
RETRACTED: Validation of the CHA2DS2-VA Score (Excluding Female Sex) in Nonvalvular Atrial Fibrillation Patients: A Nationwide Population-Based Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Risk Stratification Schemes for Ischemic Stroke
2.3. Clinical Endpoint
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
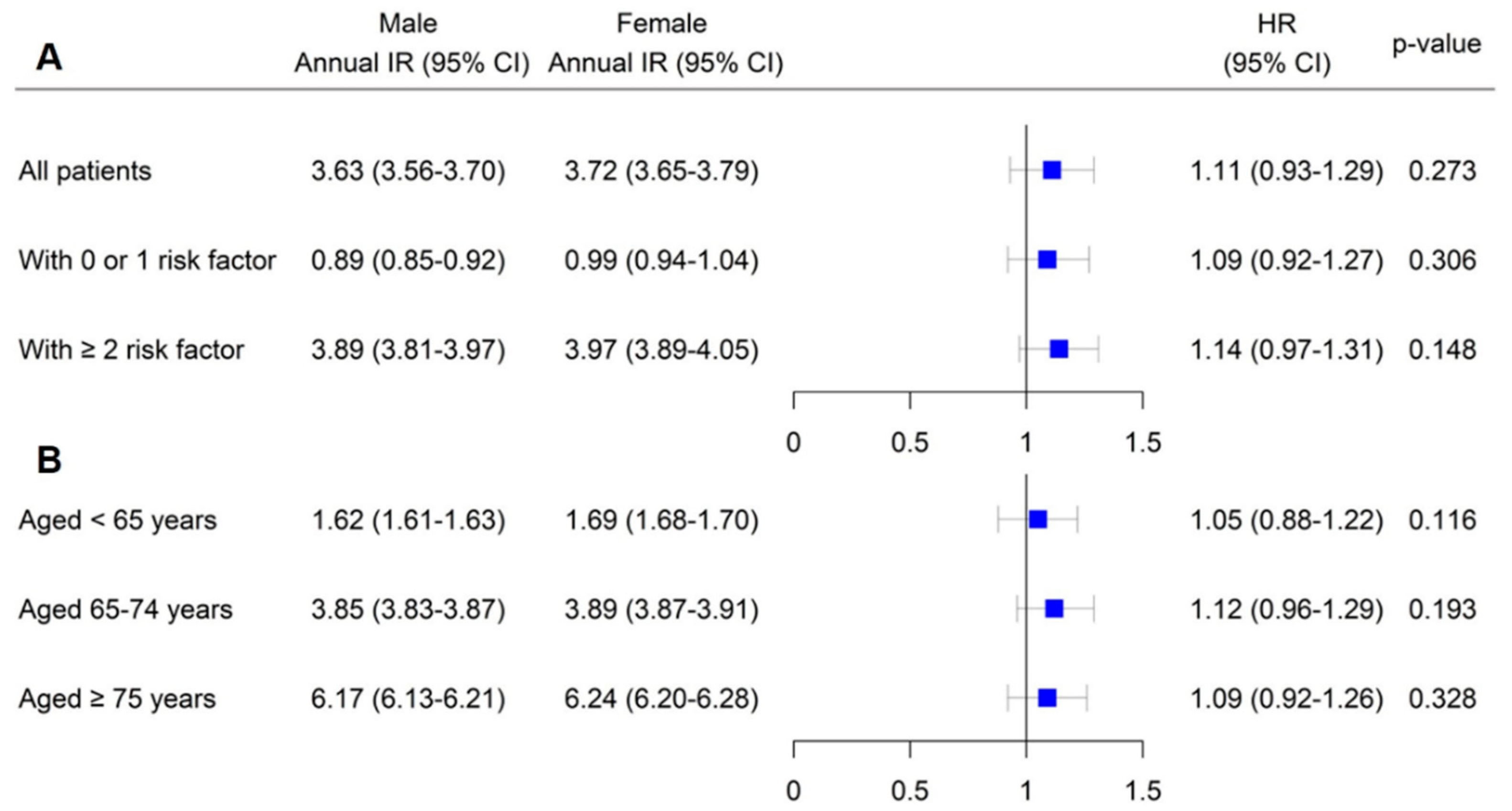
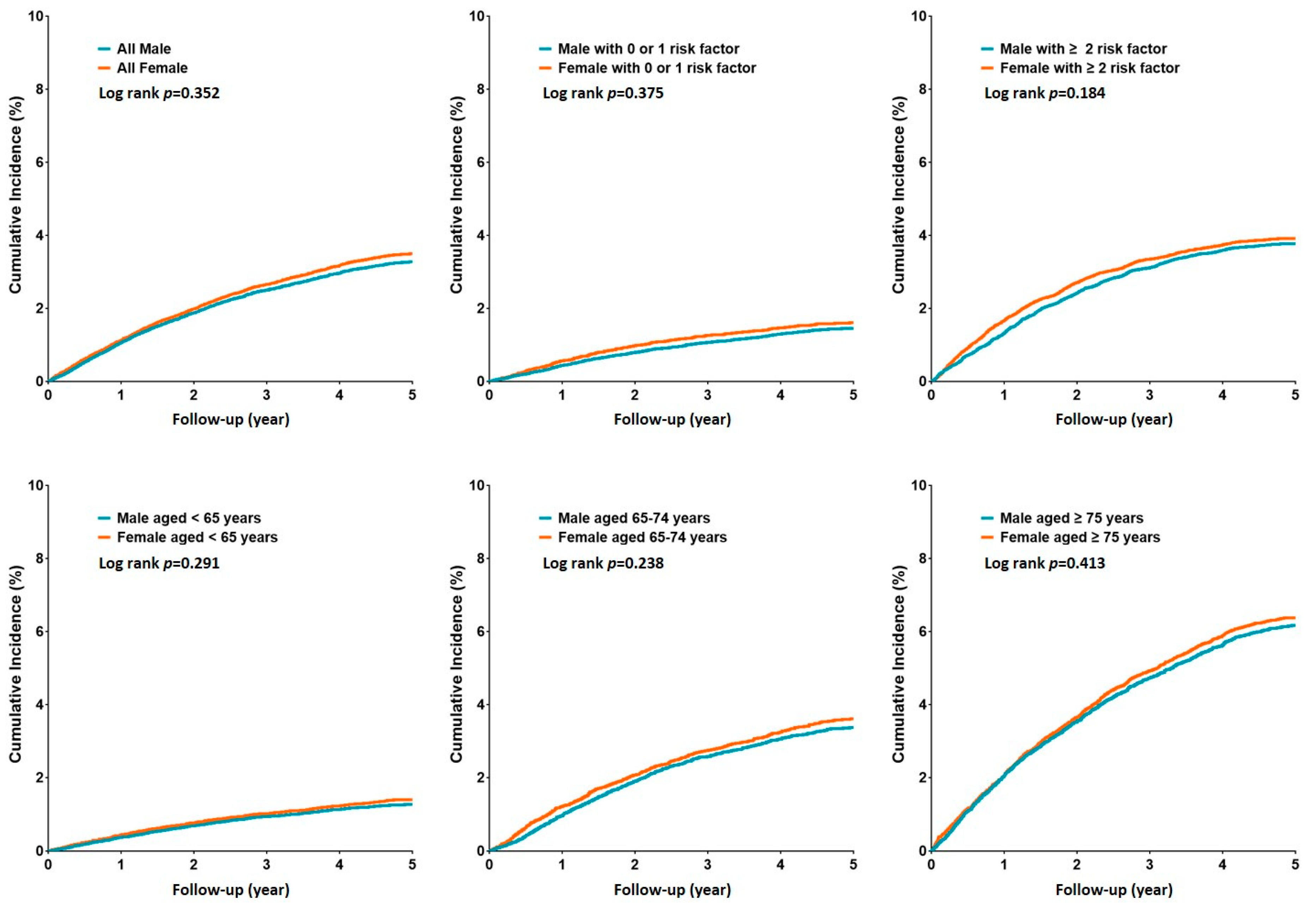
3.2. Risk of Ischemic Stroke in Male and Female Patients Stratified by Risk Score Components and Age
3.3. Risk of Ischemic Stroke in AF Patients Stratified by Risk Scores
3.4. Comparison of Risk Scores
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. ESC scientific document group. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.E.; Okumura, K.; Zhang, S.; Chao, T.F.; Siu, C.W.; Wei Lim, T.; Saxena, A.; Takahashi, Y.; Siong Teo, W. Consensus of the Asia Pacific heart rhythm society on stroke prevention in atrial fibrillation. J. Arrhythm. 2017, 33, 345–367. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patientswith atrialfibrillation. J. Am. Coll. Cardiol. 2019, 74, 104–132. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The Euro Heart Survey on Atrial Fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Humphries, K.H.; Kerr, C.R.; Connolly, S.J.; Klein, G.; Boone, J.A.; Green, M.; Sheldon, R.; Talajic, M.; Dorian, P.; Newman, D. New-onset atrial fibrillation: Sex differences in presentation, treatment, and outcome. Circulation 2001, 103, 2365–2370. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch. Intern. Med. 1994, 154, 1449–1457. [Google Scholar] [CrossRef]
- Tsadok, M.A.; Jackevicius, C.A.; Rahme, E.; Humphries, K.H.; Behlouli, H.; Pilote, L. Sex differences in stroke risk among older patients with recently diagnosed atrial fibrillation. JAMA 2012, 307, 1952–1958. [Google Scholar]
