
Risk Stratification and Clinical Characteristics of Patients with Late Recurrence of Melanoma (>10 Years)


Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garbe, C.; Leiter, U. Melanoma epidemiology and trends. Clin. Dermatol. 2009, 27, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Herbert, A.; Koo, M.M.; Barclay, M.E.; Greenberg, D.C.; Abel, G.A.; Levell, N.J.; Lyratzopoulos, G. Stage-specific incidence trends of melanoma in an English region, 1996–2015, Longitudinal analyses of population-based data. Melanoma Res. 2018, 30, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Bredgaard, R.; Lock-Andersen, J. Recurrence of cutaneous malignant melanoma after more than 20 years. J. Plast. Surg. Hand Surg. 2011, 45, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Faries, M.B.; Steen, S.; Ye, X.; Sim, M.; Morton, D.L. Late recurrence in melanoma: Clinical implications of lost dormancy. J. Am. Coll. Surg. 2013, 217, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callaway, M.P.; Briggs, J.C. The incidence of late recurrence (greater than 10 years); an analysis of 536 consecutive cases of cutaneous melanoma. Br. J. Plast. Surg. 1989, 42, 46–49. [Google Scholar] [CrossRef]
- Sosa, M.S.; Bragado, P.; Aguirre-Ghiso, J.A. Mechanisms of disseminated cancer cell dormancy: An awakening field. Nat. Rev. Cancer 2014, 14, 611–622. [Google Scholar] [CrossRef]
- Senft, D.; Ronai, Z.A. Immunogenic, cellular, and angiogenic drivers of tumor dormancy—A melanoma view. Pigment. Cell Melanoma Res. 2016, 29, 27–42. [Google Scholar] [CrossRef] [Green Version]
- Piskounova, E.; Agathocleous, M.; Murphy, M.M.; Hu, Z.; Huddlestun, S.E.; Zhao, Z.; Leitch, A.M.; Johnson, T.M.; DeBerardinis, R.J.; Morrison, S.J. Oxidative stress inhibits distant metastasis by human melanoma cells. Nature 2015, 527, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Huang, X.; Fu, L. Impact of smoking on efficacy of PD-1/PD-L1 inhibitors in non-small cell lung cancer patients: A meta-analysis. OncoTargets Ther. 2018, 11, 3691–3696. [Google Scholar] [CrossRef] [Green Version]
- Charalabopoulos, K.; Assimakopoulos, D.; Karkabounas, S.; Danielidis, V.; Kiortsis, D.; Evangelou, A. Effects of cigarette smoking on the antioxidant defence in young healthy male volunteers. Int. J. Clin. Pract. 2005, 59, 25–30. [Google Scholar] [CrossRef]
