
Psychological Profiles of Treatment-Seeking Adults with Overweight and Obesity: A Cluster Analysis Approach



Abstract
:1. Introduction
2. Methods
2.1. ESTEAM Cohort
2.2. Participants
2.3. Measures
2.3.1. Eating Self-Efficacy
2.3.2. State Self-Esteem
2.3.3. Perceived Stress
2.3.4. Physical Hunger
2.3.5. Body Satisfaction
2.3.6. Well-Being
2.3.7. Depressive Symptoms
2.3.8. Anthropometric and Demographic Information
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics of the Sample
3.2. Cluster Solution
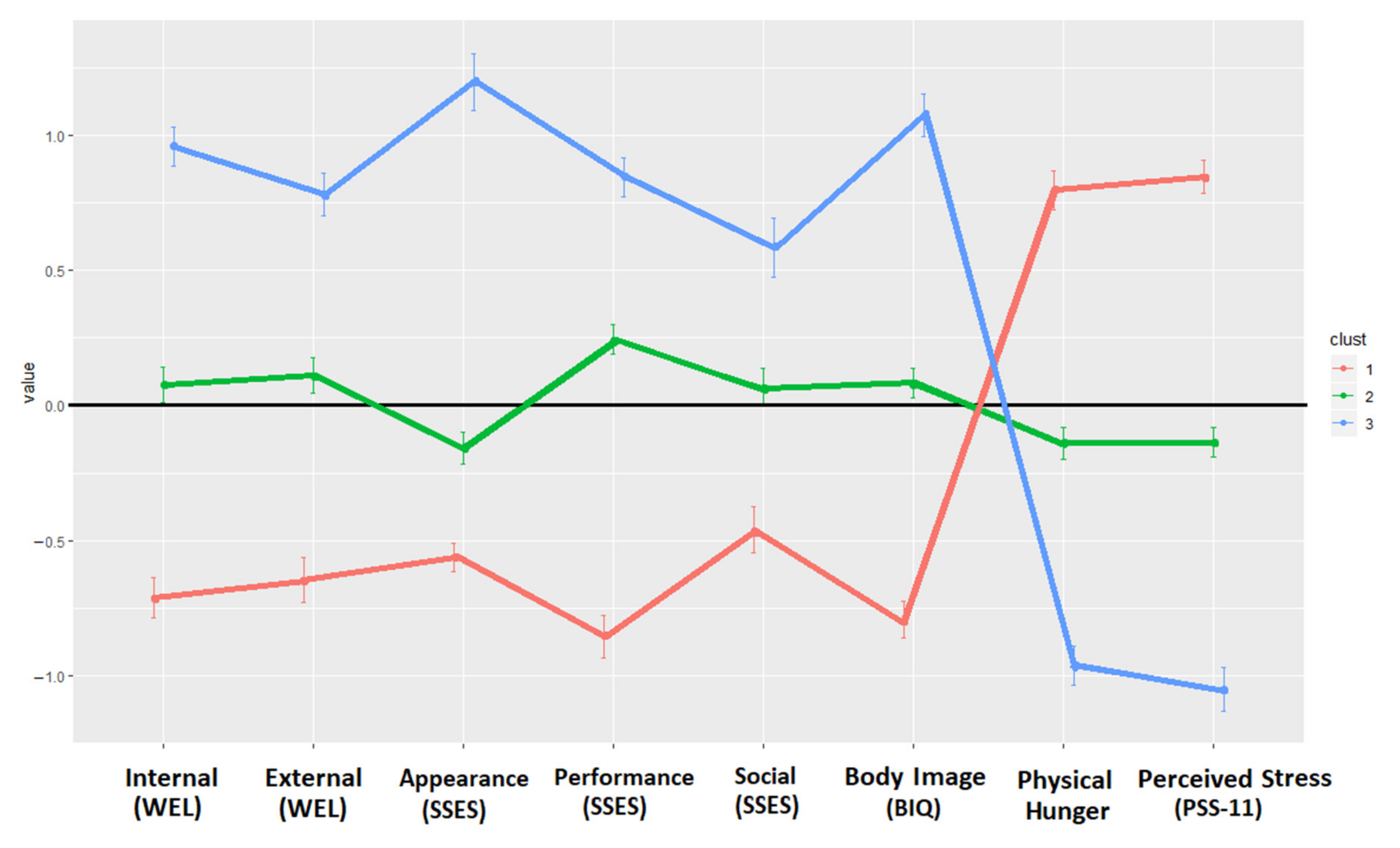
3.2.1. Female Subsample
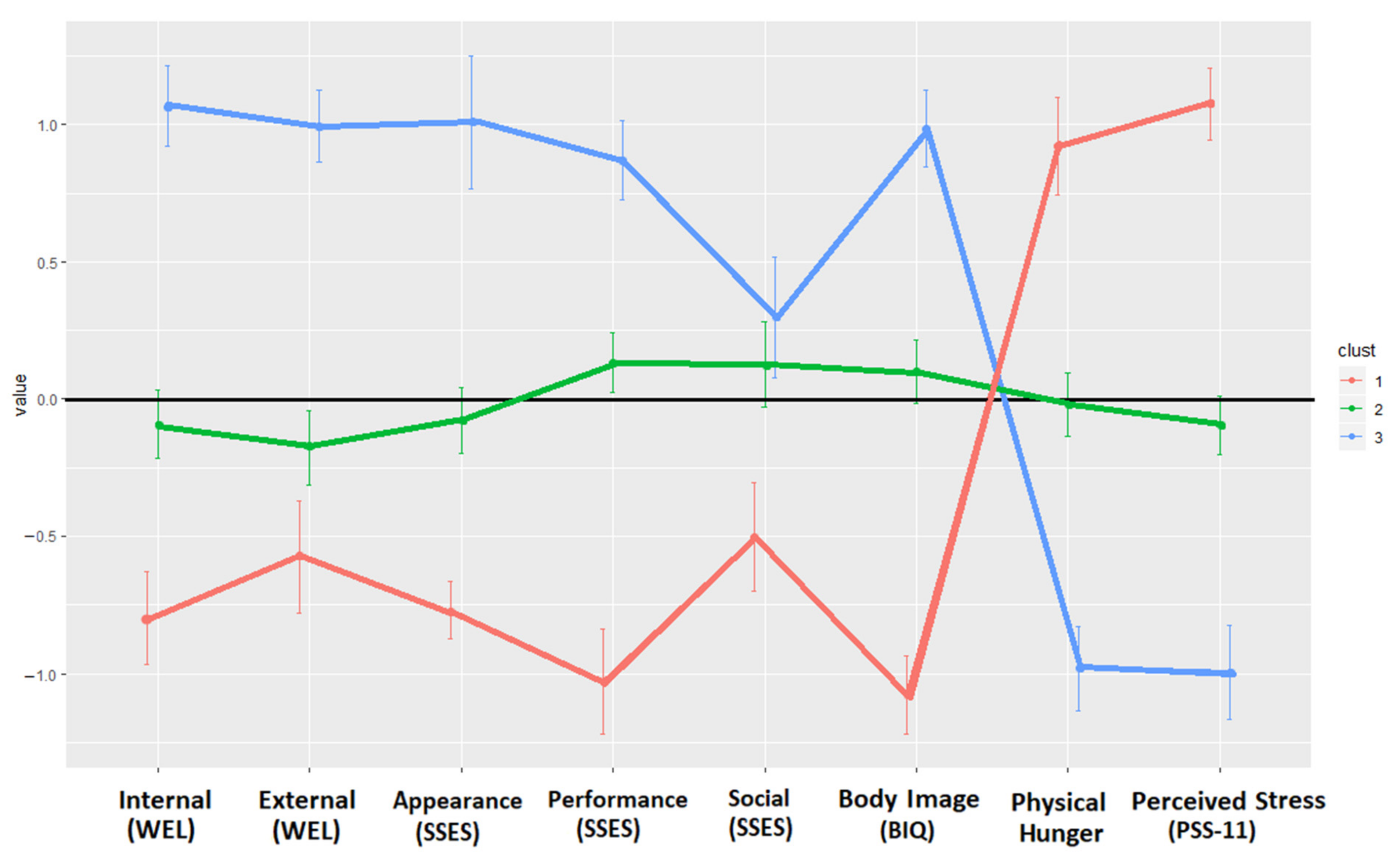
3.2.2. Male Subsample
3.3. Internal Validation of the Clusters
3.3.1. Female Subsample
3.3.2. Male Subsample
3.4. External Validation of the Clusters
3.4.1. Female Subsample
3.4.2. Male Subsample
4. Discussion
5. Clinical Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 30 August 2021).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Fryar, C.D.; Carroll, M.D.; Ogden, C.L. Prevalence of Overweight and Obesity among Children and Adolescents Aged 2–19 Years: United States, 1963–1965 through 2013–2014. National Center for Health Statistics Data, Health E-Stats. Available online: https://www.cdc.gov/nchs/data/hestat/obesity_child_13_14/obesity_child_13_14.htm (accessed on 8 October 2021).
