
Adherence to Medication in Older Adults with Type 2 Diabetes Living in Lubuskie Voivodeship in Poland: Association with Frailty Syndrome




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
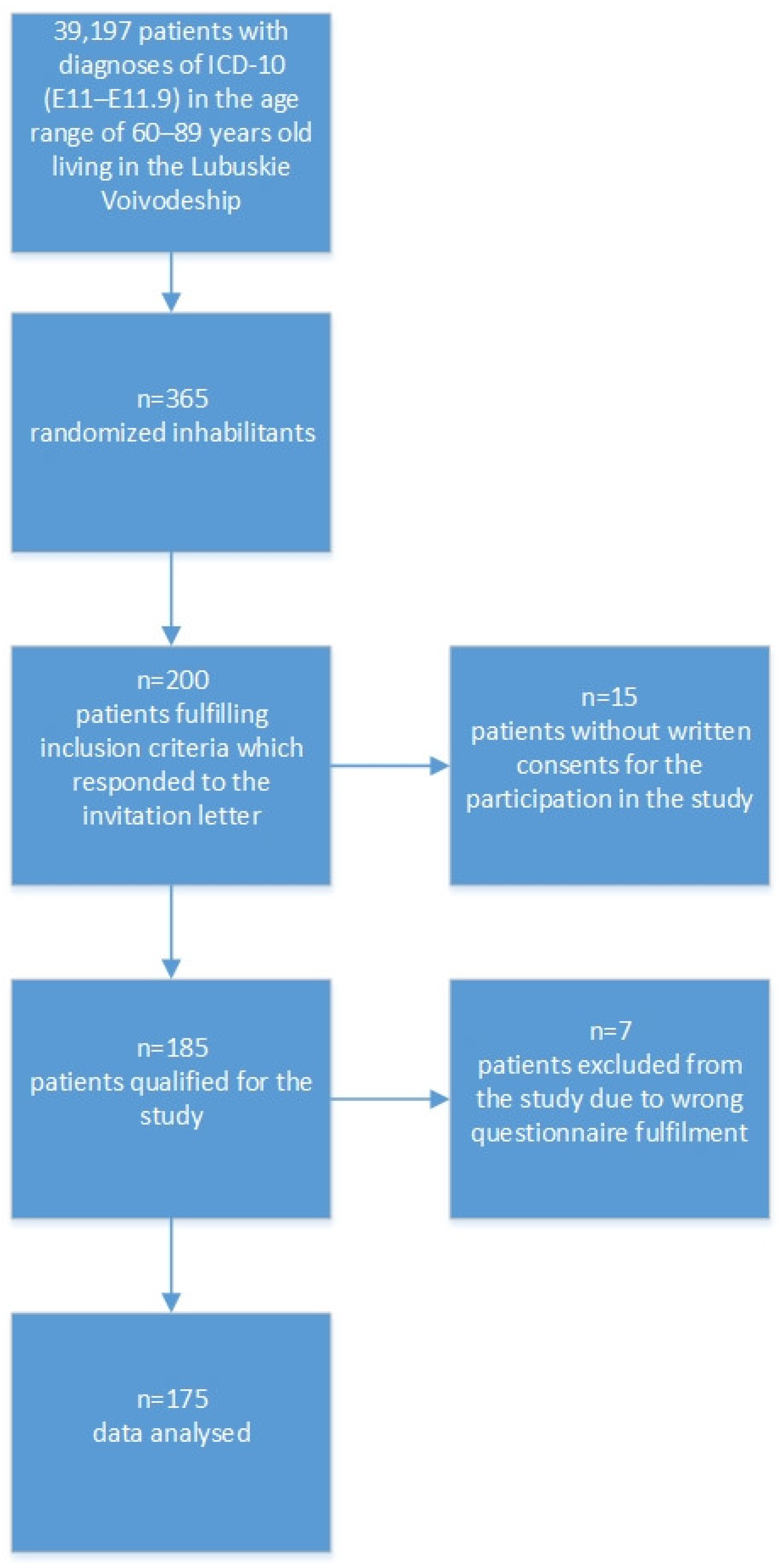
2.2. Participants
2.3. Research Tools
2.4. Statistical Analysis
3. Results
3.1. Descriptive Data
3.2. The Prevalence of Frailty Syndrome and Level of Adherence to Medication in Type 2 Diabetes Elderly Patients
3.3. Socio-Demographic and Clinical Variables in Adherent and Non-Adherent Groups
3.4. Frailty Syndrome vs. Adherence to Therapeutic Recommendations
3.5. Non-Adherence Predictors vs. Multifactorial Regression Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogura, S.; Jakovljevic, M.M. Editorial: Global Population Aging—Health Care, Social and Economic Consequences. Front. Public Health 2018, 6, 335. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.; Saeedi, P.; Kaundal, A.; Karuranga, S.; Malanda, B.; Williams, R. Diabetes and global ageing among 65–99-year-old adults: Findings from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, R.; Jialal, I. Diabetes Mellitus Type 2; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513253/ (accessed on 16 March 2022).
