
Sex-Specific Risk Factors for Short- and Long-Term Outcomes after Surgery in Patients with Infective Endocarditis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
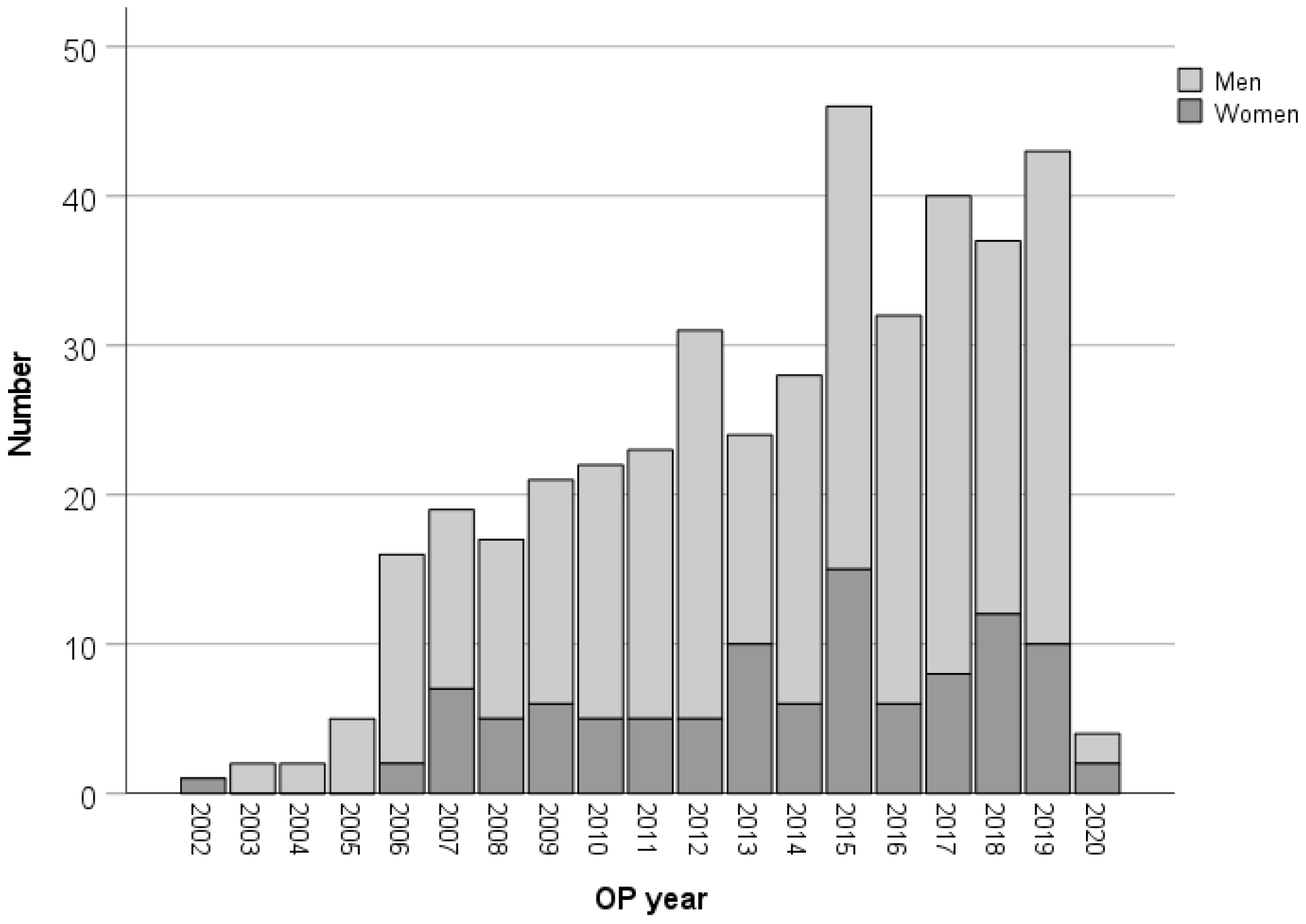
2.1. Patients and Study Design
2.2. Patient Management
2.3. Surgical Procedure
2.4. Statistical Analysis
3. Results
3.1. Demographics and Clinical Details of the Study Population
3.2. Univariate Association to 30-Day Mortality
3.3. Independent Predictors for 30 Day Mortality
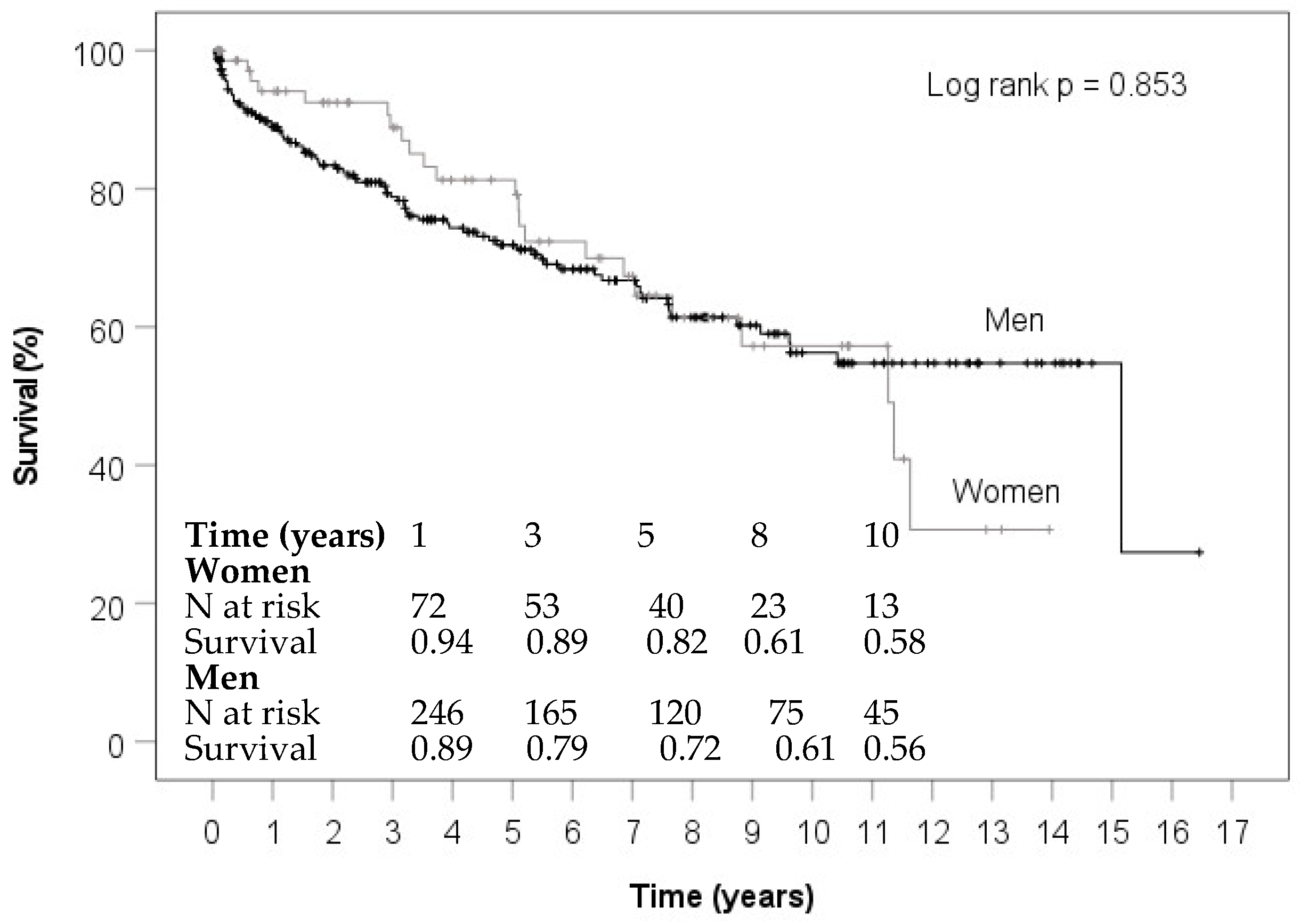
3.4. Survival Analysis
3.5. Risk Factors for Long-Term Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cresti, A.; Chiavarelli, M.; Scalese, M.; Nencioni, C.; Valentini, S.; Guerrini, F.; D’Aiello, I.; Picchi, A.; De Sensi, F.; Habib, G. Epidemiological and mortality trends in infective endocarditis, a 17-year population-based prospective study. Cardiovasc. Diagn. Ther. 2017, 7, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elamragy, A.A.; Meshaal, M.S.; El-Kholy, A.A.; Rizk, H.H. Gender differences in clinical features and complications of infective endocarditis: 11-year experience of a single institute in Egypt. Egypt. Heart J. 2020, 72, 5. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, C.; Nogueira, P.; Pinto, F.J. Insight into the epidemiology of infective endocarditis in Portugal: A contemporary nationwide study from 2010 to 2018. BMC Cardiovasc. Disord. 2021, 21, 138. [Google Scholar] [CrossRef] [PubMed]
- Ahtela, E.; Oksi, J.; Porela, P.; Ekström, T.; Rautava, P.; Kytö, V. Trends in occurrence and 30-day mortality of infective endocarditis in adults: Population-based registry study in Finland. BMJ Open 2019, 9, e026811. [Google Scholar] [CrossRef]
- Thornhill, M.H.; Jones, S.; Prendergast, B.; Baddour, L.M.; Chambers, J.B.; Lockhart, P.B.; Dayer, M.J. Quantifying infective endocarditis risk in patients with predisposing cardiac conditions. Eur. Heart J. 2018, 39, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Rajani, R.; Klein, J.L. Infective endocarditis: A contemporary update. Clin. Med. 2020, 20, 31–35. [Google Scholar] [CrossRef]
- Aksoy, O.; Meyer, L.T.; Cabell, C.H.; Kourany, W.M.; Pappas, P.A.; Sexton, D.J. Gender differences in infective endocarditis: Pre- and co-morbid conditions lead to different management and outcomes in female patients. Scand. J. Infect. Dis. 2007, 39, 101–107. [Google Scholar] [CrossRef]
- Sambola, A.; Fernández-Hidalgo, N.; Almirante, B.; Roca, I.; González-Alujas, T.; Serra, B.; Pahissa, A.; García-Dorado, D.; Tornos, P. Sex differences in native-valve infective endocarditis in a single tertiary-care hospital. Am. J. Cardiol. 2010, 106, 92–98. [Google Scholar] [CrossRef]
