
Lumbosacral Transitional Vertebra Contributed to Lumbar Spine Degeneration: An MR Study of Clinical Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Image Evaluation
2.3. LSTV Evaluation
2.4. Disc Degeneration
2.5. Endplate Degeneration
2.6. Canal Stenosis, Ligamentum Flavum Thickening, and Facet Joint Degeneration
2.7. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Differences in MRI Findings between Unilateral and Bilateral LSTV
3.3. MRI Findings for Type I LSTV
3.4. MRI Findings for Type II LSTV
- (1)
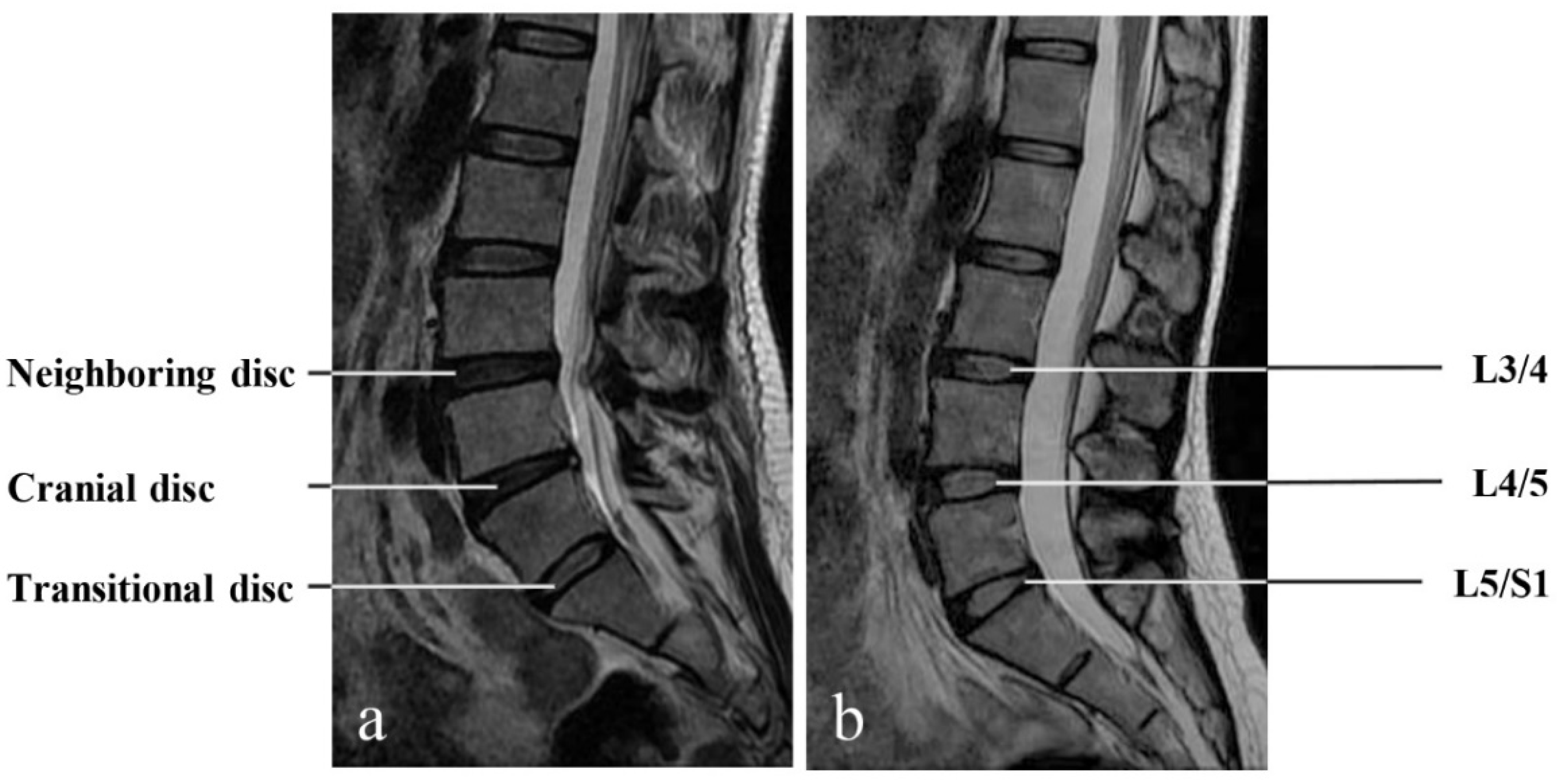
- The Transitional Disc
- (2)
- The cranial disc
- (3)
- The neighboring disc
3.5. MRI Findings for Type III LSTV
- (1)
- The Transitional Disc
- (2)
- The cranial disc
- (3)
- The neighboring disc
3.6. MRI Findings for Type IV LSTV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahato, N.K. Complete sacralization of L5 vertebrae: Traits, dimensions, and load bearing in the involved sacra. Spine J. 2010, 10, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Mahato, N.K. Morphological traits in sacra associated with complete and partial lumbarization of first sacral segment. Spine J. 2010, 10, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Apazidis, A.; Ricart, P.A.; Diefenbach, C.M.; Spivak, J.M. The prevalence of transitional vertebrae in the lumbar spine. Spine J. 2011, 11, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Nardo, L.; Alizai, H.; Virayavanich, W.; Liu, F.; Hernandez, A.; Lynch, J.A.; Nevitt, M.C.; McCulloch, C.E.; Lane, N.E.; Link, T.M. Lumbosacral Transitional Vertebrae: Association with Low Back Pain. Radiology 2012, 265, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Tang, M.; Yang, X.-F.; Yang, S.-W.; Han, P.; Ma, Y.-M.; Yu, H.; Zhu, B. Lumbosacral transitional vertebra in a population-based study of 5860 individuals: Prevalence and relationship to low back pain. Eur. J. Radiol. 2014, 83, 1679–1682. [Google Scholar] [CrossRef]
- Hanhivaara, J.; Määttä, J.H.; Niinimäki, J.; Nevalainen, M.T. Lumbosacral transitional vertebrae are associated with lumbar degeneration: Retrospective evaluation of 3855 consecutive abdominal CT scans. Eur. Radiol. 2020, 30, 3409–3416. [Google Scholar] [CrossRef] [Green Version]
- Lian, J.; Levine, N.; Cho, W. A review of lumbosacral transitional vertebrae and associated vertebral numeration. Eur. Spine J. 2018, 27, 995–1004. [Google Scholar] [CrossRef]
- Tini, P.G.; Wieser, C.; Zinn, W.M. The Transitional Vertebra of the Lumbosacral Spine: Its Radiological Classification, Incidence, Prevalence, and Clinical Significance. Rheumatology 1977, 16, 180–185. [Google Scholar] [CrossRef]
- Wellik, D.M.; Capecchi, M.R. Hox10 and Hox11 Genes Are Required to Globally Pattern the Mammalian Skeleton. Science 2003, 301, 363–367. [Google Scholar] [CrossRef] [Green Version]
