4. Definition of Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liborio, A.B.; Leite, T.T.; Neves, F.M.; Teles, F.; Bezerra, C.T. AKI complications in critically ill patients: Association with mortality rates and RRT. Clin. J. Am. Soc. Nephrol. 2015, 10, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Elseviers, M.M.; Lins, R.L.; Van der Niepen, P.; Hoste, E.; Malbrain, M.L.; Damas, P.; Devriendt, J.; the SHARF Investigators. Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury. Crit. Care 2010, 14, R221. [Google Scholar] [CrossRef] [Green Version]
- Siew, E.D.; Davenport, A. The growth of acute kidney injury: A rising tide or just closer attention to detail? Kidney Int. 2015, 87, 46–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, L.; Wei, Q.; Liu, J.; Yi, M.; Liu, Y.; Liu, H.; Sun, L.; Peng, Y.; Liu, F.; Venkatachalam, M.A.; et al. AKI on CKD: Heightened injury, suppressed repair, and the underlying mechanisms. Kidney Int. 2017, 92, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- An, J.N.; Hwang, J.H.; Kim, D.K.; Lee, H.; Ahn, S.Y.; Kim, S.; Park, J.T.; Kang, S.W.; Oh, Y.K.; Kim, Y.S.; et al. Chronic Kidney Disease After Acute Kidney Injury Requiring Continuous Renal Replacement Therapy and Its Impact on Long-Term Outcomes: A Multicenter Retrospective Cohort Study in Korea. Crit. Care Med. 2017, 45, 47–57. [Google Scholar] [CrossRef]
- Stads, S.; Fortrie, G.; van Bommel, J.; Zietse, R.; Betjes, M.G. Impaired kidney function at hospital discharge and long-term renal and overall survival in patients who received CRRT. Clin. J. Am. Soc. Nephrol. 2013, 8, 1284–1291. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Jeon, K.; Chung, C.R.; Yang, J.H.; Cho, Y.H.; Cho, J.; Park, C.M.; Park, H.; Cho, J.; Guallar, E.; et al. A nationwide analysis of intensive care unit admissions, 2009–2014—The Korean ICU National Data (KIND) study. J. Crit. Care 2018, 44, 24–30. [Google Scholar] [CrossRef]
- Kim, J.A.; Yoon, S.; Kim, L.Y.; Kim, D.S. Towards Actualizing the Value Potential of Korea Health Insurance Review and Assessment (HIRA) Data as a Resource for Health Research: Strengths, Limitations, Applications, and Strategies for Optimal Use of HIRA Data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef]
- Lee, Y.S.; Lee, Y.R.; Chae, Y.; Park, S.Y.; Oh, I.H.; Jang, B.H. Translation of Korean Medicine Use to ICD-Codes Using National Health Insurance Service-National Sample Cohort. Evid. Based Complement. Alternat. Med. 2016, 2016, 8160838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagshaw, S.M.; Wald, R. Strategies for the optimal timing to start renal replacement therapy in critically ill patients with acute kidney injury. Kidney Int. 2017, 91, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Kdigo, A. Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kim, K.H. Comparative study on three algorithms of the ICD-10 Charlson comorbidity index with myocardial infarction patients. J. Prev. Med. Public Health 2010, 43, 42–49. [Google Scholar] [CrossRef]
- Morgan, J.H.; Kallen, M.A.; Okike, K.; Lee, O.C.; Vrahas, M.S. PROMIS Physical Function Computer Adaptive Test Compared With Other Upper Extremity Outcome Measures in the Evaluation of Proximal Humerus Fractures in Patients Older Than 60 Years. J. Orthop. Trauma 2015, 29, 257–263. [Google Scholar] [CrossRef]