- Kao, C.C.; Hsieh, H.M.; Lee, D.Y.; Hsieh, K.P.; Sheu, S.J. Importance of medication adherence in treatment needed diabetic retinopathy. Sci. Rep. 2021, 11, 19100. [Google Scholar] [CrossRef] [PubMed]
- Bello-Chavolla, O.Y.; Rojas-Martinez, R.; Aguilar-Salinas, C.A.; Hernández-Avila, M. Epidemiology of diabetes mellitus in Mexico. Nutr. Rev. 2017, 75, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J.; Kim, K.I. Frailty and Disability in Diabetes. Ann. Geriatr. Med. Res. 2019, 23, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bujnowska-Fedak, M.M.; Gwyther, H.; Szwamel, K.; D’Avanzo, B.; Holland, C.; Shaw, R.L.; Kurpas, D. A qualitative study examining everyday frailty management strategies adopted by Polish stakeholders. Eur. J. Gen. Pract. 2019, 25, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Galluzzo, L.; Rodríguez-Laso, Á.; Van der Heyden, J.; Ranhoff, A.H.; Lamprini-Koula, M.; Ciutan, M.; López-Samaniego, L.; Carcaillon-Bentata, L.; Kennelly, S.; et al. Prevalence of frailty at population level in European ADVANTAGE Joint Action Member States: A systematic review and meta-analysis. Ann. Dell’istituto Super. Di Sanita 2018, 54, 226–238. [Google Scholar]
- Chhetri, J.K.; Zheng, Z.; Xu, X.; Ma, C.; Chan, P. The prevalence and incidence of frailty in Pre-diabetic and diabetic community-dwelling older population: Results from Beijing longitudinal study of aging II (BLSA-II). BMC Geriatr. 2017, 17, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKenzie, H.T.; Tugwell, B.; Rockwood, K.; Theou, O. Frailty and Diabetes in Older Hospitalized Adults: The Case for Routine Frailty Assessment. Can. J. Diabetes 2020, 44, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.; Wang, J.; Chien, K.L.; COhort of GEriatric Nephrology in NTUH (COGENT) Study Group. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 130. [Google Scholar] [CrossRef]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox. Biol. 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Ida, S.; Kaneko, R.; Imataka, K.; Murata, K. Relationship between frailty and mortality, hospitalization, and cardiovascular diseases in diabetes: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2019, 18, 81. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Woodhouse, L.; Rodríguez-Mañas, L.; Fried, L.P.; Woo, J.; Aprahamian, I.; Sanford, A.; Lundy, J.; et al. Physical Frailty: ICFSR International Clinical Practice Guidelines for Identification and Management. Nutr. Health Aging 2019, 23, 771–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, P.O.; Michel, J.P.; Zekry, D. Frailty syndrome: A transitional state in a dynamic process. Gerontology 2009, 55, 539–549. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Available online: https://www.who.int/chp/knowledge/publications/adherence_full_report.pdf?ua=1 (accessed on 19 January 2021).
- Fernandez-Lazaro, C.I.; García-González, J.M.; Adams, D.P.; Fernandez-Lazaro, D.; Mielgo-Ayuso, J.; Caballero-Garcia, A.; Racionero, F.M.; Córdova, A.; Miron-Canelo, J.A. Adherence to treatment and related factors among patients with chronic conditions in primary care: A cross-sectional study. BMC Fam. Pract. 2019, 20, 132. [Google Scholar] [CrossRef]
- Mendes, R.; Martins, S.; Fernandes, L. Adherence to Medication, Physical Activity and Diet in Older Adults With Diabetes: Its Association With Cognition, Anxiety and Depression. J. Clin. Med. Res. 2019, 11, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminde, L.N.; Tindong, M.; Ngwasiri, C.A.; Aminde, J.A.; Njim, T.; Fondong, A.A.; Takah, N.F. Adherence to antidiabetic medication and factors associated with non-adherence among patients with type-2 diabetes mellitus in two regional hospitals in Cameroon. BMC Endocr. Disord. 2019, 19, 35. [Google Scholar] [CrossRef] [Green Version]
- Hatah, E.; Rahim, N.; Makmor-Bakry, M.; Mohamed Shah, N.; Mohamad, N.; Ahmad, M.; Haron, N.H.; Hwe, C.S.; Wah, A.T.M.; Hassan, F.; et al. Adherence Development and validation of Malaysia Medication Assessment Tool (MyMAAT) for diabetic patients. PLoS ONE 2020, 15, e0241909. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition Management in Older Adults with Diabetes: A Review on the Importance of Shifting Prevention Strategies from Metabolic Syndrome to Frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Pobrotyn, P.; Pasieczna, A.; Diakowska, D.; Uchmanowicz, B.; Mazur, G.; Banasik, M.; Kołtuniuk, A. Evaluation of Frailty Syndrome and Adherence to Recommendations in Elderly Patients with Hypertension. J. Clin. Med. 2021, 10, 3771. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Nessler, J.; Gobbens, R.; Gackowski, A.; Kurpas, D.; Straburzyńska-Migaj, E.; Kałuzna-Oleksy, M.; Jankowska, E.A. Coexisting Frailty with Heart Failure. Front. Physiol. 2019, 10, 791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bąk, E.; Młynarska, A.; Marcisz, C.; Bobiński, R.; Sternal, D.; Młynarski, R. The influence of frailty syndrome on quality of life in elderly patients with type 2 diabetes. Qual. Life Res. 2021, 30, 2487–2495. [Google Scholar] [CrossRef] [PubMed]