- Chang, L.; Neu, J. Early factors leading to later obesity: Interactions of the microbiome, epigenome, and nutrition. Curr. Probl. Pediatric Adolesc. Health Care 2015, 45, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Bacaro, V.; Ballesio, A.; Cerolini, S.; Vacca, M.; Poggiogalle, E.; Donini, L.M.; Lucidi, F.; Lombardo, C. Sleep duration and obesity in adulthood: An updated systematic review and meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Fábrega-Cuadros, R.; Cruz-Díaz, D.; Martínez-Amat, A.; Aibar-Almazán, A.; Redecillas-Peiró, M.T.; Hita-Contreras, F. Associations of sleep and depression with obesity and sarcopenia in middle-aged and older adults. Maturitas 2020, 142, 1–7. [Google Scholar] [CrossRef]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- McCafferty, B.J.; Hill, J.O.; Gunn, A.J. Obesity: Scope, lifestyle interventions, and medical management. Tech. Vasc. Interv. Radiol. 2020, 23, 100653. [Google Scholar] [CrossRef]
- Claassen, M.A.; Klein, O.; Bratanova, B.; Claes, N.; Corneille, O. A systematic review of psychosocial explanations for the relationship between socioeconomic status and body mass index. Appetite 2019, 132, 208–221. [Google Scholar] [CrossRef] [Green Version]
- Newton, S.; Braithwaite, D.; Akinyemiju, T.F. Socio-economic status over the life course and obesity: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0177151. [Google Scholar] [CrossRef] [Green Version]
- Fleischhacker, S.E.; Evenson, K.R.; Rodriguez, D.A.; Ammerman, A.S. A systematic review of fast food access studies. Obes. Rev. 2011, 12, e460–e471. [Google Scholar] [CrossRef]
- Han, J.; Schwartz, A.E.; Elbel, B. Does Proximity to Fast Food Cause Childhood Obesity? Evidence from Public Housing. Reg. Sci. Urban Econ. 2020, 84, 103565. [Google Scholar] [CrossRef]
- Mason, K.E.; Pearce, N.; Cummins, S. Associations between fast food and physical activity environments and adiposity in mid-life: Cross-sectional, observational evidence from UK Biobank. Lancet Public Health 2018, 3, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Polsky, J.Y.; Moineddin, R.; Dunn, J.R.; Glazier, R.H.; Booth, G.L. Absolute and relative densities of fast-food versus other restaurants in relation to weight status: Does restaurant mix matter? Prev. Med. 2016, 82, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Zhang, X.; Huang, J.; Lu, X.; Liu, F.; Gu, D. Ambient air pollution and body weight status in adults: A systematic review and meta-analysis. Environ. Pollut. 2020, 265, 114999. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottière, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Energy balance and obesity: What are the main drivers? Cancer Causes Control 2017, 28, 247–258. [Google Scholar] [CrossRef] [Green Version]
- Friedman, M.A.; Brownell, K.D. Psychological correlates of obesity: Moving to the next research generation. Psychol. Bull. 1995, 117, 3–20. [Google Scholar] [CrossRef]
- Robinson, E.; Roberts, C.; Vainik, U.; Estonia, T.; Jones, A. The psychology of obesity: An umbrella review and evidence-based map of the psychological correlates of heavier body weight. Neurosci. Biobehav. Rev. 2020, 119, 468–480. [Google Scholar] [CrossRef]
- Bourdier, L.; Fatseas, M.; Maria, A.S.; Carre, A.; Berthoz, S. The psycho-affective roots of obesity: Results from a french study in the general population. Nutrients 2020, 12, 2962. [Google Scholar] [CrossRef]
- Hruby, A.; Hu, F.B. The epidemiology of obesity: A big picture. Pharmacoeconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Ishihara, B.P.; Farah, D.; Fonseca, M.C.; Nazario, A. The risk of developing breast, ovarian, and endometrial cancer in obese women submitted to bariatric surgery: A meta-analysis. Surg. Obes. Relat. Dis. 2020, 16, 1596–1602. [Google Scholar] [CrossRef]
- Tsekrekos, A.; Lovece, A.; Chrysikos, D.; Ndegwa, N.; Schizas, D.; Kumagai, K.; Rouvelas, I. Impact of obesity on the outcomes after gastrectomy for gastric cancer: A meta-analysis. Asian J. Surg. 2021, 45, 15–26. [Google Scholar] [CrossRef]
- Markowitz, S.; Friedman, M.A.; Arent, S.M. Understanding the relation between obesity and depression: Causal mechanisms and implications for treatment. Clin. Psychol. Sci. Pract. 2008, 15, 1–20. [Google Scholar] [CrossRef]
- Pereira-Miranda, E.; Costa, P.R.; Queiroz, V.A.; Pereira-Santos, M.; Santana, M.L. Overweight and obesity associated with higher depression prevalence in adults: A systematic review and meta-analysis. J. Am. Coll. Nutr. 2017, 36, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Preiss, K.; Brennan, L.; Clarke, D. A systematic review of variables associated with the relationship between obesity and depression. Obes. Rev. 2013, 14, 906–918. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.T.; Nguyet, N.T.M.; Nga, V.T.; Lien, N.V.T.; Vo, D.D.; Lien, N.; Ngoc, V.T.N.; Son, L.H.; Le, D.H.; Nga, V.B.; et al. An update on obesity: Mental consequences and psychological interventions. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 155–160. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 2 December 2021).