- Friberg, L.; Benson, L.; Rosenqvist, M.; Lip, G.Y. Assessment of female sex as a risk factor in atrial fibrillation in Sweden: Nationwide retrospective cohort study. BMJ 2012, 344, e3522. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, A.P.; Lindhardsen, J.; Lip, G.; Gislason, G.H.; Torp-Pedersen, C.; Olesen, J.B. Female sex as a risk factor for stroke in atrial fibrillation: A nationwide cohort study. J. Thromb. Haemost. 2012, 10, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.J.; Overvad, T.; Lip, G.Y.; Lane, D.A. Is female sex a risk factor for stroke and thromboembolism in patients with atrial fibrillation? A systematic review and meta-analysis. QJM 2014, 107, 955–967. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.Y.; Lee, C.H.; Yu, C.C.; Tsai, C.T.; Lai, L.P.; Hwang, J.J.; Chen, P.C.; Lin, J.L. Risk factors and incidence of ischemic stroke in Taiwanese with nonvalvular atrial fibrillation: A nationwide database analysis. Atherosclerosis 2011, 217, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Apostolakis, S.; Blann, A.D.; Wang, H.; Zhao, X.; Zhang, Y.; Zhang, D.; Ma, J.; Wang, Y.; Lip, G.Y. Validation of contemporary stroke and bleeding risk stratification scores in non-anticoagulated Chinese patients with atrial fibrillation. Int. J. Cardiol. 2013, 168, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Siu, C.W.; Lip, G.Y.; Lam, K.F.; Tse, H.F. Risk of stroke and intracranial hemorrhage in 9727 Chinese with atrial fibrillation in Hong Kong. Heart Rhythm. 2014, 11, 1401–1408. [Google Scholar] [CrossRef]
- Inoue, H.; Atarashi, H.; Okumura, K.; Yamashita, T.; Origasa, H.; Kumagai, N.; Sakurai, M.; Kawamura, Y.; Kubota, I.; Matsumoto, K.; et al. Impact of gender on the prognosis of patients with nonvalvular atrial fibrillation. Am. J. Cardiol. 2014, 113, 957–962. [Google Scholar] [CrossRef]
- Overvad, T.F.; Rasmussen, L.H.; Skjoth, F.; Overvad, K.; Albertsen, I.E.; Lane, D.A.; Lip, G.Y.; Larsen, T.B. Female sex as a risk factor for thromboembolism and death in patients with incident atrial fibrillation: The prospective Danish Diet, Cancer and Health study. Thromb. Haemost. 2014, 112, 789–795. [Google Scholar]