- de Lima, B.F.; Gama, A.G.D.; da Nóbrega Dias, V.; da Silva, E.M.T.; da Costa Cavalcanti, F.A.; Gazzola, J.M. The frailty syndrome in older adults with type 2 diabetes mellitus and associated factors. Rev. Bras. De Geriatr. E Gerontol. 2020, 23, e190196. [Google Scholar] [CrossRef]
- Mone, P.; Gambardella, J.; Lombardi, A.; Pansini, A.; De Gennaro, S.; Leo, A.L.; Famiglietti, M.; Marro, A.; Morgante, M.; Frullone, S.; et al. Correlation of physical and cognitive impairment in diabetic and hypertensive frail older adults. Cardiovasc. Diabetol. 2022, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Thein, F.S.; Li, Y.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Physical frailty and cognitive impairment is associated with diabetes and adversely impact functional status and mortality. Postgrad. Med. 2018, 130, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Casals, C.; Casals Sánchez, J.L.; Suárez Cadenas, E.; Aguilar-Trujillo, M.P.; Estébanez Carvajal, F.M.; Vázquez-Sánchez, M.Á. Fragilidad en el adulto mayor con diabetes mellitus tipo 2 y su relación con el control glucémico, perfil lipídico, tensión arterial, equilibrio, grado de discapacidad y estado nutricional [Frailty in older adults with type 2 diabetes mellitus and its relation with glucemic control, lipid profile, blood pressure, balance, disability grade and nutritional status]. Nutr. Hosp. 2018, 35, 820–826. [Google Scholar] [PubMed]
- Dalon, F.; Van Ganse, E.; Correia Da Silva, C.; Nachbaur, G.; Saïl, L.; Belhassen, M. Revue générale sur l’adhésion aux traitements inhalés de la BPCO [Therapeutic adherence in chronic obstructive pulmonary disease: A literature review]. Rev. Mal. Respir. 2019, 36, 801–849. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Valiee, S.; Tahan, M.; Ebtekar, F.; Ghanei Gheshlagh, R. Barriers of medication adherence in patients with type-2 diabetes: A pilot qualitative study. Diabetes Metab. Syndr. Obes. 2019, 1, 589–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshehri, K.A.; Altuwaylie, T.M.; Alqhtani, A.; Albawab, A.A.; Almalki, A.H. Type 2 Diabetic Patients Adherence Towards Their Medications. Cureus 2020, 12, e6932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Świątoniowska-Lonc, N.; Tański, W.; Polański, J.; Jankowska-Polańska, B.; Mazur, G. Psychosocial Determinants of Treatment Adherence in Patients with Type 2 Diabetes—A Review. Diabetes Metab. Syndr. Obes. 2021, 16, 2701–2715. [Google Scholar] [CrossRef] [PubMed]
- Kefale, B.; Tadesse, Y.; Alebachew, M.; Engidawork, E. Management Practice, and Adherence and Its Contributing Factors among Patients with Chronic Kidney Disease at Tikur Anbessa Specialized Hospital: A Hospital Based Cross-Sectional Study. Int. J. Nephrol. 2018, 29, 2903139. [Google Scholar]
- Algabbani, F.M.; Algabbani, A.M. Treatment adherence among patients with hypertension: Findings from a cross-sectional study. Clin. Hypertens. 2020, 26, 18. [Google Scholar] [CrossRef] [PubMed]
- Mekonen, K.K.; Yismaw, M.B.; Abiye, A.A.; Tadesse, T.A. Adherence to Benzathine Penicillin G Secondary Prophylaxis and Its Determinants in Patients with Rheumatic Heart Disease at a Cardiac Center of an Ethiopian Tertiary Care Teaching Hospital. Patient Prefer. Adherence 2020, 14, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enricho Nkhoma, D.; Jenya Soko, C.; Joseph Banda, K.; Greenfield, D.; Li, Y.J.; Iqbal, U. Impact of DSMES app interventions on medication adherence in type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ Health Care Inform. 2021, 28, e100291. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.P.; Cheng, K.K.F.; Siah, R.C. A systematic review and meta-analysis on the effectiveness of education on medication adherence for patients with hypertension, hyperlipidaemia and diabetes. J. Adv. Nurs. 2019, 75, 2478–2494. [Google Scholar] [CrossRef] [PubMed]
- Wleklik, M.; Denfeld, Q.; Lisiak, M.; Czapla, M.; Kałużna-Oleksy, M.; Uchmanowicz, I. Frailty Syndrome in Older Adults with Cardiovascular Diseases-What Do We Know and What Requires Further Research? Int. J. Environ. Res. Public Health 2022, 19, 2234. [Google Scholar] [CrossRef] [PubMed]
- WSOZ-II.0123.28.2018; NFZ-Załącznik nr 1 Do Pisma Znak. National Health Fund: Warszawa, Poland, 2018.