- Slipczuk, L.; Codolosa, J.N.; Davila, C.D.; Romero-Corral, A.; Yun, J.; Pressman, G.S.; Figueredo, V.M. Infective endocarditis epidemiology over five decades: A systematic review. PLoS ONE 2013, 8, e82665. [Google Scholar] [CrossRef]
- Vincent, L.L.; Otto, C.M. Infective Endocarditis: Update on Epidemiology, Outcomes, and Management. Curr. Cardiol. Rep. 2018, 20, 86. [Google Scholar] [CrossRef]
- Dohmen, P.M.; Binner, C.; Mende, M.; Daviewala, P.; Etz, C.D.; Borger, M.A.; Misfeld, M.; Eifert, S.; Mohr, F.W. Gender-Based Long-Term Surgical Outcome in Patients with Active Infective Aortic Valve Endocarditis. Med. Sci. Monit. 2016, 22, 2520–2527. [Google Scholar] [CrossRef] [Green Version]
- Varela Barca, L.; Vidal-Bonnet, L.; Fariñas, M.C.; Muñoz, P.; Valerio Minero, M.; de Alarcón, A.; Gutiérrez Carretero, E.; Gutiérrez Cuadra, M.; Moreno Camacho, A.; Kortajarena Urkola, X.; et al. Analysis of sex differences in the clinical presentation, management and prognosis of infective endocarditis in Spain. Heart 2021, 107, 1717–1724. [Google Scholar] [CrossRef]
- Polishchuk, I.; Stavi, V.; Awesat, J.; Ben Baruch Golan, Y.; Bartal, C.; Sagy, I.; Jotkowitz, A.; Barski, L. Sex Differences in Infective Endocarditis. Am. J. Med. Sci. 2021, 361, 83–89. [Google Scholar] [CrossRef]
- van den Brink, F.S.; Swaans, M.J.; Hoogendijk, M.G.; Alipour, A.; Kelder, J.C.; Jaarsma, W.; Eefting, F.D.; Groenmeijer, B.; Kupper, A.J.F.; Ten Berg, J.M. Increased incidence of infective endocarditis after the 2009 European Society of Cardiology guideline update: A nationwide study in the Netherlands. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Varela Barca, L.; Navas Elorza, E.; Fernández-Hidalgo, N.; Moya Mur, J.L.; Muriel García, A.; Fernández-Felix, B.M.; Miguelena Hycka, J.; Rodríguez-Roda, J.; López-Menéndez, J. Prognostic factors of mortality after surgery in infective endocarditis: Systematic review and meta-analysis. Infection 2019, 47, 879–895. [Google Scholar] [CrossRef]
- Weber, C.; Gassa, A.; Rokohl, A.; Sabashnikov, A.; Deppe, A.C.; Eghbalzadeh, K.; Merkle, J.; Hamacher, S.; Liakopoulos, O.J.; Wahlers, T. Severity of Presentation, Not Sex, Increases Risk of Surgery for Infective Endocarditis. Ann. Thorac. Surg. 2019, 107, 1111–1117. [Google Scholar] [CrossRef]
- Castillo, J.C.; Anguita, M.P.; Delgado, M.; Ruiz, M.; Mesa, D.; Romo, E.; Crespín, M.; García, D.; Arizón, J.M.; Suárez de Lezo, J. Clinical characteristics and prognosis of infective endocarditis in women. Rev. Esp. Cardiol. 2008, 61, 36–40. [Google Scholar] [CrossRef]