- Tomita, H.; Okumura, K.; Inoue, H.; Atarashi, H.; Yamashita, T.; Origasa, H.; Tsushima, E.; J-RHYTHM Registry Investigators. Validation of risk scoring system excluding female sex from CHA2DS2-VASc in Japanese patients with nonvalvular atrial fibrillation—Subanalysis of the J-RHYTHM Registry. Circ. J. 2015, 79, 1719–1726. [Google Scholar] [CrossRef]
- Nielsen, P.B.; Skjøth, F.; Overvad, T.F.; Larsen, T.B.; Lip, G.Y.H. Female sex is a risk modifier rather than a risk factor for stroke in atrial fibrillation: Should we use a CHA2DS2-VA score rather than CHA2DS2-VASc? Circulation 2018, 137, 832–840. [Google Scholar] [CrossRef]
- Nielsen, P.B.; Overvad, T.F. Female sex as a risk modifier for stroke risk in atrial fibrillation: Using CHA2DS2-VASc versus CHA2DS2-VA for stroke risk stratification in atrial fibrillation: A note of caution. Thromb. Haemost. 2020, 120, 894–898. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Cairns, J.; Mitchell, L.B.; Macle, L.; Stiell, I.G.; Gladstone, D.; McMurtry, M.S.; Connolly, S.; Cox, J.L.; Dorian, P.; et al. 2014 focused update of the Canadian cardiovascular society guidelines for the management of atrial fibrillation. Can. J. Cardiol. 2014, 30, 1114–1130. [Google Scholar] [CrossRef] [PubMed]
- Brieger, D.; Amerena, J.; Attia, J.; Bajorek, B.; Chan, K.H.; Connell, C.; Freedman, B.; Ferguson, C.; Hall, T.; Haqqani, H.M.; et al. National Heart foundation of Australia and the cardiac society of Australia and New Zealand: Australian clinical guidelines for the diagnosis and management of atrial fibrillation 2018. Heart Lung. Circ. 2018, 27, 1209–1266. [Google Scholar] [CrossRef] [PubMed]
- JCS Joint Working Group. Guidelines for pharmacotherapy of atrial fibrillation (JCS 2013): Digest version. Circ. J. 2014, 78, 1997–2021. [Google Scholar] [CrossRef]
- Proietti, M.; Mujovic, N.; Potpara, T.S. Optimizing stroke and bleeding risk assessment in patients with atrial fibrillation: A balance of evidence, practicality and precision. Thromb. Haemost. 2018, 118, 2014–2017. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factor | CHA2DS2-VASc Score | CHA2DS2-VA Score |
|---|---|---|