- Kubica, A.; Kosobucka, A.; Michalski, P.; Pietrzykowski, Ł.; Jurek, A.; Wawrzyniak, M.; Kasprzak, Ł. Skala adherence w chorobach przewlekłych—nowe narzędzie do badania realizacji planu terapeutycznego. Folia Cardiol. 2017, 12, 19. [Google Scholar]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. The Tilburg Frailty Indicator: Psychometric properties. J. Am. Med. Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Jankowska-Polańska, B.; Uchmanowicz, B.; Kowalczuk, K.; Gobbens, R.J. Validity and Reliability of the Polish Version of the Tilburg Frailty Indicator (TFI). J. Frailty Aging 2016, 5, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Santiago, L.M. The Tilburg Frailty Indicator (TFI): New Evidence for Its Validity. Clin. Interv. Aging 2020, 15, 265–274. [Google Scholar]
- Uchmanowicz, I.; Jankowska-Polańska, B.; Łoboz-Rudnicka, M.; Manulik, S.; Łoboz-Grudzień, K.; Gobbens, R.J. Cross-cultural adaptation and reliability testing of the Tilburg Frailty Indicator for optimizing care of Polish patients with frailty syndrome. Clin. Interv. Aging 2014, 25, 997–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, G.A.; Gray, D.S. Obesity. Part I—Pathogenesis. West. J. Med. 1988, 149, 429–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Lifestyle Management: Standards of Medical Care in Diabetes. Diabetes Care 2018, 41, 38–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, L.N.; Lyu, Q.; Yao, H.Y.; Yang, L.; Chen, S.Z. The prevalence of frailty among community-dwelling older adults with diabetes: A meta-analysis. Int. J. Nurs. Stud. 2021, 119, 103952. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, G.; Midão, L.; Paúl, C.; Cena, C.; Duarte, M.; Costa, E. Prevalence of frailty status among the European elderly population: Findings from the Survey of Health, Aging and Retirement in Europe. Geriatr. Gerontol. Int. 2019, 19, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Cobo, A.; Vázquez, L.A.; Reviriego, J.; Rodríguez-Mañas, L. Impact of frailty in older patients with diabetes mellitus: An overview. Endocrinol. Nutr. 2016, 63, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Saum, K.U.; Dieffenbach, A.K.; Müller, H.; Holleczek, B.; Hauer, K.; Brenner, H. Frailty prevalence and 10-year survival in community-dwelling older adults: Results from the ESTHER cohort study. Eur. J. Epidemiol. 2014, 29, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Ferri-Guerra, J.; Aparicio-Ugarriza, R.; Salguero, D.; Baskaran, D.; Mohammed, Y.N.; Florez, H.; Ruiz, J.G. The Association of Frailty with Hospitalizations and Mortality among Community Dwelling Older Adults with Diabetes. J. Frailty Aging 2020, 9, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, K.; Kivimäki, M.; Hamer, M.; Shipley, M.J.; Akbaraly, T.N.; Tabak, A.; Singh-Manoux, A.; Batty, G.D. Diabetes risk factors, diabetes risk algorithms, and the prediction of future frailty: The Whitehall II prospective cohort study. J. Am. Med. Dir. Assoc. 2013, 14, 851.e1–851.e6. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Wang, J.; Huang, J.W.; Chan, D.C.; Chien, K.L.; COhort of GEriatric Nephrology in NTUH (COGENT) Study Group. Hypoglycemic episodes are associated with an increased risk of incident frailty among new onset diabetic patients. J. Diabetes Complicat. 2020, 34, 107492. [Google Scholar] [CrossRef] [PubMed]