- Curlier, E.; Hoen, B.; Alla, F.; Selton-Suty, C.; Schubel, L.; Doco-Lecompte, T.; Minary, L.; Erpelding, M.L.; Duval, X.; Chirouze, C. Relationships between sex, early valve surgery and mortality in patients with left-sided infective endocarditis analysed in a population-based cohort study. Heart 2014, 100, 1173–1178. [Google Scholar] [CrossRef]
- Friedrich, C.; Salem, M.; Panholzer, B.; Cremer, J.; Haneya, A. Geschlechtsspezifische Ergebnisse nach operativer Therapie bei infektiöser Endokarditis. CHAZ 2021, 22, 35–39. [Google Scholar]
- Salem, M.; Friedrich, C.; Saad, M.; Frank, D.; Salem, M.; Puehler, T.; Schoettler, J.; Schoeneich, F.; Cremer, J.; Haneya, A. Active Infective Native and Prosthetic Valve Endocarditis: Short- and Long-Term Outcomes of Patients after Surgical Treatment. J. Clin. Med. 2021, 10, 1868. [Google Scholar] [CrossRef] [PubMed]
- Roques, F.; Michel, P.; Goldstone, A.R.; Nashef, S.A. The logistic EuroSCORE. Eur. Heart J. 2003, 24, 881–882. [Google Scholar] [CrossRef]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardiothorac. Surg. 2012, 41, 734–744, discussion 744–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaudszun, G.; Munting, K.E.; Butchart, A.; Gerrard, C.; Klein, A.A. The association between borderline pre-operative anaemia in women and outcomes after cardiac surgery: A cohort study. Anaesthesia 2018, 73, 572–578. [Google Scholar] [CrossRef] [Green Version]
- Faerber, G.; Zacher, M.; Reents, W.; Boergermann, J.; Kappert, U.; Boening, A.; Diegeler, A.; Doenst, T. Female sex is not a risk factor for post procedural mortality in coronary bypass surgery in the elderly: A secondary analysis of the GOPCABE trial. PLoS ONE 2017, 12, e0184038. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, C.; Salem, M.A.; Puehler, T.; Hoffmann, G.; Lutter, G.; Cremer, J.; Haneya, A. Sex-specific risk factors for early mortality and survival after surgery of acute aortic dissection type a: A retrospective observational study. J. Cardiothorac. Surg. 2020, 15, 145. [Google Scholar] [CrossRef]
- Wang, H.; Guo, X.; Zhu, X.; Li, Y.; Jia, Y.; Zhang, Z.; Yuan, S.; Yan, F. Gender Differences and Postoperative Delirium in Adult Patients Undergoing Cardiac Valve Surgery. Front. Cardiovasc. Med. 2021, 8, 751421. [Google Scholar] [CrossRef]
- Koster, S.; Hensens, A.G.; Schuurmans, M.J.; van der Palen, J. Risk factors of delirium after cardiac surgery: A systematic review. Eur. J. Cardiovasc. Nurs. 2011, 10, 197–204. [Google Scholar] [CrossRef]
- Kumar, A.K.; Jayant, A.; Arya, V.K.; Magoon, R.; Sharma, R. Delirium after cardiac surgery: A pilot study from a single tertiary referral center. Ann. Card. Anaesth. 2017, 20, 76–82. [Google Scholar]