- Carapuço, M.; Nóvoa, A.; Bobola, N.; Mallo, M. Hox genes specify vertebral types in the presomitic mesoderm. Genes Dev. 2005, 19, 2116–2121. [Google Scholar] [CrossRef] [Green Version]
- Castellvi, A.E.; Goldstein, L.A.; Chan, D.P. Lumbosacral Transitional Vertebrae and Their Relationship with Lumbar Extradural Defects. Spine 1984, 9, 493–495. [Google Scholar] [CrossRef]
- Carrino, J.A.; Campbell, P.D.; Lin, D.C.; Morrison, W.B.; Schweitzer, M.E.; Flanders, A.E.; Eng, J.; Vaccaro, A.R. Effect of Spinal Segment Variants on Numbering Vertebral Levels at Lumbar MR Imaging. Radiology 2011, 259, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Elster, A.D. Bertolotti’s syndrome revisited. Transitional vertebrae of the lumbar spine. Spine 1989, 14, 1373–1377. [Google Scholar] [CrossRef] [PubMed]
- Luoma, K.; Vehmas, T.; Raininko, R.; Luukkonen, R.; Riihimäki, H. Lumbosacral transitional vertebra: Relation to disc degeneration and low back pain. Spine 2004, 29, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Hashimoto, K.; Tsubakino, T.; Hoshikawa, T.; Inawashiro, T.; Tanaka, Y. Lumbosacral Transitional Vertebrae Cause Spinal Level Misconception in Surgeries for Degenerative Lumbar Spine Disorders. Tohoku J. Exp. Med. 2017, 242, 223–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farshad-Amacker, N.; Herzog, R.J.; Hughes, A.P.; Aichmair, A.; Farshad, M. Associations between lumbosacral transitional anatomy types and degeneration at the transitional and adjacent segments. Spine J. 2015, 15, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Apaydin, M.; Uluc, M.E.; Sezgin, G. Lumbosacral transitional vertebra in the young men population with low back pain: Anatomical considerations and degenerations (transitional vertebra types in the young men population with low back pain). La Radiol. Med. 2018, 124, 375–381. [Google Scholar] [CrossRef]
- Hou, L.; Bai, X.; Li, H.; Gao, T.; Li, W.; Wen, T.; He, Q.; Ruan, D.; Shi, L.; Bing, W. Lumbar plain radiograph is not reliable to identify lumbosacral transitional vertebra types according to Castellvi classification principle. BMC Musculoskelet. Disord. 2020, 21, 333. [Google Scholar] [CrossRef]
- Pfirrmann, C.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Deyo, R.A.; Mirza, S.K. Clinical Practice. Herniated Lumbar Intervertebral Disk. N. Engl. J. Med. 2016, 374, 1763–1772. [Google Scholar] [CrossRef]
- Feng, Z.; Liu, Y.; Wei, W.; Hu, S.; Wang, Y. Type II Modic Changes May not Always Represent Fat Degeneration: A Study Using MR Fat Suppression Sequence. Spine 2016, 41, E987–E994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, Y.Y.-N.; Diederichs, G.; Walter, T.C.; Wagner, M.; Liebig, T.; Rickert, M.; Hermann, K.-G.; Hamm, B.; Makowski, M.R. Differentiation of Osteophytes and Disc Herniations in Spinal Radiculopathy Using Susceptibility-Weighted Magnetic Resonance Imaging. Investig. Radiol. 