- Gaesser, G.A.; Angadi, S.S. Obesity treatment: Weight loss versus increasing fitness and physical activity for reducing health risks. Iscience 2021, 24, 102995. [Google Scholar] [CrossRef]
- Hoare, E.; Collins, S.; Marx, W.; Callaly, E.; Moxham-Smith, R.; Cuijpers, P.; Holte, A.; Nierenberg, A.A.; Reavley, N.; Christensen, H.; et al. Universal depression prevention: An umbrella review of meta-analyses. J. Psychiatr. Res. 2021, 144, 483–493. [Google Scholar] [CrossRef]
- Papadopoulos, S.; Brennan, L. Correlates of weight stigma in adults with overweight and obesity: A systematic literature review. Obesity 2015, 23, 1743–1760. [Google Scholar] [CrossRef] [Green Version]
- De Wit, L.; Luppino, F.; van Straten, A.; Penninx, B.; Zitman, F.; Cuijpers, P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Res. 2010, 178, 230–235. [Google Scholar] [CrossRef]
- Faith, M.S.; Butryn, M.; Wadden, T.A.; Fabricatore, A.; Nguyen, A.M.; Heymsfield, S.B. Evidence for prospective associations among depression and obesity in population-based studies. Obes. Rev. 2011, 12, e438–e453. [Google Scholar] [CrossRef]
- González-Castro, T.B.; Escobar-Chan, Y.M.; Fresan, A.; López-Narváez, M.L.; Tovilla-Zárate, C.A.; Juárez-Rojop, I.E.; Ble-Castillo, J.L.; Genis-Mendoza, A.D.; Arias-Vázquez, P.I. Higher risk of depression in individuals with type 2 diabetes and obesity: Results of a meta-analysis. J. Health Psychol. 2019, 16, 1404–1419. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.J.; Woo, H.T.; Cho, S.; Park, K.; Jeong, S.; Lee, Y.J.; Kang, D.; Shin, A. Association between body size, weight change and depression: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 211, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Atlantis, E.; Baker, M. Obesity effects on depression: Systematic review of epidemiological studies. Int. J. Obes. 2008, 32, 881–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Chen, D.; Ruan, W.; Peng, Y.; Lu, Z.; Wang, D. Associations of depression, sleep disorder with total and cause-specific mortality: A prospective cohort study. J. Affect. Disord. 2022, 298, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Tubbs, A.S.; Khader, W.; Fernandez, F.; Grandner, M.A. The common denominators of sleep, obesity, and psychopathology. Curr. Opin. Psychol. 2020, 34, 84–88. [Google Scholar] [CrossRef]
- Chireh, B.; D’Arcy, C. Shared and unique risk factors for depression and diabetes mellitus in a longitudinal study, implications for prevention: An analysis of a longitudinal population sample aged ≥ 45 years. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819865828. [Google Scholar] [CrossRef] [Green Version]
- Fulton, S.; Décarie-Spain, L.; Fioramonti, X.; Guiard, B.; Nakajima, S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol. Metab. 2022, 33, 18–35. [Google Scholar] [CrossRef]
- Haregu, T.N.; Lee, J.T.; Oldenburg, B.; Armstrong, G. Comorbid Depression and Obesity: Correlates and Synergistic Association With Noncommunicable Diseases Among Australian Men. Prev. Chronic. Dis. 2020, 17, 190420. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Foster, G.D.; Kendall, P.C. The realistic treatment of obesity: Changing the scales of success. Clin. Psychol. Rev. 1994, 14, 701–736. [Google Scholar] [CrossRef]
- Konttinen, H.; Kiviruusu, O.; Huurre, T.; Haukkala, A.; Aro, H.; Marttunen, M. Longitudinal associations between depressive symptoms and body mass index in a 20-year follow-up. Int. J. Obes. 2014, 38, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Aldenderfer, M.; Blashfield, R.K. Cluster Analysis; Sage: Newbury Park, CA, USA, 1984. [Google Scholar]
- Wu, Y.P.; Steele, R.G. Predicting health-related quality of life from the psychosocial profiles of youth seeking treatment for obesity. J. Dev. Behav. Pediatrics 2013, 34, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A.; Staniszewska, A.; Hallit, S. Identifying the profile of orthorexic behavior and “normal” eating behavior with cluster analysis: A cross-sectional study among polish adults. Nutrients 2020, 12, 3490. [Google Scholar] [CrossRef] [PubMed]