| Congestive heart failure/LV dysfunction | 1 | 1 |
| Hypertension | 1 | 1 |
| Age ≥75 | 2 | 2 |
| Diabetes mellitus | 1 | 1 |
| Stroke/TIA/thromboembolism | 2 | 2 |
| Vascular disease | 1 | 1 |
| Age 65–74 | 1 | 1 |
| Sex category (i.e., female sex) | 1 | 0 |
| Variables | Total (Total = 185,637) | Male Patients (n = 93,395) | Female Patients (n = 92,242) |
|---|---|---|---|
| Age, years | 65.7 ± 12.3 | 64.9 ± 11.5 | 66.5 ± 12.1 |
| <55 years, n (%) | 38,639 (20.8) | 21,574 (23.1) | 17,065 (18.5) |
| 55–64 years, n (%) | 41,327 (22.3) | 22,602 (24.2) | 18,725 (20.3) |
| 65–74 years, n (%) | 52,320 (28.2) | 23,909 (25.6) | 28,411 (30.8) |
| ≥75 years, n (%) | 53,352 (28.7) | 25,310 (27.1) | 28,042 (30.4) |
| Clinical history, n (%) | |||
| Hypertension | 121,580 (65.5) | 60,146 (64.4) | 61,433 (66.6) |
| Diabetes mellitus | 41,200 (22.2) | 19,800 (21.2) | 21,400 (23.2) |
| Heart failure | 60,232 (32.4) | 29,700 (31.8) | 30,532 (33.1) |
| Dyslipidemia | 67,306 (36.3) | 34,836 (37.3) | 32,469 (35.2) |
| Vascular disease | 44,441 (23.9) | 20,827 (22.3) | 23,614 (25.6) |
| Prior myocardial infarction | 7981 (4.3) | 3923 (4.2) | 4059 (4.4) |
| Prior peripheral artery disease | 36,738 (19.8) | 16,998 (18.2) | 19,740 (21.4) |
| CHA2DS2-VASc score | |||
| Score = 0 | 8996 (4.8) | 8996 (9.6) | 0 (0.0) |
| Score = 1 | 26,757 (14.4) | 21,312 (22.8) | 5445 (5.9) |
| Score = 2 | 43,344 (23.3) | 29,955 (32.1) | 13,389 (14.5) |
| Score ≥ 3 | 106,540 (57.4) | 33,132 (35.5) | 73,408 (79.6) |
| CHA2DS2-VA score | |||
| Score = 0 | 14,441 (7.8) | 8996 (9.6) | 5445 (5.9) |
| Score = 1 | 34,701 (18.7) | 21,312 (22.8) | 13,389 (14.5) |
| Score = 2 | 57,093 (30.8) | 29,955 (32.1) | 27,138 (29.4) |
| Score ≥ 3 | 79,402 (42.8) | 33,132 (35.5) | 46,270 (50.2) |
| Medication | |||
| No therapy | 17,207 (9.3) | 8395 (9.0) | 8812 (9.6) |
| Aspirin | 42,163 (22.7) | 20,386 (21.8) | 21,777 (23.6) |
| Warfarin | 61,128 (32.9) | 29,981 (32.1) | 31,147 (33.8) |
| NOAC | 65,139 (35.1) | 34,633 (37.1) | 30,506 (33.1) |
| Rivaroxaban | 27,970 (15.1) | 14,599 (15.6) | 13,371 (14.5) |