- Overbeek, C.L.; Nota, S.P.; Jayakumar, P.; Hageman, M.G.; Ring, D. The PROMIS physical function correlates with the QuickDASH in patients with upper extremity illness. Clin. Orthop. Relat. Res. 2015, 473, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Shulman, L.N.; Palis, B.E.; McCabe, R.M.; Gay, E.G.; Mallin, K.; Loomis, A.; Winchester, D.P.; McKellar, D.P. Survival as a measure of quality of cancer care and advances in therapy: Lessons learned from analyses of the National Cancer Data Base (NCDB). J. Clin. Oncol. 2016, 34, 173. [Google Scholar] [CrossRef]
- Vinsonneau, C.; Camus, C.; Combes, A.; Costa de Beauregard, M.A.; Klouche, K.; Boulain, T.; Pallot, J.L.; Chiche, J.D.; Taupin, P.; Landais, P.; et al. Continuous venovenous haemodiafiltration versus intermittent haemodialysis for acute renal failure in patients with multiple-organ dysfunction syndrome: A multicentre randomised trial. Lancet 2006, 368, 379–385. [Google Scholar] [CrossRef]
- Lins, R.L.; Elseviers, M.M.; Van der Niepen, P.; Hoste, E.; Malbrain, M.L.; Damas, P.; Devriendt, J.; the SHARF Investigators. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: Results of a randomized clinical trial. Nephrol. Dial. Transpl. 2009, 24, 512–518. [Google Scholar] [CrossRef] [Green Version]
- Gaudry, S.; Grolleau, F.; Barbar, S.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Montini, F.; Bohe, J.; et al. Continuous renal replacement therapy versus intermittent hemodialysis as first modality for renal replacement therapy in severe acute kidney injury: A secondary analysis of AKIKI and IDEAL-ICU studies. Crit Care 2022, 26, 93. [Google Scholar] [CrossRef] [PubMed]
- Pannu, N.; Klarenbach, S.; Wiebe, N.; Manns, B.; Tonelli, M.; Alberta Kidney Disease, N. Renal replacement therapy in patients with acute renal failure: A systematic review. JAMA 2008, 299, 793–805. [Google Scholar] [CrossRef] [PubMed]
- Nash, D.M.; Przech, S.; Wald, R.; O’Reilly, D. Systematic review and meta-analysis of renal replacement therapy modalities for acute kidney injury in the intensive care unit. J. Crit. Care 2017, 41, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Wald, R.; Shariff, S.Z.; Adhikari, N.K.; Bagshaw, S.M.; Burns, K.E.; Friedrich, J.O.; Garg, A.X.; Harel, Z.; Kitchlu, A.; Ray, J.G. The association between renal replacement therapy modality and long-term outcomes among critically ill adults with acute kidney injury: A retrospective cohort study*. Crit. Care Med. 2014, 42, 868–877. [Google Scholar] [CrossRef]
- De Corte, W.; Dhondt, A.; Vanholder, R.; De Waele, J.; Decruyenaere, J.; Sergoyne, V.; Vanhalst, J.; Claus, S.; Hoste, E.A. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: A prospective cohort study. Crit. Care 2016, 20, 256. [Google Scholar] [CrossRef] [Green Version]
- Khosla, N.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.; Mehta, R.L.; Program to Improve Care in Acute Renal Disease. Preexisting chronic kidney disease: A potential for improved outcomes from acute kidney injury. Clin. J. Am. Soc. Nephrol. 2009, 4, 1914–1919. [Google Scholar] [CrossRef] [Green Version]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syndromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef]