- Mohanan, S.; Gopalan Nair, R.; Vellani, H.; Sajeev, C.G.; George, B.; Krishnan, M.N. Baseline C-reactive protein levels and prognosis in patients with infective endocarditis: A prospective cohort study. Indian Heart J. 2018, 70 (Suppl. 3), S43–S49. [Google Scholar] [CrossRef]
- Salsano, A.; Giacobbe, D.R.; Del Puente, F.; Natali, R.; Miette, A.; Moscatelli, S.; Perocchio, G.; Scarano, F.; Porto, I.; Mariscalco, G.; et al. Culture-negative infective endocarditis (CNIE): Impact on postoperative mortality. Open Med. 2020, 15, 571–579. [Google Scholar] [CrossRef]
- Liang, F.; Song, B.; Liu, R.; Yang, L.; Tang, H.; Li, Y. Optimal timing for early surgery in infective endocarditis: A meta-analysis. Interact Cardiovasc Thorac. Surg. 2016, 22, 336–345. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Overall (n = 413) | Men (n = 308, 74.6%) | Women (n = 105, 25.4%) | p-Value |
|---|---|---|---|---|
| Age, years | 64 (52;73) | 64 (50;73) | 65 (57;75) | 0.082 |
| Body mass index (kg/m2) | 25.9 (23.0;29.4) | 25.7 (23.0;29.0) | 26.1 (23.0;30.8) | 0.223 |
| Body mass index > 30 (kg/m2) | 92 (22.4%) | 63 (20.6%) | 29 (27.6%) | 0.136 |
| Logistic EuroSCORE | 27.2 (12.5;49.1) | 24.8 (11.7;45.6) | 35.7 (14.6;53.6) | 0.054 |
| EuroSCORE II | 12.1 (5.2;27.3) | 11.6 (5.0;25.2) | 16.3 (6.1;30.8) | 0.127 |
| Co-morbidity | ||||
| COPD | 50 (12.1%) | 37 (12.0%) | 13 (12.4%) | 0.920 |
| Arterial hypertension | 240 (58.1%) | 177 (57.5%) | 63 (60.0%) | 0.650 |
| Pulmonary hypertension (>25 mmHg) | 86 (20.9%) | 60 (19.5%) | 26 (25.0%) | 0.231 |
| Atrial fibrillation | 81 (19.6%) | 61 (19.8%) | 20 (19.0%) | 0.866 |
| Peripheral vascular disease | 36 (8.7%) | 28 (9.1%) | 8 (7.6%) | 0.644 |
| Type 1 Diabetes mellitus | 3 (0.7%) | 2 (0.6%) | 1 (1.0%) | 1.000 |
| Type 2 Diabetes mellitus | 83 (20.1%) | 58 (18.8%) | 25 (23.8%) | 0.272 |
| IDDM | 45 (10.9%) | 30 (9.7%) | 15 (14.3%) | 0.197 |
| Hyperlipoproteinemia | 116 (28.1%) | 82 (26.6%) | 34 (32.4%) | 0.257 |
| Dialysis (acute and chronic) | 45 (10.9%) | 32 (10.4%) | 13 (12.4%) | 0.572 |
| Acute renal insufficiency | 53 (12.8%) | 42 (13.6%) | 11 (10.5%) | 0.403 |
| Chronic dialysis preoperative | 18 (4.4%) | 11 (3.6%) | 7 (6.7%) | 0.177 |
| Chronic renal insufficiency | 116 (28.1%) | 92 (29.9%) | 24 (22.9%) | 0.167 |
| NYHA IV | 83 (20.2%) | 65 (21.2%) | 18 (17.3%) | 0.388 |
| Tumor | 55 (13.3%) | 40 (13.0%) | 15 (14.3%) | 0.735 |
| Rheumatic disease | 23 (5.6%) | 16 (5.2%) | 7 (6.7%) | 0.570 |
| History of liver disease | 55 (13.3%) | 42 (13.7%) | 13 (12.4%) | 0.735 |
| Drug abuse | 23 (5.6%) | 16 (5.2%) | 7 (6.7%) | 0.570 |
| Smoking 1 | 103 (27.8%) | 78 (28.4%) | 25 (26.0%) | 0.662 |
| Immunosuppressive therapy | 11 (2.7%) | 6 (1.9%) | 5 (4.8%) | 0.156 |