2017, 52, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Pye, S.R.; Reid, D.M.; Lunt, M.; Adams, J.E.; Silman, A.J.; O’Neill, T.W. Lumbar disc degeneration: Association between osteophytes, end-plate sclerosis and disc space narrowing. Ann. Rheum. Dis. 2007, 66, 330–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Shen, H.; Wu, J.; Hu, X.; Zhu, Z.; Lv, X.; Liu, Y.; Wang, Y. Spine Explorer: A deep learning based fully automated program for efficient and reliable quantifications of the vertebrae and discs on sagittal lumbar spine MR images. Spine J. 2020, 20, 590–599. [Google Scholar] [CrossRef]
- Suthar, P.; Patel, R.; Mehta, C.; Patel, N. MRI evaluation of lumbar disc degenerative disease. J Clin. Diagn. Res. 2015, 9, Tc04-9. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Videman, T.; Niemeläinen, R.; Battié, M.C. Quantitative measures of modic changes in lumbar spine magnetic resonance imaging: Intra- and inter-rater reliability. Spine 2011, 36, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Modic, M.T.; Steinberg, P.M.; Ross, J.S.; Masaryk, T.J.; Carter, J.R. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988, 166, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Liu, Y.; Yang, G.; Battié, M.C.; Wang, Y. Lumbar vertebral endplate defects on magnetic resonance images: Classification, distribution patterns, and associations with Modic changes and disc degeneration. Spine 2018, 43, 919–927. [Google Scholar] [CrossRef]
- Lee, G.Y.; Lee, J.W.; Choi, H.S.; Oh, K.-J.; Kang, H.S. Erratum to: A new grading system of lumbar central canal stenosis on MRI: An easy and reliable method. Skelet. Radiol. 2011, 40, 1127. [Google Scholar] [CrossRef] [Green Version]
- Weishaupt, D.; Zanetti, M.; Boos, N.; Hodler, J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skelet. Radiol. 1999, 28, 215–219. [Google Scholar] [CrossRef]
- Peckham, M.; Hutchins, T.; Stilwill, S.; Mills, M.; Morrissey, B.; Joiner, E.; Sanders, R.; Stoddard, G.; Shah, L. Localizing the L5 Vertebra Using Nerve Morphology on MRI: An Accurate and Reliable Technique. Am. J. Neuroradiol. 2017, 38, 2008–2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legaye, J.; Duval-Beaupère, C.; Hecquet, J.; Marty, C. Pelvic incidence: A fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur. Spine J. 1998, 7, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulay, C.; Tardieu, C.; Hecquet, J.; Benaim, C.; Mouilleseaux, B.; Marty, C.; Prat-Pradal, D.; Legaye, J.; Duval-Beaupère, G.; Pélissier, J. Sagittal alignment of spine and pelvis regulated by pelvic incidence: Standard values and prediction of lordosis. Eur. Spine J. 2006, 15, 415–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafage, V.; Schwab, F.; Patel, A.; Hawkinson, N.; Farcy, J.P. Pelvic tilt and truncal inclination: Two key radiographic parameters in the setting of adults with spinal deformity. Spine 2009, 34, E599–E606. [Google Scholar] [CrossRef]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the Normal Variation in the Sagittal Alignment of the Human Lumbar Spine and Pelvis in the Standing Position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef]