| Dabigatran | 16,837 (9.1) | 9285 (9.9) | 7552 (8.2) |
| Apixaban | 15,608 (8.4) | 8574 (9.2) | 7034 (7.6) |
| Edoxaban | 4724 (2.5) | 2175 (2.3) | 2549 (2.8) |
| Follow up, years (IQR) | 2.1 (1.4–2.6) | 2.0 (1.1–2.7) | 2.2 (1.2–2.6) |
| No. of Events | IR (95% CI) | p-Value | HR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| CHA2DS2-VASc of 0 | 157/8996 | 0.65 (0.60–0.70) | 0.498 | Reference | 0.498 |
| CHA2DS2-VA of 0 | 260/14,441 | 0.72 (0.68–0.76) | 1.12 (0.95–1.29) | ||
| CHA2DS2-VASc of 1 | 517/26,757 | 1.01 (0.97–1.05) | 0.483 | Reference | 0.414 |
| CHA2DS2-VA of 1 | 690/34,701 | 1.09 (1.06–1.12) | 1.16 (0.99–1.33) | ||
| CHA2DS2-VASc of 2 | 1501/43,344 | 2.12 (2.07–2.17) | 0.004 | Reference | < 0.001 |
| CHA2DS2-VA of 2 | 1619/57,093 | 2.44 (2.39–2.49) | 1.33 (1.17–1.49) | ||
| CHA2DS2-VASc of ≥3 | 4076/106,540 | 5.18 (5.10–5.26) | <0.001 | Reference | < 0.001 |
| CHA2DS2-VA of ≥3 | 3682/79,402 | 5.46 (5.41–5.51) | 1.49 (1.34–1.64) |
| All Patients | C-Statistic | SE | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| CHA2DS2-VA score | 0.671 | 0.005 | 0.663–0.679 | <0.001 | ||
| CHA2DS2-VASc score | 0.668 | 0.004 | 0.661–0.675 | <0.001 | ||
| Score difference | C-Statistic Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.003 (0.000–0.003) | 0.998 | 0.318 | 0.031 | 0.002–0.037 | 0.118 | |
| Risk score of 0 or 1 | C-Statistic | SE | 95% CI | p-Value | ||
| CHA2DS2-VA score | 0.628 | 0.005 | 0.619–0.637 | <0.001 | ||
| CHA2DS2-VASc score | 0.626 | 0.005 | 0.618–0.634 | <0.001 | ||
| Score difference | C-Statistic Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.002 (0.000–0.004) | 1.099 | 0.272 | 0.019 | 0.001–0.032 | 0.321 | |
| Risk score of≥2 | C-Statistic | SE | 95% CI | p-Value | ||
| CHA2DS2-VA score | 0.701 | 0.003 | 0.692–0.713 | <0.001 | ||
| CHA2DS2-VASc score | 0.689 | 0.003 | 0.675–0.703 | <0.001 | ||
| Score difference | C-Statistic Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.012 (0.009–0.021) | 4.596 | < 0.001 | 0.126 | 0.081–0.172 | 0.005 | |