- Chapuis-de-Andrade, S.; Moret-Tatay, C.; de Paula, T.A.; Irigaray, T.Q.; Antonello, I.C.F.; da Costa, B.E.P. Psychological factors and coping strategies in pregnancies complicated by hypertension: A cluster-analytic approach. J. Affect. Disord. 2022, 296, 89–94. [Google Scholar] [CrossRef]
- Décamps, G.; Idier, L.; Battaglia, N. Personnalité et profils addictifs: Étude des consommations de substances et des pratiques comportementales addictives en population étudiante. J. Thérapie Comport. Cogn. 2013, 23, 73–80. [Google Scholar] [CrossRef]
- Rebetez, M.M.L.; Rochat, L.; Van der Linden, M. Cognitive, emotional, and motivational factors related to procrastination: A cluster analytic approach. Personal. Individ. Differ. 2015, 76, 1–6. [Google Scholar] [CrossRef]
- Berlin, K.S.; Kamody, R.C.; Thurston, I.B.; Banks, G.G.; Rybak, T.M.; Ferry, R.J., Jr. Physical activity, sedentary behaviors, and nutritional risk profiles and relations to body mass index, obesity, and overweight in eighth grade. Behav. Med. 2017, 43, 31–39. [Google Scholar] [CrossRef]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Adair, L.S. Obesogenic clusters: Multidimensional adolescent obesity-related behaviors in the US. Ann. Behav. Med. 2008, 36, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Boutelle, K.N.; Peterson, C.B.; Crosby, R.D.; Rydell, S.A.; Zucker, N.; Harnack, L. Overeating phenotypes in overweight and obese children. Appetite 2014, 76, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Braet, C.; Beyers, W.; Goossens, L.; Verbeken, S.; Moens, E. Subtyping children and adolescents who are overweight based on eating pathology and psychopathology. Eur. Eat. Disord. Rev. 2012, 20, 279–286. [Google Scholar] [CrossRef]
- De Carvalho-Ferreira, J.P.; Finlayson, G.; da Cunha, D.T.; Caldas, G.; Bandoni, D.; de Rosso, V.V. Adiposity and binge eating are related to liking and wanting for food in Brazil: A cultural adaptation of the Leeds Food Preference Questionnaire. Appetite 2019, 133, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, V.B.; Da Silva, R.B.; Prud’Homme, A.; Campan, P.; Azorin, J.M.; Belzeaux, R. Association between binge eating disorder and psychiatric comorbidity profiles in patients with obesity seeking bariatric surgery. Compr. Psychiatry 2018, 87, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Daw, J.; Margolis, R.; Wright, L. Emerging adulthood, emergent health lifestyles: Sociodemographic determinants of trajectories of smoking, binge drinking, obesity, and sedentary behavior. J. Health Soc. Behav. 2017, 58, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Leslie, M.; Turton, R.; Burgess, E.; Nazar, B.P.; Treasure, J. Testing the addictive appetite model of binge eating: The importance of craving, coping, and reward enhancement. Eur. Eat. Disord. Rev. 2018, 26, 541–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manta, S.W.; Sandreschi, P.F.; Matias, T.S.; Tomicki, C.; Benedetti, T.R. Clustering of physical activity and sedentary behavior associated to risk for metabolic syndrome in older adults. J. Aging Phys. Act. 2019, 27, 781–786. [Google Scholar] [CrossRef]
- Romain, A.J.; Avignon, A.; Macioce, V.; Boegner, C.; Attalin, A.; Sultan, A. Patterns of eating behavior in people with severe obesity seeking weight loss treatment: An exploratory study. Appetite 2021, 169, 105797. [Google Scholar] [CrossRef]
- Claes, L.; Vandereycken, W.; Vandeputte, A.; Braet, C. Personality subtypes in female pre-bariatric obese patients: Do they differ in eating disorder symptoms, psychological complaints and coping behaviour? Eur. Eat. Disord. Rev. 2013, 21, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Gagnon-Girouard, M.P.; Bégin, C.; Provencher, V.; Tremblay, A.; Boivin, S.; Lemieux, S. Subtyping weight-preoccupied overweight/obese women along restraint and negative affect. Appetite 2010, 55, 742–745. [Google Scholar] [CrossRef]