- Nguyen, N.; Couts, K.L.; Luo, Y.; Fujita, M. Understanding melanoma stem cells. Melanoma Manag. 2015, 2, 179–188. [Google Scholar] [CrossRef] [PubMed]
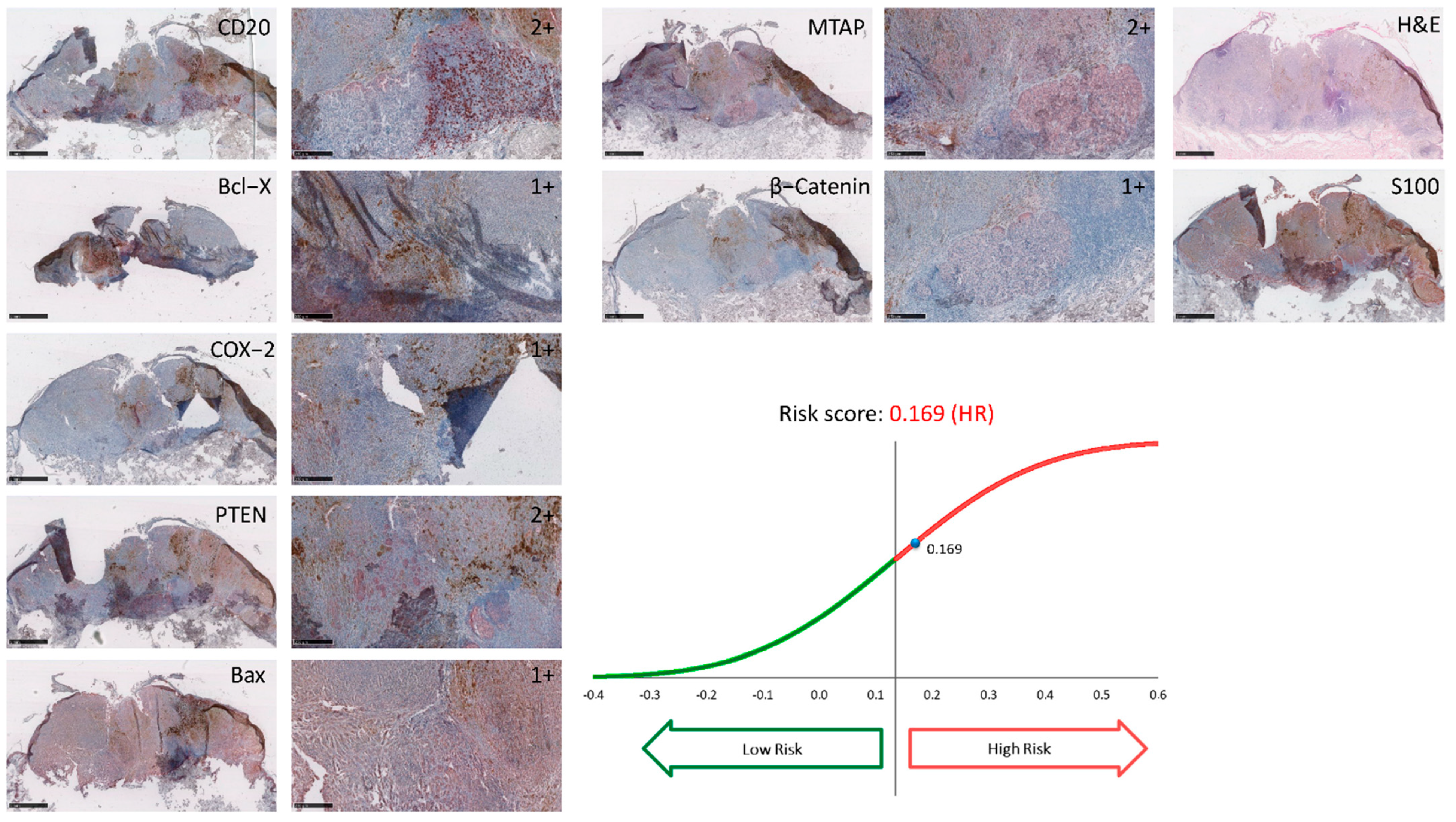
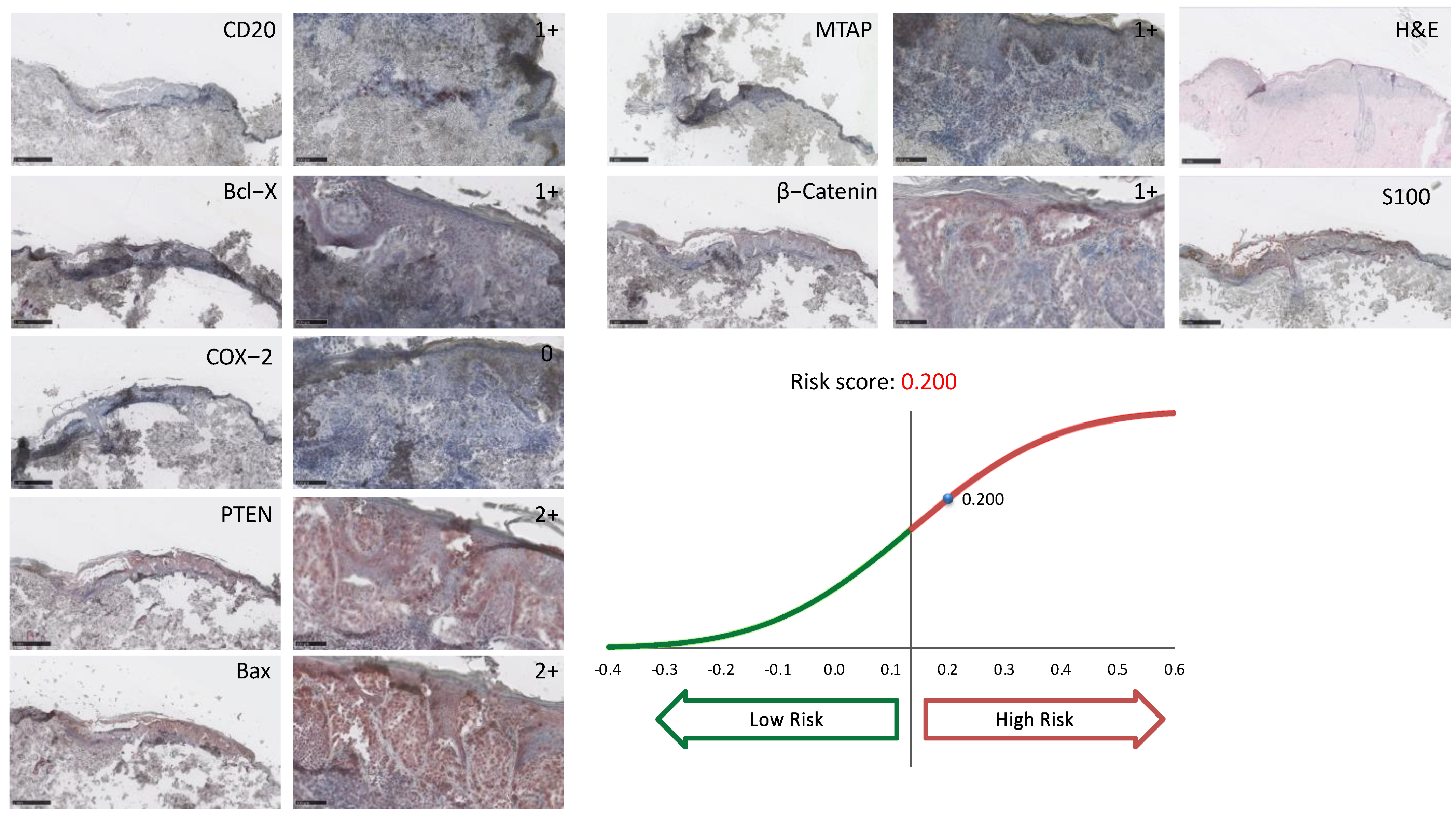
- Reschke, R.; Gussek, P.; Ziemer, M. Identifying High-Risk Tumors within AJCC Stage IB-III Melanomas Using a Seven-Marker Immunohistochemical Signature. Cancers 2021, 13, 2902. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Fuchs, T.J.; Bosserhoff, A.K.; Hofstädter, F.; Pauer, A.; Roth, V.; Buhmann, J.M.; Moll, I.; Anagnostou, N.; Brandner, J.M.; et al. A seven-marker signature and clinical outcome in malignant melanoma: A large-scale tissue-microarray study with two independent patient cohorts. PLoS ONE 2012, 7, e38222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gesellschaft der Epidemiologischen Krebsregister Deutschland. Melanom Atlas. Available online: http://atlas.gekid.de/CurrentVersion/atlas.html (accessed on 15 March 2022).
- Stanienda-Sokół, K.; Salwowska, N.; Sławińska, M.; Wicherska-Pawłowska, K.; Lorenc, A.; Wcisło-Dziadecka, D.; Wydmański, J.; Majewski, W. Primary Locations of Malignant Melanoma Lesions Depending on Patients’ Gender and Age. Asian Pac. J. Cancer Prev. APJCP 2017, 18, 3081–3086. [Google Scholar] [CrossRef]
- Tahery, D.P.; Moy, R.L. Lack of predictive factors in late recurrence of stage I melanoma. Int. J. Dermatol. 1992, 31, 629–631. [Google Scholar] [CrossRef]
- Ding, Y.; Zhang, S.; Qiao, J. Prognostic value of neutrophil-to-lymphocyte ratio in melanoma: Evidence from a PRISMA-compliant meta-analysis. Medicine 2018, 97, e11446. [Google Scholar] [CrossRef]
- Krähn, G.; Kaskel, P.; Sander, S.; Waizenhöfer, P.J.; Wortmann, S.; Leiter, U.; Peter, R.U. S100 beta is a more reliable tumor marker in peripheral blood for patients with newly occurred melanoma metastases compared with MIA, albumin and lactate-dehydrogenase. Anticancer Res. 2001, 21, 1311–1316. [Google Scholar]
- Sarac, E.; Wilhelmi, J.; Thomas, I.; Leiter, U.; Keim, U.; Eigentler, T.K.; Garbe, C.; Amaral, T. Late recurrence of melanoma after 10 years—Is the course of the disease different from early recurrences? J. Eur. Acad. Dermatol. Venereol. 2020, 34, 977–983. [Google Scholar] [CrossRef]