| Aged < 65 years | C-Statistic | SE | 95% CI | p-Value | ||
| CHA2DS2-VA score | 0.642 | 0.006 | 0.630–0.654 | <0.001 | ||
| CHA2DS2-VASc score | 0.639 | 0.005 | 0.629–0.649 | <0.001 | ||
| Score difference | C-Statistic Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.003 (0.002–0.006) | 0.879 | 0.379 | 0.021 | 0.009–0.042 | 0.309 | |
| Aged 65–74 years | C-Statistic | SE | 95% CI | p-Value | ||
| CHA2DS2-VA score | 0.668 | 0.005 | 0.658–0.678 | <0.001 | ||
| CHA2DS2-VASc score | 0.663 | 0.004 | 0.655–0.671 | <0.001 | ||
| Score difference | C-Statistic Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.005 (0.003–0.008) | 1.193 | 0.233 | 0.034 | 0.016–0.059 | 0.227 | |
| Aged ≥ 75 years | C-Statistic | SE | 95% CI | p-Value | ||
| CHA2DS2-VA score | 0.715 | 0.004 | 0.707–0.723 | <0.001 | ||
| CHA2DS2-VASc score | 0.701 | 0.005 | 0.691–0.711 | <0.001 | ||
| Score difference | C-Statistis Analysis | NRI Analysis | ||||
| C-Statistic Difference | Z | p-Value | NRI | 95% CI | p-Value | |
| 0.014 (0.011–0.022) | 4.957 | <0.001 | 0.159 | 0.119–0.196 | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.Y.; Kim, M.H.; Kim, H.B.; Kang, S.Y.; Lee, K.M.; Hyun, K.-Y.; Yun, S.-C. RETRACTED: Validation of the CHA2DS2-VA Score (Excluding Female Sex) in Nonvalvular Atrial Fibrillation Patients: A Nationwide Population-Based Study. J. Clin. Med. 2022, 11, 1823. https://doi.org/10.3390/jcm11071823
Choi SY, Kim MH, Kim HB, Kang SY, Lee KM, Hyun K-Y, Yun S-C. RETRACTED: Validation of the CHA2DS2-VA Score (Excluding Female Sex) in Nonvalvular Atrial Fibrillation Patients: A Nationwide Population-Based Study. Journal of Clinical Medicine. 2022; 11(7):1823. https://doi.org/10.3390/jcm11071823
Chicago/Turabian StyleChoi, Sun Young, Moo Hyun Kim, Hyo Bin Kim, Sa Yul Kang, Kwang Min Lee, Kyung-Yae Hyun, and Sung-Cheol Yun. 2022. "RETRACTED: Validation of the CHA2DS2-VA Score (Excluding Female Sex) in Nonvalvular Atrial Fibrillation Patients: A Nationwide Population-Based Study" Journal of Clinical Medicine 11, no. 7: 1823. https://doi.org/10.3390/jcm11071823