- Gullo, S.; Lo Coco, G.; Salerno, L.; La Pietra, F.; Bruno, V. A study of personality subtypes in obese patients seeking treatment. Res. Psychother. Psychopathol. Process Outcome 2013, 16, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Jansen, A.; Havermans, R.; Nederkoorn, C.; Roefs, A. Jolly fat or sad fat? Subtyping non-eating disordered overweight and obesity along an affect dimension. Appetite 2008, 51, 635–640. [Google Scholar] [CrossRef]
- Leombruni, P.; Rocca, G.; Fassino, S.; Gastaldi, F.; Nicotra, B.; Siccardi, S.; Lavagnino, L. An exploratory study to subtype obese binge eaters by personality traits. Psychother. Psychosom. 2014, 83, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Lo Coco, G.; Gullo, S.; Scrima, F.; Bruno, V. Obesity and interpersonal problems: An analysis with the interpersonal circumplex. Clin. Psychol. Psychother. 2012, 19, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Guerra, L.S.; Coêlho, B.M.; Santo, M.A.; Lotufo-Neto, F.; Wang, Y.P. Gender-related patterns of psychiatric disorder clustering among bariatric surgery candidates: A latent class analysis. J. Affect. Disord. 2018, 240, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Claes, L.; Wilderjans, T.F.; De Zwaan, M. Temperament subtypes in treatment seeking obese individuals: A latent profile analysis. Eur. Eat. Disord. Rev. 2014, 22, 260–266. [Google Scholar] [CrossRef]
- Claes, L.; Boekaerts, E.; Verschueren, M.; Boukaert, W.; Luyckx, K. Identity statuses in prebariatric patients with obesity: Associations with eating disorder symptoms, psychological complaints, and coping behaviour? Eur. Eat. Disord. Rev. 2019, 27, 410–420. [Google Scholar] [CrossRef]
- Plasonja, N.; Brytek-Matera, A.; Décamps, G. French validation of the Weight Efficacy Life-Style questionnaire (WEL): Links with mood, self-esteem and stress among the general population and a clinical sample of individuals with overweight and obesity. PLoS ONE 2021, 16, e0259885. [Google Scholar] [CrossRef]
- Clark, M.M.; Abrams, D.B.; Niaura, R.S.; Eaton, C.A.; Rossi, J.S. Self-efficacy in weight management. J. Consult. Clin. Psychol. 1991, 59, 739–744. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Polivy, J. Development and validation of a scale for measuring state self-esteem. J. Personal. Soc. Psychol. 1991, 60, 895–910. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lesage, F.X.; Berjot, S.; Deschamps, F. Psychometric properties of the French versions of the Perceived Stress Scale. Int. J. Occup. Med. Environ. Health 2012, 25, 178–184. [Google Scholar]
- Plasonja, N.; Villemur, E.; Ostermann, G.; Dubourdeaux, M.; Bocandé, E.; Blondeau, C.; Décamps, G. Creation and French validation of a physical hunger scale [Création et validation en français d’une échelle de faim physique] [Poster presentation]. In Proceedings of the 15th French General Practice Conference, Paris, France, 24–26 March 2022; Available online: https://www.congresmg.fr/programme-2022 (accessed on 9 March 2022).
- Bruchon-Schweitzer, M. Dimensionality of the Body Image: The BIQ. Percept. Mot. Ski. 1987, 65, 887–892. [Google Scholar] [CrossRef]
- Koleck, M.; Bruchon-Schweitzer, M.; Cousson-Gélie, F.; Gilliard, J.; Quintard, B. The body-image questionnaire: An extension. Percept. Mot. Ski. 2002, 94, 189–196. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Regional Office for Europe. Well-Being Measures in Primary Health Care/The DepCare Project: Report on a WHO Meeting. 1998. Available online: http://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf (accessed on 16 December 2020).
- Olsen, L.R.; Jensen, D.V.; Noerholm, V.; Martiny, K.; Bech, P. The internal and external validity of the Major Depression Inventory in measuring severity of depressive states. Psychol. Med. 2003, 33, 351–356. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Process of Translation and Adaptation of Instruments. Available online: https://www.who.int/substance_abuse/research_tools/translation/en/# (accessed on 14 January 2020).
- Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 9 March 2022).