- García-Esquinas, E.; Graciani, A.; Guallar-Castillón, P.; López-García, E.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Diabetes and risk of frailty and its potential mechanisms: A prospective cohort study of older adults. J. Am. Med. Dir. Assoc. 2015, 16, 748–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denicolò, S.; Perco, P.; Thöni, S.; Mayer, G. Non-adherence to antidiabetic and cardiovascular drugs in type 2 diabetes mellitus and its association with renal and cardiovascular outcomes: A narrative review. J. Diabetes Complicat. 2021, 35, 107931. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayer, A.A.; Dennison, E.M.; Syddall, H.E.; Gilbody, H.J.; Phillips, D.I.; Cooper, C. Type 2 diabetes, muscle strength, and impaired physical function: The tip of the iceberg? Diabetes Care 2005, 28, 2541–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourdel-Marchasson, I.; Catheline, G.; Regueme, S.; Danet-Lamasou, M.; Barse, E.; Ratsimbazafy, F.; Rodriguez-Manas, L.; Hood, K.; Sinclair, A.J. Frailty and Brain-Muscle Correlates in Older People with Type 2 Diabetes: A structural-MRI Explorative Study. J. Nutr. Health Aging 2019, 23, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Gundmi, S.; Maiya, A.G.; Bhat, A.K.; Ravishankar, N.; Hande, M.H.; Rajagopal, K.V. Hand dysfunction in type 2 diabetes mellitus: Systematic review with meta-analysis. Ann. Phys. Rehabil. Med. 2018, 61, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Motta, F.; Sica, A.; Selmi, C. Frailty in Rheumatic Diseases. Front. Immunol. 2020, 29, 576134. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Toscani, M.; Colaizzi, J. Telepharmacy: A New Paradigm for Our Profession. J. Pharm. Pract. 2020, 33, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Ishikawa, J.; Fujiwara, Y.; Tanaka, M.; Kanazawa, N.; Chiba, Y.; Iizuka, A.; Kaito, S.; Tanaka, J.; Sugie, M.; et al. Prevalence of frailty, cognitive impairment, and sarcopenia in outpatients with cardiometabolic disease in a frailty clinic. BMC Geriatr. 2018, 18, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munshi, M.N. Cognitive dysfunction in older adults with diabetes: What a clinician needs to know. Diabetes Care 2017, 40, 461–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljohani, W.; Algohani, L.; Alzahrani, A.; Bazuhair, M.; Bawakid, A.; Aljuid, L.; Al-Ahdal, A. Prevalence of Depression Among Patients With Type 2 Diabetes at King Abdullah Medical City. Cureus 2021, 13, e18447. [Google Scholar] [CrossRef] [PubMed]
- Mathur, D.; Anand, A.; Srivastava, V.; Patil, S.S.; Singh, A.; Rajesh, S.K.; Nagendra, H.R.; Nagarathna, R. Depression in High-Risk Type 2 Diabetes Adults. Ann. Neurosci. 2020, 27, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.; El Assar, M.; Rodríguez-Mañas, L. Frailty and sarcopenia as the basis for the phenotypic manifestation of chronic diseases in older adults. Mol. Asp. Med. 2016, 50, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, B.; Chudiak, A.; Uchmanowicz, I.; Mazur, G. How May Coexisting Frailty Influence Adherence to Treatment in Elderly Hypertensive Patients? Int. J. Hypertens. 2019, 2019, 5245184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankowska-Polańska, B.; Dudek, K.; Szymanska-Chabowska, A.; Uchmanowicz, I. The influence of frailty syndrome on medication adherence among elderly patients with hypertension. Clin. Interv. Aging 2016, 11, 1781–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, X.; Tian, X.; Liu, N.; Dong, L.; Jin, Y.; Si, H.; Liu, X.; Wang, C. The association between frailty and medication adherence among community-dwelling older adults with chronic diseases: Medication beliefs acting as mediators. Patient Educ. Couns. 2020, 103, 2548–2554. [Google Scholar] [CrossRef] [PubMed]
- Strain, W.D.; Down, S.; Brown, P.; Puttanna, A.; Sinclair, A. Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes. Diabetes Ther. 2021, 12, 1227–1247. [Google Scholar] [CrossRef] [PubMed]