- Osella-Abate, S.; Ribero, S.; Sanlorenzo, M.; Maule, M.M.; Richiardi, L.; Merletti, F.; Tomasini, C.; Marra, E.; Macripò, G.; Fierro, M.T.; et al. Risk factors related to late metastases in 1372 melanoma patients disease free more than 10 years. Int. J. Cancer 2015, 136, 2453–2457. [Google Scholar] [CrossRef]
- Hohnheiser, A.M.; Gefeller, O.; Göhl, J.; Schuler, G.; Hohenberger, W.; Merkel, S. Malignant melanoma of the skin: Long-term follow-up and time to first recurrence. World J. Surg. 2011, 35, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Hansel, G.; Schönlebe, J.; Haroske, G.; Wollina, U. Late recurrence (10 years or more) of malignant melanoma in south-east Germany (Saxony). A single-centre analysis of 1881 patients with a follow-up of 10 years or more. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 833–836. [Google Scholar] [CrossRef] [PubMed]
- Leman, J.A.; Mac Kie, R.M. Late (10 years) recurrence of melanoma: The Scottish experience. Br. J. Dermatol. 2003, 148, 372–373. [Google Scholar] [CrossRef] [PubMed]
- Schmid-Wendtner, M.H.; Baumert, J.; Schmidt, M.; Konz, B.; Hölzel, D.; Plewig, G.; Volkenandt, M. Late metastases of cutaneous melanoma: An analysis of 31 patients. J. Am. Acad. Dermatol. 2000, 43, 605–609. [Google Scholar] [CrossRef]
- Peters, A.; Lippold, A.; Hundeiker, M. Melanomerstmetastasen nach 10 und mehr Jahren Erscheinungsfreiheit. Hautarzt 1997, 48, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Tsao, H.; Cosimi, A.B.; Sober, A.J. Ultra-late recurrence (15 years or longer) of cutaneous melanoma. Cancer 1997, 79, 2361–2370. [Google Scholar] [CrossRef]
- Crowley, N.J.; Seigler, H.F. Late recurrence of malignant melanoma. Analysis of 168 patients. Ann. Surg. 1990, 212, 173–177. [Google Scholar] [CrossRef]
- McEwan, L.; Smith, J.G.; Matthews, J.P. Late recurrence of localized cutaneous melanoma: Its influence on follow-up policy. Plast. Reconstr. Surg. 1990, 86, 527–534. [Google Scholar] [CrossRef]
- Landthaler, M.; Braun-Falco, O.; Schlamminger, F.; Schubert-Fritschle, G. Späte Metastasierung bei malignem Melanom der Haut. Dtsch. Med. Wochenschr. 1989, 114, 1149–1152. [Google Scholar] [CrossRef]
- Gutman, M.; Klausner, J.M.; Inbar, M.; Rozin, R.R. Late recurrence of stage I malignant melanoma. J. Surg. Oncol. 1989, 42, 96–98. [Google Scholar] [CrossRef]