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Wierzchoń, S.T.; Kłopotek, M.A. Modern Algorithms of Cluster Analysis; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- MacQueen, J. Some methods for classification and analysis of multivariate observations. In Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability; University of California Press: Berkeley, CA, USA, 1967; Volume 1, pp. 281–297. [Google Scholar]
- Kassambara, A. Practical Guide to Cluster Analysis in R: Unsupervised Machine Learning; STHDA, 2017; Volume 1, ISBN 1542462703/978-1542462709. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Blüher, S.; Schwarz, P. Metabolically healthy obesity from childhood to adulthood—Does weight status alone matter? Metabolism 2014, 63, 1084–1092. [Google Scholar] [CrossRef]
- Hinnouho, G.M.; Singh-Manoux, A.; Gueguen, A.; Matta, J.; Lemogne, C.; Goldberg, M.; Zins, M.; Czernichow, S. Metabolically healthy obesity and depressive symptoms: 16-year follow-up of the Gazel cohort study. PLoS ONE 2017, 12, e0174678. [Google Scholar] [CrossRef]
- Mehrabi, F.; Amiri, P.; Cheraghi, L.; Kheradmand, A.; Hosseinpanah, F.; Azizi, F. Emotional states of different obesity phenotypes: A sex-specific study in a west-Asian population. BMC Psychiatry 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Phillips, C.M.; Perry, I.J. Depressive symptoms, anxiety and well-being among metabolic health obese subtypes. Psychoneuroendocrinology 2015, 62, 47–53. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Pietrabissa, G.; Manzoni, G.M.; Cattivelli, R.; Rossi, A.; Novelli, M.; Varallo, G.; Molinari, E. Cognitive behavioral therapy to aid weight loss in obese patients: Current perspectives. Psychol. Res. Behav. Manag. 2017, 10, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Beintner, I.; Emmerich, O.L.M.; Vollert, B.; Taylor, C.B.; Jacobi, C. Promoting positive body image and intuitive eating in women with overweight and obesity via an online intervention: Results from a pilot feasibility study. Eat. Behav. 2019, 34, 101307. [Google Scholar] [CrossRef]
- Pinto-Gouveia, J.; Carvalho, S.A.; Palmeira, L.; Castilho, P.; Duarte, C.; Ferreira, C.; Duarte, J.; Cunha, M.; Matos, M.; Costa, J. BEfree: A new psychological program for binge eating that integrates psychoeducation, mindfulness, and compassion. Clin. Psychol. Psychother. 2017, 24, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Turk, F.; Waller, G. Is self-compassion relevant to the pathology and treatment of eating and body image concerns? A systematic review and meta-analysis. Clin. Psychol. Rev. 2020, 79, 101856. [Google Scholar] [CrossRef] [PubMed]
- Latner, J.D.; Ciao, A.C.; Wendicke, A.U.; Murakami, J.M.; Durso, L.E. Community-based behavioral weight-loss treatment: Long-term maintenance of weight loss, physiological, and psychological outcomes. Behav. Res. Ther. 2013, 51, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Wharton, S.; Lau, D.C.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Adamo, K.; Alberga, A.; Bell, R.; Boulé, N.; et al. Obesity in adults: A clinical practice guideline. Cmaj 2020, 192, E875–E891. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, L.; Cunha, M.; Pinto-Gouveia, J. Processes of change in quality of life, weight self-stigma, body mass index and emotional eating after an acceptance-, mindfulness-and compassion-based group intervention (Kg-Free) for women with overweight and obesity. J. Health Psychol. 2019, 24, 1056–1069. [Google Scholar] [CrossRef]
- Elliott, M.; Gillison, F.; Barnett, J. Exploring the influences on men’s engagement with weight loss services: A qualitative study. BMC Public Health 2020, 20, 249. [Google Scholar] [CrossRef] [Green Version]
- Pagoto, S.L.; Schneider, K.L.; Oleski, J.L.; Luciani, J.M.; Bodenlos, J.S.; Whited, M.C. Male inclusion in randomized controlled trials of lifestyle weight loss interventions. Obesity 2012, 20, 1234–1239. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Assessment Scale | Cronbach’s Alpha Values | |
|---|---|---|
| Female Subsample (n = 1427) | Male Subsample (n = 310) | |
| WEL-Fr-C | 0.91 | 0.91 |
| External i | 0.89 | 0.88 |
| Internal | 0.91 | 0.91 |
| SSES | 0.84 | 0.84 |
| Appearance | 0.82 | 0.84 |
| Social | 0.79 | 0.79 |
| Performance | 0.82 | 0.84 |
| MDI | 0.83 a | 0.81 b |