| Previous endocarditis | 60 (14.5%) | 51 (16.6%) | 9 (8.6%) | 0.045 |
| LVEF poor (<30) | 41 (10.5%) | 35 (12.0%) | 6 (6.1%) | 0.096 |
| Coronary heart disease | 178 (43.2%) | 142 (46.3%) | 36 (34.3%) | 0.033 |
| Single-vessel disease | 76 (18.4%) | 56 (18.2%) | 20 (19.0%) | 0.854 |
| Two-vessel-disease | 36 (8.7%) | 29 (9.4%) | 7 (6.7%) | 0.384 |
| Three-vessel disease | 66 (16.0%) | 57 (18.6%) | 9 (8.6%) | 0.016 |
| Previous cardiac surgery | 171 (41.4%) | 125 (40.6%) | 46 (43.8%) | 0.562 |
| Previous CABG | 9 (2.2%) | 7 (2.3%) | 2 (1.9%) | 1.000 |
| Aortic valve replacement | 69 (16.7%) | 45 (14.6%) | 24 (22.9%) | 0.050 |
| Mitral valve replacement/ resection | 6 (1.5%) | 4 (1.3%) | 2 (1.9%) | 0.067 |
| Combined valve surgery | 79 (19.1%) | 63 (20.5%) | 16 (15.2%) | 0.241 |
| TAVI | 2 (0.5%) | 2 (0.6%) | 0 (0%) | 1.000 |
| Clinical presentation | ||||
| Acute myocardial infarction (≤48 h) | 14 (3.4%) | 11 (3.6%) | 3 (2.9%) | 1.000 |
| Cardiogenic shock | 21 (5.1%) | 18 (5.8%) | 3 (2.9%) | 0.229 |
| CPR (≤48 h) | 9 (2.2%) | 8 (2.6%) | 1 (1.0%) | 0.449 |
| Emergency | 90 (21.8%) | 72 (23.4%) | 18 (17.1%) | 0.181 |
| Transfer from intensive care unit | 109 (26.5%) | 80 (26.1%) | 29 (27.6%) | 0.754 |
| Intubated at admission | 38 (9.2%) | 29 (9.4%) | 9 (8.6%) | 0.796 |
| Neurological deficits (TIA or stroke) | 81 (19.6%) | 55 (17.9%) | 26 (24.8%) | 0.124 |
| Stroke | 76 (18.4%) | 53 (17.2%) | 23 (21.9%) | 0.283 |
| Preoperative embolization | 114 (27.6%) | 81 (26.3%) | 33 (31.4%) | 0.310 |
| Embolization of several organs | 28 (6.8%) | 17 (5.5%) | 11 (10.5%) | 0.081 |
| Fever (≥38 °C) | 270 (66.5%) | 206 (68.0%) | 64 (62.1%) | 0.277 |
| Fever until surgery | 63 (15.5%) | 48 (15.8%) | 15 (14.6%) | 0.757 |
| Time from diagnosis to surgery >7 days | 243 (59.3%) | 180 (58.8%) | 63 (60.6%) | 0.753 |
| Time from antibiotic start to surgery | ||||
| ≤1 day | 59 (14.5%) | 49 (16.1%) | 10 (9.6%) | 0.104 |
| 2–3 days | 38 (9.3%) | 23 (7.6%) | 15 (14.4%) | 0.038 |
| 4–7 days | 47 (11.5%) | 39 (12.8%) | 8 (7.7%) | 0.157 |
| >7 days | 264 (64.7%) | 193 (63.5%) | 71 (68.3%) | 0.378 |
| Pathogens | ||||
| Staphylococcus aureus | 82 (20.0%) | 59 (19.3%) | 23 (21.9%) | 0.562 |
| Enterococcus | 61 (14.8%) | 48 (15.7%) | 13 (12.4%) | 0.411 |
| Streptococcus viridans | 43 (10.5%) | 35 (11.4%) | 8 (7.6%) | 0.270 |
| Gram-positive streptococcus | 37 (9.0%) | 26 (8.5%) | 11 (10.5%) | 0.541 |
| HACEK group | 1 (0.2%) | 1 (0.3%) | 0 (0%) | 1.000 |
| Mycosis | 6 (1.5%) | 3 (1.0%) | 3 (2.9%) | 0.177 |
| Culture negative IE | 113 (27.5%) | 85 (27.8%) | 28 (26.7%) | 0.826 |
| Staphylococcus epidermidis | 28 (6.8%) | 18 (5.9%) | 10 (9.5%) | 0.201 |