- Shaw, H.M.; Beattie, C.W.; McCarthy, W.H.; Milton, G.W. Late relapse from cutaneous stage I malignant melanoma. Arch. Surg. 1985, 120, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Briele, H.A.; Beattie, C.W.; Ronan, S.G.; Chaudhuri, P.K.; Das Gupta, T.K. Late recurrence of cutaneous melanoma. Arch. Surg. 1983, 118, 800–803. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.S.; Kopf, A.W.; Rigel, D.S.; Friedman, R.J.; Levine, J.L.; Levenstein, M.; Bart, R.S.; Mintzis, M.M. Effect of anatomical location on prognosis in patients with clinical stage I melanoma. Arch. Dermatol. 1983, 119, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Erturk, K. Limb melanomas: Acral melanomas have worse survival. J. Dermatol. Treat. 2021, 1–8. [Google Scholar] [CrossRef]
- El Sharouni, M.A.; Ahmed, T.; Witkamp, A.J.; Sigurdsson, V.; van Gils, C.H.; Nieweg, O.E.; Scolyer, R.A.; Thompson, J.F.; van Diest, P.J.; Lo, S.N. Predicting recurrence in patients with sentinel node-negative melanoma: Validation of the EORTC nomogram using population-based data. Br. J. Surg. 2021, 108, 550–553. [Google Scholar] [CrossRef]
- Reschke, R.; Jäger, I.; Mehnert-Theuerkauf, A.; Ziemer, M. Therapy understanding and health related quality of life in stage III/IV melanoma patients treated with novel adjuvant therapies. J. Dtsch. Dermatol. Ges. 2021, 19, 215–221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overview | Total | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | 36 (100%) | 18 (50%) | 18 (50%) | |||||||||
| Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | |
| Age at primary diagnosis [years] | 51.4 | 50.6 | 76 | 27.8 | 50.9 | 51.9 | 75.8 | 27.8 | 51.8 | 50.6 | 76 | 30.2 |
| Age at manifestation of metastatic disease [years] | 66.3 | 68.2 | 89.4 | 41 | 66.7 | 69.3 | 89.4 | 41 | 65.8 | 66.4 | 87.7 | 41.2 |
| Years until occurrence of metastases | 14.9 | 12.4 | 33.2 | 10.1 | 15.8 | 13.3 | 33.2 | 10.1 | 14 | 11.9 | 29.7 | 10.1 |
| Localization of primary melanoma: | ||||||||||||
| Head/Neck n (%) | 5 (13.9%) | 3 (16.7%) | 2 (11.1%) | |||||||||
| Trunk n (%) | 19 (52.8%) | 11 (61.1%) | 8 (44.4%) | |||||||||
| Upper extremity n (%) | 5 (13.9%) | 1 (5.6%) | 4 (22.2%) | |||||||||
| Lower extremity n (%) | 7 (19.4%) | 3 (16.7%) | 4 (22.2%) | |||||||||
| Primary Melanoma Histopathology | Total | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | 24 (100%) | 12 (50%) | 12 (50%) | |||||||||
| Ulceration, n (%) | 4 (16.7%) | 2 (16.7%) | 2 (16.7%) | |||||||||
| Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | |
| Breslow’s depth [mm] | 1.8 | 1.5 | 4.5 | 0.4 | 1.7 | 1.6 | 3 | 0.4 | 1.8 | 1.4 | 4.5 | 0.6 |
| S100 at the Time of Metastatic Disease | Total | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | 24 (100%) | 14 (58.3%) | 10 (41.7%) | |||||||||
| S100 normal n (%) (<0.105 ng/mL) | 14 (58.3%) | 10 (71.4%) | 4 (40%) | |||||||||
| S100 increased n (%) (≥0.105 ng/mL) | 10 (41.7%) | 4 (28.6%) | 6 (60%) | |||||||||
| Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | |
| S100 (without one outlier) [ng/mL] | 0.28 | 0.07 | 2.16 | 0.05 | 0.25 | 0.07 | 2.16 | 0.05 | 0.33 | 0.11 | 1.85 | 0.05 |
| LDH at the Time of Metastatic Disease | Total | Male | Female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | 24 (100%) | 12 (50%) | 12 (50%) | |||||||||
| LDH normal n (%) (2.25–3.55 µkat/L) | 6 (25%) | 4 (33.3%) | 2 (16.7%) | |||||||||
| LDH increased n (%) (>3.55 µkat/L) | 18 (75%) | 8 (66.7%) | 10 (83.3%) | |||||||||
| Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | Mean | Median | Maximum | Minimum | |
| LDH (without one outlier [ng/mL] | 5.1 | 4.7 | 10.2 | 2.9 | 4.8 | 4.7 | 8.7 | 2.9 | 5.4 | 4.7 | 10.2 | 3.2 |
| Neutrophil-to-Lymphocyte-Ratio (NLR) | ≤5 | >5 | |
|---|---|---|---|
| Time period until metastatic disease [years] | Mean | 13.97 | 19.31 |
| Median | 12.36 | 15.36 | |
| n (Total Cases) | % LR Melanoma | n (LR Melanoma >10 Years) | n (Female) | n (Male) | Age at Primary Diagnosis (Years) | Period Until Metastasis (Years) | Breslow’s Depth (mm) | Ulceration | Localization: Trunk | Localization: Lower Extremity | Localization: Upper Extremity | Localization: Head/Neck | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reschke (2022) | - | - | 36 | 18 (50%) | 18 (50%) | 51 | 14.9 | 1.8 | 4 (16.7%) ** | 19 (52.8%) | 6 (16.7%) | 6 (16.7%) | 5 (13.9%) |
| Sarac [20] (2020) | 1537 | 99 | 45 (45.5%) | 54 (54.5%) | - | 14.5 | - | 8 (13.6%) | 44 (44.4%) | 29 (29.3%) | 17 (17.2%) | 9 (9.1%) | |
| Osella-Abate [21] (2015) | 3580 | 2.2% | 77 | 46 (59.7%) | 31 (40.3%) | 48 | - | 2.3 | 7 (9.1%) | 40 (51.9%) | 31 (40.3%) | 0 | 6 (7.8%) |
| Faries [4] (2013) | - | - | 406 | 171 (41.9%) | 235 (57.6%) | 41 | 15.7 | 1.2 | 22 (5.4%) | 185 (45.3%) | 155 (38.0%) | 68 (16.7%) | |
| Hohnheiser [22] (2011) | 2062 | 1.6% | 34 | - | - | 52 | - | - | - | - | - | - | - |
| Hansel [23] (2010) | 2314 | 0.9% | 20 | 13 (65%) | 7 (35%) | 44 | 13.9 | 2 | 4 (20%) | 6 (30.0%) | 9 (45.0%) | 4 (20.0%) | 1 (5.0%) |