- Laouissat, F.; Sebaaly, A.; Gehrchen, M.; Roussouly, P. Classification of normal sagittal spine alignment: Refounding the Roussouly classification. Eur. Spine J. 2018, 27, 2002–2011. [Google Scholar] [CrossRef]
- Haffer, H.; Becker, L.; Putzier, M.; Wiethölter, M.; Ziegeler, K.; Diekhoff, T.; Pumberger, M.; Hardt, S. Changes of Fixed Anatomical Spinopelvic Parameter in Patients with Lumbosacral Transitional Vertebrae: A Matched Pair Analysis. Diagnosis 2021, 11, 59. [Google Scholar] [CrossRef]
- Golubovsky, J.L.; Colbrunn, R.W.; Klatte, R.S.; Nagle, T.F.; Briskin, I.N.; Chakravarthy, V.B.; Gillespie, C.M.; Reith, J.D.; Jasty, N.; Benzel, E.C.; et al. Development of a novel in vitro cadaveric model for analysis of biomechanics and surgical treatment of Bertolotti syndrome. Spine J. 2020, 20, 638–656. [Google Scholar] [CrossRef]
- Vergauwen, S.; Parizel, P.M.; Van Breusegem, L.; Van Goethem, J.W.; Nackaerts, Y.; Hauwe, L.V.D.; De Schepper, A.M. Distribution and incidence of degenerative spine changes in patients with a lumbo-sacral transitional vertebra. Eur. Spine J. 1997, 6, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Aihara, T.; Takahashi, K.; Ogasawara, A.; Itadera, E.; Ono, Y.; Moriya, H. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: A clinical and anatomical study. J. Bone Jt. Surg. Br. 2005, 87, 687–691. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent Segment Disease after Lumbar or Lumbosacral Fusion: Review of the Literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Hilibrand, A.S.; Robbins, M. Adjacent segment degeneration and adjacent segment disease: The consequences of spinal fusion? Spine J. 2004, 4, S190–S194. [Google Scholar] [CrossRef] [PubMed]
- Sekharappa, V.; Amritanand, R.; Krishnan, V.; David, K.S. Lumbosacral Transition Vertebra: Prevalence and Its Significance. Asian Spine J. 2014, 8, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paik, N.C.; Lim, C.S.; Jang, H.S. Numeric and Morphological Verification of Lumbosacral Segments in 8280 Consecutive Patients. Spine 2013, 38, E573–E578. [Google Scholar] [CrossRef] [PubMed]
- Wigh, R.E.; Anthony, H.F. Transitional Lumbosacral Discs. Spine 1981, 6, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Farshad-Amacker, N.A.; Lurie, B.; Herzog, R.J.; Farshad, M. Interreader and intermodality reliability of standard anteroposterior radiograph and magnetic resonance imaging in detection and classification of lumbosacral transitional vertebra. Spine J. 2014, 14, 1470–1475. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Controls (N = 179) | Type I (N = 182) | Type II (N = 107) | Type III (N = 43) | Type IV (N = 18) | |
|---|---|---|---|---|---|
| Disc bulging | |||||