| MRSA | 14 (3.4%) | 10 (3.3%) | 4 (3.8%) | 0.760 |
| Affected valves | ||||
| Aortic valve endocarditis | 168 (40.7%) | 137 (44.5%) | 31 (29.5%) | 0.007 |
| Isolated Aortic valve endocarditis | 128 (31.0%) | 107 (34.7%) | 21 (20.0%) | 0.005 |
| Mitral valve endocarditis | 129 (31.2%) | 90 (29.2%) | 39 (37.1%) | 0.130 |
| Isolated Mitral valve endocarditis | 92 (22.3%) | 61 (19.8%) | 31 (29.5%) | 0.039 |
| Tricuspid valve endocarditis | 16 (3.9%) | 8 (2.6%) | 8 (7.6%) | 0.036 |
| Isolated Tricuspid valve endocarditis | 7 (1.7%) | 4 (1.3%) | 3 (2.9%) | 0.377 |
| Isolated Prosthetic endocarditis | 143 (34.6%) | 104 (33.8%) | 39 (37.1%) | 0.530 |
| Paravalvular leak | 17 (4.1%) | 13 (4.2%) | 4 (3.8%) | 1.000 |
| Valve insufficiency (at least grade 2) | 359 (87.3%) | 267 (87.3%) | 92 (87.6%) | 0.923 |
| Aortic valve | 108 (26.3%) | 87 (28.4%) | 21 (20.0%) | 0.090 |
| Mitral valve | 78 (19.0%) | 55 (18.0%) | 23 (21.9%) | 0.375 |
| Tricuspid valve | 8 (1.9%) | 3 (1.0%) | 5 (4.8%) | 0.029 |
| Peri-annular abscess | 113 (27.8%) | 81 (26.6%) | 32 (31.1%) | 0.386 |
| Vegetation | 285 (70.4%) | 209 (69.2%) | 76 (73.8%) | 0.309 |
| Preoperative laboratory results | ||||
| C-reactive protein (mg/L) | 42.7 (16.4;90.5) | 43.5 (19.3;91.1) | 41.2 (13.6;88.2) | 0.565 |
| Variable | Overall (n = 413) | Men (n = 308, 74.6%) | Women (n = 105, 25.4%) | p-Value |
|---|---|---|---|---|
| Length of surgery (min) | 273 (220;355) | 274 (224;357) | 271 (216;337) | 0.411 |
| Cardiopulmonary bypass time (min) | 166 (125;215) | 166 (126;214) | 166 (121;219) | 0.879 |
| Cross-clamp time (min) | 116 (86;156) | 115 (86;157) | 116 (83;144) | 0.433 |
| Circulatory arrest (min) | 0 (0–36) | 0 (0–36) | 0 (0–32) | 0.520 |
| Number of packed red blood cells (unit) | 3 (0–27) | 2 (0–27) | 4 (0–14) | <0.001 |
| Number of fresh frozen plasma (unit) | 0 (0–13) | 0 (0–13) | 0 (0–12) | 0.900 |
| Number of platelet concentrate (unit) | 1 (0–6) | 1 (0–6) | 1 (0–4) | 0.143 |
| Aortic valve surgery | 305 (74.2%) | 239 (78.1%) | 66 (62.9%) | 0.002 |
| Mitral valve surgery | 155 (37.7%) | 110 (35.9%) | 45 (42.9%) | 0.207 |
| Tricuspid valve surgery | 15 (3.6%) | 8 (2.6%) | 7 (6.7%) | 0.070 |
| Thoracic aortic surgery | 55 (13.4%) | 43 (14.1%) | 12 (11.5%) | 0.509 |
| CABG | 49 (11.9%) | 37 (12.1%) | 12 (11.4%) | 0.856 |
| Variable | Overall (n = 413) | Men (n = 308, 74.6%) | Women (n = 105, 25.4%) | p-Value |
|---|---|---|---|---|
| AKI KDIGO stages | 115 (29.3%) | 85 (29.2%) | 30 (29.4%) | 0.969 |
| New–onset of hemodialysis | 61 (15.6%) | 46 (15.8%) | 15 (14.9%) | 0.819 |
| 24 h-drainage loss (mL) | 600 (300;1100) | 650 (388;1150) | 510 (250;1060) | 0.123 |