- Horii, T.; Momo, K.; Yasu, T.; Kabeya, Y.; Atsuda, K. Determination of factors affecting medication adherence in type 2 diabetes mellitus patients using a nationwide claim-based database in Japan. PLoS ONE 2019, 14, e0223431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demoz, G.T.; Wahdey, S.; Bahrey, D.; Kahsay, H.; Woldu, G.; Niriayo, Y.L.; Collier, A. Predictors of poor adherence to antidiabetic therapy in patients with type 2 diabetes: A cross-sectional study insight from Ethiopia. Diabetol. Metab. Syndr. 2020, 16, 62. [Google Scholar] [CrossRef] [PubMed]
- Aloudah, N.M.; Scott, N.W.; Aljadhey, H.S.; Araujo-Soares, V.; Alrubeaan, K.A.; Watson, M.C. Medication adherence among patients with Type 2 diabetes: A mixed methods study. PLoS ONE 2018, 13, e0207583. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, T.; Lekhanth, A.; Revanth, A.; Gopinaht, C.; Babu, S.C. Effect of Polypharmacy on Medication Adherence in Patients with Type 2 Diabetes mellitus. Indian J. Phar. Pract. 2015, 8, 126–132. [Google Scholar] [CrossRef]
- Akgol, J.; Erhan, E.; Ercument, O. Factors predicting treatment compliance among hypertensive patients in an urban area. Med. Sci. Int. Med. J. 2017, 6, 447–456. [Google Scholar] [CrossRef]
- Awad, A.; Alhadab, A.; Albassam, A. Medication-Related Burden and Medication Adherence among Geriatric Patients in Kuwait: A Cross-Sectional Study. Front. Pharmacol. 2020, 11, 1296. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (n = 175) | |
|---|---|---|
| Gender | Women | 87 (49.71%) |
| Men | 88 (50.29%) | |
| Age | M ± SD | 70.25 ± 6.70 |
| median | 69 | |
| Q1–Q3 | 65–74 | |
| Marital status | Single | 58 (33.14%) |
| In relationship | 117 (66.86%) | |
| Place of residence | Village | 21 (12.00%) |
| City | 154 (88.00%) | |
| Education | Primary | 19 (10.86%) |
| Occupational | 44 (25.14%) | |
| Secondary | 80 (45.71%) | |
| High | 32 (18.29%) | |
| Diabetes duration [years] | M ± SD | 12.1 ± 8.52 |
| median | 10 | |
| Q1–Q3 | 5–15 | |
| Number of all daily medications | M ± SD | 8.07 ± 4.42 |
| median | 7 | |
| Q1–Q3 | 6–10 | |
| Number of anti-diabetes medications taken daily | M ± SD | 1.81 ± 1.25 |
| median | 2 | |
| Q1–Q3 | 1–3 | |
| Diabetes treatment method | Oral anti-diabetes medications | 106 (60.57%) |
| Insulin | 31 (17.71%) | |
| Oral anti-diabetes medications and insulin | 33 (18.86%) | |
| non-pharmacological methods | 5 (2.86%) | |
| Body Mass Index (BMI) | normal body weight | 19 (10.86%) |
| overweight | 67 (38.29%) | |
| 1st degree obesity | 55 (31.43%) | |
| 2nd/3rd degree obesity | 34 (19.43%) | |
| Co-existent diseases: Hypertension | No | 32 (18.29%) |
| Yes | 143 (81.71%) | |
| Co-existent diseases: ischaemic heart disease | No | 113 (64.57%) |
| Yes | 62 (35.43%) | |
| Co-existent diseases: Rheumatic diseases | No | 130 (74.29%) |
| Yes | 45 (25.71%) | |
| Co-existent diseases: Kidney’s diseases | No | 140 (80.00%) |
| Yes | 35 (20.00%) | |
| Co-existent diseases: Respiratory system diseases | No | 137 (78.29%) |
| Yes | 38 (21.71%) | |
| Co-existent diseases: Locomotor system disorders | No | 121 (69.14%) |
| Yes | 54 (30.86%) | |
| Co-existent diseases: Diabetic foot syndrome | No | 137 (78.29%) |
| Yes | 38 (21.71%) | |
| Co-existent diseases: Eye diseases | No | 103 (58.86%) |
| Yes | 72 (41.14%) | |
| Instrument | Points | Interpretation | n | % |
|---|---|---|---|---|
| TFI | 0–4 | lack of frailty syndrome | 35 | 20.00% |
| 5 and more | frailty syndrome | 140 | 80.00% | |
| ACDS | 0–20 | low adherence | 39 | 22.29% |