| Leman [24] (2003) | - | - | 25 | 13 (52%) | 12 (48%) | - | 11 | - | - | - | - | - | - |
| Schmid-Wendtner [25] (2000) | 6298 | 0.5% | 31 | 15 (4.4%) | 16 (51.6%) | - | 12.6 | 1.4 | - | 16 (51.6%) | - | - | - |
| Peters [26] (1997) | - | - | 36 | 20 (55.6%) | 16 (44.4%) | 50 | 12.5 | 1.8 | - | 12 (33.3%) | 11 (30.6%) | 5 (13.9%) | 8 (22.2%) |
| Tsao [27] (1997) * | 2766 | 0.7% | 20 | 10 (50%) | 10 (50%) | 36 | 18.7 | - | - | 7 (35.0%) | 10 (50.0%) | 3 (15.0%) | |
| Tahery [17] (1992) | 4301 | 0.2% | 8 | 3 (37.5%) | 5 (62.5%) | 43 | 15.3 | - | 1 (12.5%) | 2 (25.0%) | 4 (50.0%) | 2 (25.0%) | 0 |
| Crowley [28] (1990) | 7104 | 2.4% | 168 | 89 (53.0%) | 79 (47.0%) | - | 14.3 | 1.6 | - | 67 (39.9%) | 67 (39.9%) | 21 (12.5%) | |
| McEwan [29] (1990) | 769 | 1.4% | 11 | 7 (63.6%) | 4 (36.4%) | 45 | 14.2 | 1.3 | 2 (18.2%) | 3 (27.3%) | 3 (27.3%) | 3 (27.3%) | 2 (18.1%) |
| Landthaler [30] (1989) | 2403 | 0.4% | 10 | 7 (70%) | 3 (30%) | - | - | 1.7 | - | 4 (40.0%) | 2 (20.0%) | 2 (20.0%) | 2 (20.0%) |
| Gutman [31] (1989) | 510 | 1.1% | 6 | 2 (33.3%) | 4 (66.7%) | 46 | - | - | - | 2 (33.3%) | 3 (50.0%) | 1 (16.7%) | 0 |
| Callaway [5] (1989) | - | - | 5 | 5 (100%) | 0 (0%) | 51 | 12.9 | 1.8 | 0 | 0 | 4 (80.0%) | 1 (20.0%) | |
| Shaw [32] (1985) | - | - | 34 | 16 (47.1%) | 18 (52.9%) | - | 13.7 | 2 | - | 11 (32.4%) | 18 (52.9%) | 5 (14.7%) | |
| Briele [33] (1983) | - | - | 7 | 6 (85.7%) | 1 (14.3%) | 27 | 16.6 | - | - | 1 (14.3%) | 5 (71.4%) | 1 (14.3%) | 0 |
| Total | 934 | 441 (49%) | 459 (51%) | 375 (42.9%) | 352 (41.7%) | 122 (14.5%) | |||||||
| Average | 1.1% | 45 | 14.3 | 1.7 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reschke, R.; Dumann, K.; Ziemer, M. Risk Stratification and Clinical Characteristics of Patients with Late Recurrence of Melanoma (>10 Years). J. Clin. Med. 2022, 11, 2026. https://doi.org/10.3390/jcm11072026
Reschke R, Dumann K, Ziemer M. Risk Stratification and Clinical Characteristics of Patients with Late Recurrence of Melanoma (>10 Years). Journal of Clinical Medicine. 2022; 11(7):2026. https://doi.org/10.3390/jcm11072026
Chicago/Turabian StyleReschke, Robin, Konstantin Dumann, and Mirjana Ziemer. 2022. "Risk Stratification and Clinical Characteristics of Patients with Late Recurrence of Melanoma (>10 Years)" Journal of Clinical Medicine 11, no. 7: 2026. https://doi.org/10.3390/jcm11072026