| WHO-5 | 0.88 | 0.89 |
| Physical hunger | 0.84 | 0.82 |
| PSS-11 | 0.87 | 0.89 |
| BIQ | 0.89 | 0.91 |
| Variable | Female Subsample (n = 1427) | Male Subsample (n = 310) | U (1735) |
| Age | 44.4 (11.26) | 44.64 (11.19) | 217,560 |
| BMI | 32.26 (5.63) | 32.47 (5.59) | 215,376 |
| WEL-Fr-C | 58.49 (20.64) | 59.33 (20.15) | 217,556 |
| External | 34.22 (11.62) | 34.22 (11.62) | 219,442 |
| Internal | 24.27 (12.04) | 24.84 (11.89) | 215,583 |
| SSES | 43.94 (9.53) | 44.95 (9.49) | 206,266 |
| Appearance | 7.95 (3.92) | 8.35 (3.95) | 206,888 |
| Social | 25.08 (5.28) | 25.39 (5.36) | 213,725 |
| Performance | 10.91 (3.79) | 11.21 (3.70) | 209,931 |
| WHO-5 | 51.24 (23.06) | 52.39 (22.55) | 215,230 |
| Physical hunger | 21.72 (6.29) | 21.42 (5.89) | 226,789 |
| PSS-11 | 31.65 (7.87) | 31.04 (7.82) | 230,984 |
| BIQ | 55.85 (12.51) | 56.85 (13.34) | 209,886 |
| Variable | Female Subsample (n = 797) | Male Subsample (n = 170) | U (965) |
| MDI | 23.56 (8.85) | 22.69 (8.36) | 71,550 |
| Assessment Scale | Cluster 1 | Cluster 2 | Cluster 3 | Kruskal-Wallis | Eta2 |
| WEL-Internal | −0.71 (0.82) a | 0.08 (0.83) b | 0.96 (0.65) c | 535.49 *** | 0.38 |
| WEL-External | −0.64(0.94) a | 0.11 (0.84) b | 0.78 (0.70) c | 406.90 *** | 0.28 |
| SSES-Appearance | −0.56 (0.60) a | −0.16 (0.75) b | 1.20 (0.95) c | 539.39 *** | 0.43 |
| SSES-Social | −0.46 (0.94) a | 0.07 (0.88) b | 0.58 (0.98) c | 201.43 *** | 0.15 |
| SSES-Performance | −0.86 (0.87) a | 0.24 (0.70) b | 0.85 (0.65) c | 629.49 *** | 0.43 |
| Physical hunger | 0.80 (0.81) a | −0.14 (0.76) b | −0.96 (0.64) c | 624.01 *** | 0.43 |
| BIQ | −0.79 (0.75) a | 0.08 (0.72) b | 1.07 (0.71) c | 679.24 *** | 0.47 |
| PSS-11 | 0.85 (0.70) a | −0.14 (0.71) b | −1.05 (0.73) c | 721.57 *** | 0.49 |
| Cluster 1 | Cluster 2 | Cluster 3 | Kruskal-Wallis | Eta2 | |
|---|---|---|---|---|---|
| WEL-Internal | −0.80 (0.77) a | −0.09 (0.77) b | 1.07(0.64) c | 137.73 *** | 0.45 |
| WEL-External | −0.58 (0.93) a | −0.18 (0.85) b | 0.99 (0.56) c | 114.09 *** | 0.34 |
| SSES-Appearance | −0.77 (0.47) a | −0.08 (0.74) b | 1.01 (1.05) c | 120.83 *** | 0.41 |
| SSES-Social | −0.50 (0.90) a | 0.13 (0.98) b | 0.30 (0.95) b, c | 31.34 *** | 0.098 |
| SSES-Performance | −1.03 (0.87) a | 0.13 (0.68) b | 0.87 (0.63) c | 145.87 *** | 0.48 |
| Physical hunger | 0.92 (0.82) a | −0.02 (0.72) b | −0.98 (0.67) c | 143.94 *** | 0.46 |
| BIQ | −1.08 (0.65) a | 0.10 (0.71) b | 0.99 (0.61) c | 174.24 *** | 0.55 |
| PSS-11 | 1.08 (0.59) a | −0.10 (0.67) b | −0.99 (0.74) c | 174.24 *** | 0.55 |
| Variable | Cluster 1 | Cluster 2 | Cluster 3 | Kruskal-Wallis | Eta2 |
|---|---|---|---|---|---|
| Age | 44.13 (11.09) a | 43.81 (11.66) a,b | 46.02 (10.58) c | 7.67 * | 0.006 |
| BMI | 32.26 (5.59) | 32.44 (5.77) | 31.86 (5.39) | 1.79 | |
| WHO-5 | 33.82 (18.46) a | 53.83 (18.20) b | 73.30 (16.16) c | 574.56 ** | 0.40 |
| MDI | 27.96 (8.01) a | 19.68 (6.76) b | 13.53 (6.75) c | 242.41 ** | 0.30 |
| Cluster 1 | Cluster 2 | Cluster 3 | Kruskal-Wallis | Eta2 | |
|---|---|---|---|---|---|
| Age | 43.16 (10.75) | 45.02 (11.10) | 45.49 (11.84) | 2.79 | |
| BMI | 33.66 (6.76) | 31.99 (4.91) | 32.12 (5.32) | 2.86 | |
| WHO-5 | 31.05 (16.23) a | 54.08 (17.62) b | 72.53 (16.46) c | 132.86 *** | 0.44 |
| MDI | 28.69 (6.59) a | 18.43 (6.38) b | 15.21 (5.52) b | 71.69 *** | 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plasonja, N.; Brytek-Matera, A.; Décamps, G. Psychological Profiles of Treatment-Seeking Adults with Overweight and Obesity: A Cluster Analysis Approach. J. Clin. Med. 2022, 11, 1952. https://doi.org/10.3390/jcm11071952
Plasonja N, Brytek-Matera A, Décamps G. Psychological Profiles of Treatment-Seeking Adults with Overweight and Obesity: A Cluster Analysis Approach. Journal of Clinical Medicine. 2022; 11(7):1952. https://doi.org/10.3390/jcm11071952
Chicago/Turabian StylePlasonja, Natalija, Anna Brytek-Matera, and Greg Décamps. 2022. "Psychological Profiles of Treatment-Seeking Adults with Overweight and Obesity: A Cluster Analysis Approach" Journal of Clinical Medicine 11, no. 7: 1952. https://doi.org/10.3390/jcm11071952