| Rethoracotomy (bleeding/tamponade) | 50 (12.4%) | 40 (13.3%) | 10 (9.7%) | 0.341 |
| Number of packed red blood cells (unit) 1 | 2 (0–27) | 2 (0–27) | 2 (0–17) | 0.015 |
| Number of fresh frozen plasma, (unit) 1 | 0 (0–35) | 0 (0–35) | 0 (0–32) | 0.269 |
| Number of platelet concentrate, (unit) 1 | 0 (0–9) | 0 (0–8) | 0 (0–9) | 0.357 |
| Ventilation time (h) | 16 (9;45) | 16 (9;44) | 16 (9;55) | 0.801 |
| Reintubation | 49 (12.3%) | 33 (11.1%) | 16 (15.7%) | 0.220 |
| Tracheotomy | 57 (14.5%) | 47 (16.2%) | 10 (9.9%) | 0.125 |
| ICU time (d) | 3 (1;7) | 3 (1;7) | 3 (1;6) | 0.245 |
| Postoperative days (d) | 10 (7;16) | 10 (7;17) | 9 (5;15) | 0.046 |
| Postoperative delirium | 64 (16.1%) | 54 (18.2%) | 10 (10.0%) | 0.054 |
| Stroke | 18 (4.5%) | 11 (3.7%) | 7 (6.9%) | 0.265 |
| CPR | 22 (5.5%) | 17 (5.7%) | 5 (4.9%) | 0.759 |
| Pacemaker patient | 47 (11.6%) | 37 (12.2%) | 10 (9.8%) | 0.511 |
| Postoperative myocardial infarction | 5 (1.3%) | 4 (1.3%) | 1 (1.0%) | 1.000 |
| Bronchopulmonary infection | 45 (11.1%) | 36 (11.8%) | 9 (8.9%) | 0.422 |
| Sepsis | 54 (13.3%) | 40 (13.1%) | 14 (13.9%) | 0.839 |
| Sternal wound infection 2 | 9 (2.5%) | 8 (2.9%) | 1 (1.1%) | 0.694 |
| Hospital mortality | 68 (16.6%) | 45 (14.7%) | 23 (22.3%) | 0.070 |
| Cardiac death | 10 (14.3%) | 6 (13.3%) | 4 (16.0%) | 0.737 |
| Cerebral death | 1 (1.4%) | 1 (2.2%) | 0 (0%) | 1.000 |
| Sepsis | 9 (12.9%) | 5 (11.1%) | 4 (16.0%) | 0.712 |
| MOF | 50 (71.4%) | 33 (73.3%) | 17 (68.0%) | 0.636 |
| 30 day mortality | 74 (17.9%) | 46 (14.9%) | 28 (26.7%) | 0.007 |
| Survival/follow-up time (years) | 3.9 (1.2;7.7) | 3.7 (1.1;7.8) | 4.6 (1.4;7.8) | 0.535 |
| Risk Factors Group | Odds Ratio Overall | 95% CI | p-Value | Odds Ratio Men | 95% CI | p-Value | Odds Ratio Women | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 1.036 | 1.010–1.063 | 0.006 | ||||||
| Age ≥ 65 years | 4.921 | 1.048–23.099 | 0.043 | ||||||
| Age ≥ 70 years | 2.836 | 1.265–6.357 | 0.011 | ||||||
| Female gender | 2.090 | 1.077–4.053 | 0.029 | ||||||
| Body mass index | 1.104 | 1.026–1.189 | 0.008 | ||||||
| PH | 3.500 | 1.440–8.508 | 0.006 | ||||||
| Dialysis | 5.943 | 2.019–17.494 | 0.001 | 6.974 | 1.133–42.922 | 0.036 | |||
| NYHA IV | 2.719 | 1.344–5.500 | 0.005 | 3.108 | 1.344–7.189 | 0.008 | |||
| Cardiogenic shock | 3.415 | 1.027–11.350 | 0.045 | 9.083 | 2.418–34.112 | 0.001 | |||
| Stroke | 2.664 | 1.281–5.543 | 0.009 | ||||||
| Transfer from ICU | 10.086 | 1.791–56.806 | 0.009 | ||||||
| AV insufficiency | 0.341 | 0.133–0.879 | 0.026 | ||||||
| Fever until surgery | 2.828 | 1.030–7.768 | 0.044 | ||||||
| Culture negative | 2.661 | 1.161–6.100 | 0.021 | ||||||
| Abscess | 2.513 | 1.332–4.742 | 0.004 | 2.570 | 1.075–6.142 | 0.034 | |||