- Zarbock, A.; Kellum, J.A.; Schmidt, C.; Van Aken, H.; Wempe, C.; Pavenstadt, H.; Boanta, A.; Gerss, J.; Meersch, M. Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial. JAMA 2016, 315, 2190–2199. [Google Scholar] [CrossRef] [Green Version]
- Meersch, M.; Kullmar, M.; Schmidt, C.; Gerss, J.; Weinhage, T.; Margraf, A.; Ermert, T.; Kellum, J.A.; Zarbock, A. Long-Term Clinical Outcomes after Early Initiation of RRT in Critically Ill Patients with AKI. J. Am. Soc. Nephrol. 2018, 29, 1011–1019. [Google Scholar] [CrossRef]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute kidney injury increases risk of ESRD among elderly. J. Am. Soc. Nephrol. 2009, 20, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, V.C.; Huang, T.M.; Lai, C.F.; Shiao, C.C.; Lin, Y.F.; Chu, T.S.; Wu, P.C.; Chao, C.T.; Wang, J.Y.; Kao, T.W.; et al. Acute-on-chronic kidney injury at hospital discharge is associated with long-term dialysis and mortality. Kidney Int. 2011, 80, 1222–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.; Granath, F.; Schön, S.; Ekbom, A.; Martling, C.R. Continuous renal replacement therapy is associated with less chronic renal failure than intermittent haemodialysis after acute renal failure. Intensive Care Med. 2007, 33, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.G.; Bellomo, R.; Bagshaw, S.M.; Glassford, N.J.; Lo, S.; Jun, M.; Cass, A.; Gallagher, M. Choice of renal replacement therapy modality and dialysis dependence after acute kidney injury: A systematic review and meta-analysis. Intensive Care Med. 2013, 39, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Bonnassieux, M.; Duclos, A.; Schneider, A.G.; Schmidt, A.; Bénard, S.; Cancalon, C.; Joannes-Boyau, O.; Ichai, C.; Constantin, J.M.; Lefrant, J.Y.; et al. Renal Replacement Therapy Modality in the ICU and Renal Recovery at Hospital Discharge. Crit. Care Med. 2018, 46, e102–e110. [Google Scholar] [CrossRef]
- Wang, Y.; Gallagher, M.; Li, Q.; Lo, S.; Cass, A.; Finfer, S.; Myburgh, J.; Bouman, C.; Faulhaber-Walter, R.; Kellum, J.A.; et al. Renal replacement therapy intensity for acute kidney injury and recovery to dialysis independence: A systematic review and individual patient data meta-analysis. Nephrol. Dial. Transpl. 2018, 33, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- Ethgen, O.; Schneider, A.G.; Bagshaw, S.M.; Bellomo, R.; Kellum, J.A. Economics of dialysis dependence following renal replacement therapy for critically ill acute kidney injury patients. Nephrol. Dial. Transpl. 2015, 30, 54–61. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control | Dialysis | CRRT | p-Value | |
|---|---|---|---|---|
| Number of patients | 70,096 | 15,174 | 38,912 | |
| Gender | <0.001 | |||
| Male | 40,259 (57.4) | 9120 (60.1) | 24,133 (62.0) | |
| Female | 29,837 (42.6) | 6054 (39.9) | 14,779 (38.0) | |
| Age, years | 69.4 (14.9) | 64.5 (15.1) | 64.0 (15.1) | <0.001 |
| Pre-existing kidney disease | 7720 (11.0) | 5964 (39.3) | 7481 (19.2) | <0.001 |
| Comorbidity | ||||
| Myocardial infarction | 4131 (5.9) | 897 (5.9) | 2444 (6.3) | 0.03 |
| Congestive heart failure | 10,827 (15.4) | 3006 (19.8) | 5990 (15.4) | <0.001 |
| Peripheral vascular disease | 12,776 (18.2) | 3108 (20.5) | 7001 (18.0) | <0.001 |
| Cerebrovascular disease | 18,740 (26.7) | 3598 (23.7) | 8134 (20.9) | <0.001 |