| Neighboring disc | 43 (24.0%) | 59 (32.4%) | 58 (54.2%) * | 22 (51.2%) * | 9 (50.0%) * |
| Cranial disc | 96 (53.6%) | 111 (61.0%) | 94 (87.9%) * | 24 (55.8%) # | 12 (66.7%) |
| Transitional disc | 70 (39.1%) | 78 (42.9%) | 55 (51.4%) * | 1 (2.3%) *# | 1 (5.6%) * |
| Osteophytes | |||||
| Neighboring disc | 49 (27.4%) | 36 (19.8%) | 42 (39.3%) * | 10 (23.3%) | 5 (27.8%) |
| Cranial disc | 41 (22.9%) | 36 (19.8%) | 42 (39.3%) * | 15 (34.9%) | 9 (50.0%) * |
| Transitional disc | 27 (15.1%) | 22 (12.1%) | 30 (28.0%) * | 1 (2.3%) *# | 1 (5.6%) |
| Disc herniation | |||||
| Neighboring disc | 8 (4.5%) | 11 (6.0%) | 14 (13.1%) * | 5 (11.6%) | 2 (11.1%) |
| Cranial disc | 46 (25.7%) | 46 (25.3%) | 43 (40.2%) * | 18 (41.9%) * | 9 (50.0%) * |
| Transitional disc | 57 (31.8%) | 42 (23.1%) | 27 (25.2%) | 1 (2.3%) *# | 1 (5.6%) * |
| Modic changes | |||||
| Neighboring disc | 13 (7.3%) | 15 (8.2%) | 12 (11.2%) | 2 (4.7%) | 2 (11.1%) |
| Cranial disc | 23 (12.8%) | 29 (15.9%) | 24 (22.4%) * | 8 (18.6%) | 5 (27.8%) |
| Transitional disc | 30 (16.8%) | 35 (19.2%) | 20 (18.7%) | 1 (2.3%) *# | 1 (5.6%) |
| Endplate defects | |||||
| Neighboring disc | 27 (7.5%) | 12 (6.6%) | 22 (20.6%) * | 6 (14.0%) | 6 (33.3%) * |
| Cranial disc | 52 (14.4%) | 27 (14.8%) | 38 (35.5%) * | 12 (27.9%) * | 6 (33.3%) * |
| Transitional disc | 44 (12.2%) | 21 (11.5%) | 24 (22.4%) * | 2 (4.7%) # | 1 (5.6%) |
| Spondylolisthesis | |||||
| Neighboring disc | 2 (1.1%) | 3 (1.6%) | 4 (3.7%) | 4 (9.3%) * | 2 (11.1%) * |
| Cranial disc | 13 (7.3%) | 12 (6.6%) | 16 (15.0%) * | 8 (18.6%) * | 1 (5.6%) |
| Transitional disc | 7 (3.9%) | 3 (1.6%) | 2 (1.9%) | 0 (0%) | 0 (0%) |
| Coefficient | 95% CI | p Value | |
|---|---|---|---|
| Pfirrmann score | 0.027 | (0.001, 0.054) | 0.044 * |
| Disc height | −0.108 | (−0.186, −0.030) | 0.007 * |
| Disc signal | −0.003 | (−0.004, −0.001) | 0.007 * |
| Coefficient | 95% CI | p Value | |
|---|---|---|---|
| Pfirrmann score | 0.002 | (−0.003, 0.007) | 0.436 |
| Disc height | 0.009 | (−0.035, −0.055) | 0.666 |
| Disc signal | 0.001 | (−0.003, 0.004) | 0.788 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, L.; Jiang, C.; Huang, J.; Jin, J.; Guan, M.; Wang, Y. Lumbosacral Transitional Vertebra Contributed to Lumbar Spine Degeneration: An MR Study of Clinical Patients. J. Clin. Med. 2022, 11, 2339. https://doi.org/10.3390/jcm11092339
Cheng L, Jiang C, Huang J, Jin J, Guan M, Wang Y. Lumbosacral Transitional Vertebra Contributed to Lumbar Spine Degeneration: An MR Study of Clinical Patients. Journal of Clinical Medicine. 2022; 11(9):2339. https://doi.org/10.3390/jcm11092339
Chicago/Turabian StyleCheng, Linxiang, Chao Jiang, Jiawei Huang, Jiale Jin, Ming Guan, and Yue Wang. 2022. "Lumbosacral Transitional Vertebra Contributed to Lumbar Spine Degeneration: An MR Study of Clinical Patients" Journal of Clinical Medicine 11, no. 9: 2339. https://doi.org/10.3390/jcm11092339