| CRP (mg/L) | 1.008 | 1.003–1.012 | 0.001 | 1.012 | 1.002–1.022 | 0.021 | |||
| AV endocarditis | 0.041 | 0.004–0.432 | 0.007 | ||||||
| Embolization | 4.678 | 1.032–21.194 | 0.045 |
| Risk Factors Group | Hazard Ratio Overall | 95% CI | p-Value | Hazard Ratio Men | 95% CI | p-Value | Hazard Ratio Women | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Age ≥ 65 years | 2.198 | 1.385–3.488 | <0.001 | 1.921 * | 1.287–2.868 | 0.001 | 2.066 | 1.056–4.040 | 0.034 |
| Female gender | 1.097 | 0.662–1.820 | 0.718 | ||||||
| AHT | 1.685 | 1.076–2.637 | 0.022 | ||||||
| NYHA IV | 4.192 | 1.954–8.993 | <0.001 | ||||||
| Poor LVEF (<30%) | 1.945 | 1.000–3.783 | 0.050 | 2.166 | 1.342–3.497 | 0.002 | |||
| PAD | 2.515 | 1.291–4.900 | 0.007 | 1.795 | 1.023–3.152 | 0.041 | |||
| CAD stage 3 | 4.040 | 1.633–9.994 | 0.003 | ||||||
| Dialysis | 2.186 | 1.102–4.338 | 0.025 | 1.926 | 1.145–3.241 | 0.014 | 3.383 | 1.317–8.688 | 0.011 |
| Combined surgery | 2.223 | 1.236–3.998 | 0.008 | 1.709 | 1.054–2.770 | 0.030 | |||
| Cardiogenic shock | 3.601 | 1.803–7.189 | <0.001 | ||||||
| Emergency | 5.850 | 2.439–14.032 | <0.001 | ||||||
| Diagnosis > 7 days | 2.902 | 1.341–6.282 | 0.007 | ||||||
| Stroke | 2.165 | 1.334–3.516 | 0.002 | ||||||
| Tumor | 1.687 | 1.014–2.808 | 0.044 | ||||||
| Liver disease | 1.912 | 1.090–3.355 | 0.024 | 2.114 | 1.310–3.413 | 0.002 | |||
| S. viridans | 0.336 | 0.123–0.924 | 0.035 | ||||||
| S. epidermidis | 4.878 | 1.680–14.160 | 0.004 | ||||||
| AV endocarditis | 0.300 | 0.123–0.734 | 0.008 | ||||||
| Abscess | 1.561 | 1.038–2.348 | 0.032 | ||||||
| CRP (mg/L) | 1.006 | 1.001–1.010 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedrich, C.; Salem, M.; Puehler, T.; Panholzer, B.; Herbers, L.; Reimers, J.; Hummitzsch, L.; Cremer, J.; Haneya, A. Sex-Specific Risk Factors for Short- and Long-Term Outcomes after Surgery in Patients with Infective Endocarditis. J. Clin. Med. 2022, 11, 1875. https://doi.org/10.3390/jcm11071875
Friedrich C, Salem M, Puehler T, Panholzer B, Herbers L, Reimers J, Hummitzsch L, Cremer J, Haneya A. Sex-Specific Risk Factors for Short- and Long-Term Outcomes after Surgery in Patients with Infective Endocarditis. Journal of Clinical Medicine. 2022; 11(7):1875. https://doi.org/10.3390/jcm11071875
Chicago/Turabian StyleFriedrich, Christine, Mohamed Salem, Thomas Puehler, Bernd Panholzer, Lea Herbers, Julia Reimers, Lars Hummitzsch, Jochen Cremer, and Assad Haneya. 2022. "Sex-Specific Risk Factors for Short- and Long-Term Outcomes after Surgery in Patients with Infective Endocarditis" Journal of Clinical Medicine 11, no. 7: 1875. https://doi.org/10.3390/jcm11071875