| 21–26 | medium adherence | 101 | 57.71% | |
| 27–28 | high adherence | 35 | 20.00% |
| Instrument | N | M | SD | Mdn | Min | Max | Q1 | Q3 |
|---|---|---|---|---|---|---|---|---|
| ACDS | 175 | 23.13 | 3.72 | 24 | 13 | 28 | 21 | 26 |
| TFI total score | 175 | 6.95 | 2.75 | 7 | 0 | 13 | 5 | 9 |
| TFI: physical domain | 175 | 3.68 | 1.96 | 4 | 0 | 8 | 2 | 5 |
| TFI: psychological domain | 175 | 2.09 | 0.93 | 2 | 0 | 4 | 2 | 3 |
| TFI: social domain | 175 | 1.19 | 0.75 | 1 | 0 | 3 | 1 | 2 |
| Variables | ACDS | p | ||
|---|---|---|---|---|
| Adherent (n = 136) | Non-Adherent (n = 39) | |||
| Age | M ± SD | 69.64 ± 6.27 | 72.38 ± 7.72 | U = 2113.5 p = 0.053 |
| Me | 69 | 70 | ||
| Q1–Q3 | 65–73 | 67.5–76 | ||
| Gender | Women | 70 (51.47%) | 17 (43.59%) | chi2 = 0.471 p = 0.493 |
| Men | 66 (48.53%) | 22 (56.41%) | ||
| Marital status | Single | 40 (29.41%) | 18 (46.15%) | chi2 = 3.116 p = 0.078 |
| In relationship | 96 (70.59%) | 21 (53.85%) | ||
| Education | Primary | 14 (10.29%) | 5 (12.82%) | p = 0.457 |
| Occupational | 31 (22.79%) | 13 (33.33%) | ||
| Secondary | 64 (47.06%) | 16 (41.03%) | ||
| High | 27 (19.85%) | 5 (12.82%) | ||
| Place of residence | Village | 16 (11.76%) | 5 (12.82%) | p = 0.787 |
| City | 120 (88.24%) | 34 (87.18%) | ||
| Diabetes duration [years] | M ± SD | 11.88 ± 8.14 | 12.87 ± 9.81 | U = 2576 p = 0.786 |
| Me | 10 | 10 | ||
| Q1–Q3 | 15–5 | 5–18.5 | ||
| Number of anti-diabetes medications taken daily | M ± SD | 1.84 ± 1.3 | 1.69 ± 1.08 | U = 2788.5 p = 0.609 |
| Me | 2 | 2 | ||
| Q1–Q3 | 1–3 | 1–2 | ||
| Number of all daily medications | M ± SD | 8.11 ± 4.7 | 7.92 ± 3.32 | U = 2524 p = 0.645 |
| Me | 7 | 8 | ||
| Q1–Q3 | 5–10.25 | 6–10 | ||
| Body Mass Index (BMI) | normal body weight | 15 (11.03%) | 4 (10.26%) | p = 0.601 |
| overweight | 49 (36.03%) | 18 (46.15%) | ||
| 1st degree obesity | 43 (31.62%) | 12 (30.77%) | ||
| 2nd/3rd degree obesity | 29 (21.32%) | 5 (12.82%) | ||
| Co-existent diseases: Hypertension | No | 26 (19.12%) | 6 (15.38%) | chi2 = 0.088 p = 0.767 |
| Yes | 110 (80.88%) | 33 (84.62%) | ||
| Co-existent diseases: ischaemic heart disease | No | 90 (66.18%) | 23 (58.97%) | chi2 = 0.408 p = 0.523 |
| Yes | 46 (33.82%) | 16 (41.03%) | ||
| Co-existent diseases: Rheumatic diseases | No | 103 (75.74%) | 27 (69.23%) | chi2 = 0.374 p = 0.541 |
| Yes | 33 (24.26%) | 12 (30.77%) | ||
| Co-existent diseases: Kidney’s diseases | No | 111 (81.62%) | 29 (74.36%) | chi2 = 0.596 p = 0.44 |
| Yes | 25 (18.38%) | 10 (25.64%) | ||
| Co-existent diseases: Respiratory system diseases | No | 109 (80.15%) | 28 (71.79%) | chi2 = 0.801 p = 0.371 |
| Yes | 27 (19.85%) | 11 (28.21%) | ||
| Co-existent diseases: Locomotor system disorders | No | 95 (69.85%) | 26 (66.67%) | chi2 = 0.034 p = 0.855 |
| Yes | 41 (30.15%) | 13 (33.33%) | ||
| Co-existent diseases: Diabetic foot syndrome | No | 109 (80.15%) | 28 (71.79%) | chi2 = 0.801 p = 0.371 |
| Yes | 27 (19.85%) | 11 (28.21%) | ||
| Co-existent diseases: Eye diseases | No | 81 (59.56%) | 22 (56.41%) | chi2 = 0.028 p = 0.867 |
| Yes | 55 (40.44%) | 17 (43.59%) | ||
| Diabetes treatment method | Oral anti-diabetes medications | 81 (59.56%) | 25 (64.10%) | p = 0.683 |
| Insulin | 23 (16.91%) | 8 (20.51%) | ||
| Oral anti-diabetes medications and insulin | 27 (19.85%) | 6 (15.38%) | ||
| non-pharmacological methods | 5 (3.68%) | 0 (0.00%) | ||
| Tilburg Frailty Indicator (TFI) | ACDS | p | |||
|---|---|---|---|---|---|
| Low Adherence—A (n = 39) | Medium Adherence—B (n = 101) | High Adherence—C (n = 35) | |||
| TFI total score | M ± SD | 8.62 ± 2.27 | 6.64 ± 2.69 | 6 ± 2.72 | p < 0.001 * A > B, C |