| Rheumatologic disease | 3657 (5.2) | 805 (5.3) | 2516 (6.5) | <0.001 |
| Liver disease | 21,710 (31.0) | 5135 (33.8) | 15,127 (38.9) | <0.001 |
| Diabetes | 28,606 (40.8) | 8355 (55.1) | 17,908 (46.0) | <0.001 |
| Cancer | 10,527 (15.0) | 2453 (16.2) | 9306 (23.9) | <0.001 |
| AIDS/HIV | 51 (0.1) | 8 (0.1) | 36 (0.1) | 0.279 |
| Type of hospital | <0.001 | |||
| Tertiary | 20,157 (28.8) | 6162 (40.6) | 22,390 (57.5) | |
| General | 46,978 (67.0) | 8857 (58.4) | 16,297 (41.9) | |
| Nursing care hospital | 96 (0.1) | 17 (0.1) | 7 (0.0) | |
| Other | 2865 (4.1) | 138 (0.9) | 218 (0.6) | |
| Management procedures | ||||
| Mechanical ventilation | 26,662 (38.0) | 5564 (36.7) | 31,248 (80.3) | <0.001 |
| ECMO | 271 (0.4) | 25 (0.2) | 2002 (5.1) | <0.001 |
| Vasopressor drugs | 15,868 (22.6) | 3206 (21.1) | 19,278 (49.5) | <0.001 |
| Total cost, USD 10 * | 490 (229–971) | 807 (433–1459) | 1450 (720–2805) | <0.001 |
| Control | Dialysis | CRRT | p-Value | |
|---|---|---|---|---|
| Number of patients | 70,096 | 15,174 | 38,912 | |
| Gender | <0.001 | |||
| Male | 40,259 (57.4) | 9120 (60.1) | 24,133 (62.0) | |
| Female | 29,837 (42.6) | 6054 (39.9) | 14,779 (38.0) | |
| Age, years | 69.4 (14.9) | 64.5 (15.1) | 64.0 (15.1) | <0.001 |
| Pre-existing kidney disease | 7720 (11.0) | 5964 (39.3) | 7481 (19.2) | <0.001 |
| Comorbidity | ||||
| Myocardial infarction | 4131 (5.9) | 897 (5.9) | 2444 (6.3) | 0.03 |
| Congestive heart failure | 10,827 (15.4) | 3006 (19.8) | 5990 (15.4) | <0.001 |
| Peripheral vascular disease | 12,776 (18.2) | 3108 (20.5) | 7001 (18.0) | <0.001 |
| Cerebrovascular disease | 18,740 (26.7) | 3598 (23.7) | 8134 (20.9) | <0.001 |
| Rheumatologic disease | 3657 (5.2) | 805 (5.3) | 2516 (6.5) | <0.001 |
| Liver disease | 21,710 (31.0) | 5135 (33.8) | 15,127 (38.9) | <0.001 |
| Diabetes | 28,606 (40.8) | 8355 (55.1) | 17,908 (46.0) | <0.001 |
| Cancer | 10,527 (15.0) | 2453 (16.2) | 9306 (23.9) | <0.001 |
| AIDS/HIV | 51 (0.1) | 8 (0.1) | 36 (0.1) | 0.279 |
| Type of hospital | <0.001 | |||
| Tertiary | 20,157 (28.8) | 6162 (40.6) | 22,390 (57.5) | |
| General | 46,978 (67.0) | 8857 (58.4) | 16,297 (41.9) | |
| Nursing care hospital | 96 (0.1) | 17 (0.1) | 7 (0.0) | |
| Other | 2865 (4.1) | 138 (0.9) | 218 (0.6) | |
| Management procedures | ||||
| Mechanical ventilation | 26,662 (38.0) | 5564 (36.7) | 31,248 (80.3) | <0.001 |
| ECMO | 271 (0.4) | 25 (0.2) | 2002 (5.1) | <0.001 |
| Vasopressor drugs | 15,868 (22.6) | 3206 (21.1) | 19,278 (49.5) | <0.001 |
| Total cost, USD 10 * | 490 (229–971) | 807 (433–1459) | 1450 (720–2805) | <0.001 |
| Length of Stay, Days | Crude Model | Adjusted Model a | ||||
|---|---|---|---|---|---|---|
| Median (IQR) | Ratio b (95% CI) | p-Value | Ratio b (95% CI) | p-Value | ||
| Hospital length of stay | ||||||
| Overall | ||||||
| Control | 17 (9–31) | Reference | Reference | |||
| Dialysis | 25 (14–43) | 1.40 (1.37–1.43) | <0.001 | 1.46 (1.43–1.49) | <0.001 | |
| CRRT | 29 (16–53) | 1.45 (1.42–1.48) | <0.001 | 1.22 (1.2–1.25) | <0.001 | |
| Pre-existing kidney disease | ||||||
| With pre-existing kidney disease | ||||||
| Control | 16 (9–30) | Reference | Reference | |||
| Dialysis | 24 (14–41) | 1.42 (1.37–1.47) | <0.001 | 1.48 (1.43–1.53) | <0.001 | |