| Mdn | 9 | 6 | 6 | ||
| Q1–Q3 | 7–10 | 5–9 | 4.5–8 | ||
| TFI: physical domain | M ± SD | 4.87 ± 1.64 | 3.43 ± 1.94 | 3.09 ± 1.82 | p < 0.001 * A > B, C |
| Mdn | 5 | 4 | 3 | ||
| Q1–Q3 | 4–6 | 2–5 | 2–4.5 | ||
| TFI: psychological domain | M ± SD | 2.44 ± 0.99 | 2.02 ± 0.91 | 1.89 ± 0.83 | p = 0.034 * A > B, C |
| Mdn | 2 | 2 | 2 | ||
| Q1–Q3 | 2–3 | 2–2 | 1–2 | ||
| TFI: social domain | M ± SD | 1.31 ± 0.92 | 1.2 ± 0.69 | 1.03 ± 0.66 | p = 0.339 |
| Mdn | 1 | 1 | 1 | ||
| Q1–Q3 | 1–2 | 1–2 | 1–1 | ||
| Variables | OR | 95% CI | p | ||
|---|---|---|---|---|---|
| Tilburg Frailty Indicator (total score) | 1.558 | 1.245 | 1.95 | <0.001 * | |
| Age | (years) | 1.062 | 0.98 | 1.152 | 0.144 |
| Gender | Women | 1 | ref. | ||
| Men | 2.954 | 1.044 | 8.353 | 0.041 * | |
| Marital status | Single | 1 | ref. | ||
| In relationship | 0.524 | 0.175 | 1.565 | 0.247 | |
| Education | Primary | 1 | ref. | ||
| Occupational | 3.609 | 0.562 | 23.184 | 0.176 | |
| Secondary | 0.854 | 0.155 | 4.717 | 0.856 | |
| High | 1.11 | 0.132 | 9.328 | 0.923 | |
| Place of residence | Village | 1 | ref. | ||
| City | 0.554 | 0.125 | 2.448 | 0.436 | |
| Body Mass Index (BMI) | normal body weight | 1 | ref. | ||
| overweight | 1.839 | 0.374 | 9.048 | 0.454 | |
| 1st degree obesity | 1.747 | 0.347 | 8.786 | 0.499 | |
| 2nd/3rd degree obesity | 0.728 | 0.121 | 4.375 | 0.728 | |
| Co-existent diseases: Hypertension | No | 1 | ref. | ||
| Yes | 3.111 | 0.76 | 12.729 | 0.114 | |
| Co-existent diseases: Ischemic heart disease | No | 1 | ref. | ||
| Yes | 1.271 | 0.476 | 3.399 | 0.632 | |
| Co-existent diseases: Rheumatic diseases | No | 1 | ref. | ||
| Yes | 2.223 | 0.667 | 7.407 | 0.193 | |
| Co-existent diseases: Kidney’s diseases | No | 1 | ref. | ||
| Yes | 1.946 | 0.553 | 6.854 | 0.3 | |
| Co-existent diseases: Respiratory system diseases | No | 1 | ref. | ||
| Yes | 1.119 | 0.361 | 3.471 | 0.846 | |
| Co-existent diseases: Locomotor system disorders | No | 1 | ref. | ||
| Yes | 0.926 | 0.324 | 2.646 | 0.886 | |
| Co-existent diseases: Diabetic foot syndrome | No | 1 | ref. | ||
| Yes | 0.384 | 0.106 | 1.391 | 0.145 | |
| Co-existent diseases: Eye diseases | No | 1 | ref. | ||
| Yes | 1.149 | 0.402 | 3.285 | 0.796 | |
| Diabetes duration [years] | [years] | 0.97 | 0.908 | 1.035 | 0.358 |
| Diabetes treatment method | Oral anti-diabetes medications | 1 | ref. | ||
| Insulin | 0.778 | 0.119 | 5.086 | 0.793 | |
| Oral anti-diabetes medications and insulin | 1.112 | 0.281 | 4.392 | 0.88 | |
| non-pharmacological methods | 0 | 0 | Inf | 0.991 | |
| Number of anti-diabetes medications taken daily | 0.78 | 0.401 | 1.514 | 0.462 | |
| Number of all daily medications | 0.847 | 0.728 | 0.984 | 0.03 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonikowska, I.; Szwamel, K.; Uchmanowicz, I. Adherence to Medication in Older Adults with Type 2 Diabetes Living in Lubuskie Voivodeship in Poland: Association with Frailty Syndrome. J. Clin. Med. 2022, 11, 1707. https://doi.org/10.3390/jcm11061707
Bonikowska I, Szwamel K, Uchmanowicz I. Adherence to Medication in Older Adults with Type 2 Diabetes Living in Lubuskie Voivodeship in Poland: Association with Frailty Syndrome. Journal of Clinical Medicine. 2022; 11(6):1707. https://doi.org/10.3390/jcm11061707
Chicago/Turabian StyleBonikowska, Iwona, Katarzyna Szwamel, and Izabella Uchmanowicz. 2022. "Adherence to Medication in Older Adults with Type 2 Diabetes Living in Lubuskie Voivodeship in Poland: Association with Frailty Syndrome" Journal of Clinical Medicine 11, no. 6: 1707. https://doi.org/10.3390/jcm11061707