| CRRT | 28 (16–48) | 1.57 (1.51–1.64) | <0.001 | 1.35 (1.3–1.41) | <0.001 | |
| Without pre-existing kidney disease | ||||||
| Control | 17 (9–32) | Reference | Reference | |||
| Dialysis | 25 (15–46) | 1.44 (1.40–1.48) | <0.001 | 1.46 (1.42–1.50) | <0.001 | |
| CRRT | 30 (16–55) | 1.43 (1.40–1.46) | <0.001 | 1.19 (1.16–1.22) | <0.001 | |
| ICU length of stay | ||||||
| Overall | ||||||
| Control | 6 (2–14) | Reference | Reference | |||
| Dialysis | 6 (3–15) | 0.95 (0.93–0.97) | <0.001 | 1.10 (1.08–1.13) | <0.001 | |
| CRRT | 18 (8–34) | 2.06 (2.02–2.11) | <0.001 | 1.43 (1.40–1.46) | <0.001 | |
| Pre-existing kidney disease | ||||||
| With pre-existing kidney disease | ||||||
| Control | 5 (2–12) | Reference | Reference | |||
| Dialysis | 5 (2–10) | 0.88 (0.85–0.92) | <0.001 | 0.98 (0.94–1.01) | 0.239 | |
| CRRT | 14 (6–28) | 2.18 (2.08–2.28) | <0.001 | 1.52 (1.45–1.58) | <0.001 | |
| Without pre-existing kidney disease | ||||||
| Control | 6 (2–14) | Reference | Reference | |||
| Dialysis | 8 (4–20) | 1.13 (1.10–1.17) | <0.001 | 1.20 (1.17–1.23) | <0.001 | |
| CRRT | 18 (8–37) | 2.10 (2.05–2.15) | <0.001 | 1.40 (1.37–1.43) | <0.001 | |
| Person Years | No. of Cases | Incidence Rate (per 1000 Person-Years) | Model 1 HR (95% CI) | Model 2 HR (95% CI) | |
|---|---|---|---|---|---|
| Overall | |||||
| Control | 35,140.5 | 570 | 16.2 | Reference | Reference |
| Dialysis | 3986.5 | 1849 | 463.8 | 25.48 (21.30–30.48) | 17.67 (15.06–20.72) |
| CRRT | 8014.1 | 1014 | 126.5 | 7.74 (6.59–9.10) | 7.28 (6.29–8.41) |
| p-value | <0.001 | <0.001 | |||
| With pre-existing kidney disease | |||||
| Control | 3984.4 | 222 | 55.7 | Reference | Reference |
| Dialysis | 974 | 1168 | 1199.2 | 15.76 (13.37–18.58) | 15.15 (12.88–17.83) |
| CRRT | 1426.5 | 480 | 336.5 | 5.37 (4.52–6.38) | 5.83 (4.89–6.96) |
| p-value | <0.001 | <0.001 | |||
| Without pre-existing kidney disease | |||||
| Control | 31,156.1 | 348 | 11.2 | Reference | Reference |
| Dialysis | 3012.5 | 681 | 226.1 | 19.22 (15.39–24.01) | 20.06 (16.06–25.05) |
| CRRT | 6587.6 | 534 | 81.1 | 7.30 (6.03–8.85) | 8.86 (7.30–10.76) |
| p-value | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, S.; Kang, D.; Park, H.; Kim, Y.; Guallar, E.; Jeon, J.; Lee, J.-E.; Huh, W.; Suh, G.-Y.; Cho, J.; et al. Impact of Renal Replacement Therapy on Mortality and Renal Outcomes in Critically Ill Patients with Acute Kidney Injury: A Population-Based Cohort Study in Korea between 2008 and 2015. J. Clin. Med. 2022, 11, 2392. https://doi.org/10.3390/jcm11092392
Hwang S, Kang D, Park H, Kim Y, Guallar E, Jeon J, Lee J-E, Huh W, Suh G-Y, Cho J, et al. Impact of Renal Replacement Therapy on Mortality and Renal Outcomes in Critically Ill Patients with Acute Kidney Injury: A Population-Based Cohort Study in Korea between 2008 and 2015. Journal of Clinical Medicine. 2022; 11(9):2392. https://doi.org/10.3390/jcm11092392
Chicago/Turabian StyleHwang, Subin, Danbee Kang, Hyejeong Park, Youngha Kim, Eliseo Guallar, Junseok Jeon, Jung-Eun Lee, Wooseong Huh, Gee-Young Suh, Juhee Cho, and et al. 2022. "Impact of Renal Replacement Therapy on Mortality and Renal Outcomes in Critically Ill Patients with Acute Kidney Injury: A Population-Based Cohort Study in Korea between 2008 and 2015" Journal of Clinical Medicine 11, no. 9: 2392. https://doi.org/10.3390/jcm11092392