
Effect of Music Intervention on Lung Expansion Exercises after Cardiothoracic Surgery

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Randomization
2.4. Data Collection
2.5. Statistics
3. Results
3.1. Differences between the Normal Distribution and the Two Groups before the Trial
3.2. Music of Model Effects in Pulmonary Function in the Music Group and the Control Group
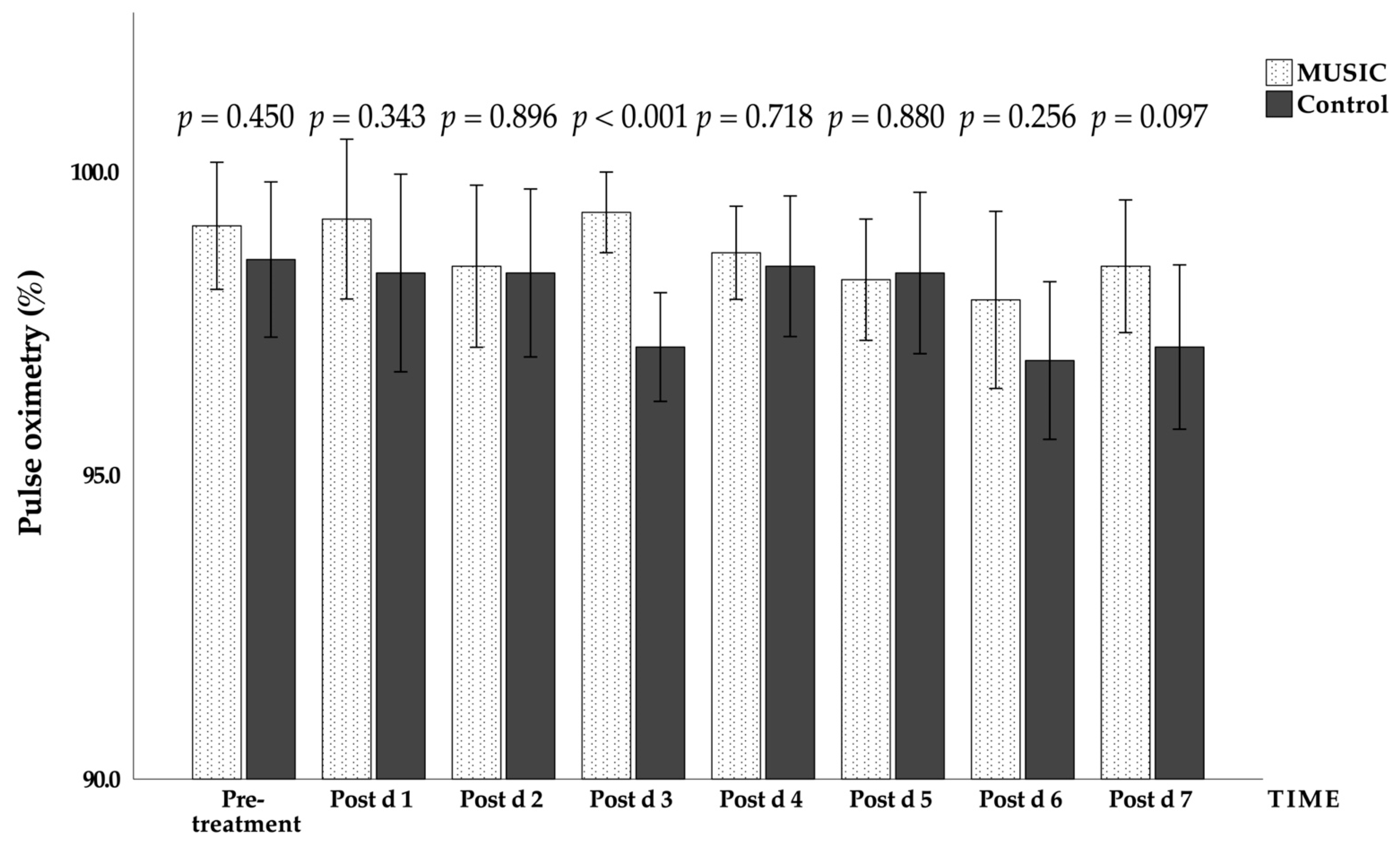
3.3. Effects of Music on Vital Signs and Visual Analogue Scale for Pain in the Music Group and the Control Group
3.4. Changes of State-Trait Anxiety Scale before and after Surgery in the Control Group and the Music Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- McCaffrey, R.G.; Good, M. The lived experience of listening to music while recovering from surgery. J. Holist. Nurs. 2000, 18, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Yozbatiran, N.; Gelecek, N.; Karadibak, D. Influence of physiotherapy programme on peak expiratory flow rate (PEFR) and chest expansion in patients with neck and low back pain. J. Back Musculoskelet. Rehabil. 2006, 19, 35–40. [Google Scholar] [CrossRef]
- Heo, J.; Baek, H.J.; Hong, S.; Chang, M.H.; Lee, J.S.; Park, K.S. Music and natural sounds in an auditory steady-state response based brain–computer interface to increase user acceptance. Comput. Biol. Med. 2017, 84, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B. Chapter 10—Sleep and Respiratory Physiology. In Fundamentals of Sleep Medicine; Berry, R.B., Ed.; W.B. Saunders: St. Louis, MO, USA, 2012; pp. 141–157. [Google Scholar]
- Ramsay, M.; Polkey, M.I.; Hart, N. Chapter 64—Diseases of the Thoracic Cage and Respiratory Muscles. In Clinical Respiratory Medicine, 4th ed.; Spiro, S.G., Silvestri, G.A., Agustí, A., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2012; pp. 763–775. [Google Scholar]
- Laveneziana, P.; Albuquerque, A.; Aliverti, A.; Babb, T.; Barreiro, E.; Dres, M.; Dubé, B.-P.; Fauroux, B.; Gea, J.; Guenette, J.A.; et al. ERS Statement on Respiratory Muscle Testing at Rest and during Exercise. Eur. Respir. J. 2019, 53, 1801214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelley, R.C.; Ferreira, L.F. Diaphragm abnormalities in heart failure and aging: Mechanisms and integration of cardiovascular and respiratory pathophysiology. Heart Fail. Rev. 2017, 22, 191–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, V.; Aziz, K.B.K.; Kamaruddin, K.; Leonard, J.H.; Das, S.; Jagannathan, M.G. Effect of intercostal stretch on pulmonary function parameters among healthy males. EXCLIJ 2012, 11, 284. [Google Scholar]
- Ishida, H.; Suehiro, T.; Watanabe, S. Comparison of abdominal muscle activity and peak expiratory flow between forced vital capacity and fast expiration exercise. J. Phys. Ther. Sci. 2017, 29, 563–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jinakote, M.; Pongpanit, K. Correlations between change in neural respiratory drive and heart rate variability in patients submitted to open-heart surgery. J. Exerc. Rehabil. 2019, 15, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss-Blasche, G.; Moser, M.; Voica, M.; McLeod, D.R.; Klammer, N.; Marktl, W. Relative timing of inspiration and expiration affects respiratory sinus arrhythmia. Clin. Exp. Pharmacol. Physiol. 2000, 27, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, M.; Kobayashi, A.; Kawasaki, C. Heart rate variability with repetitive exposure to music. Biol. Psychol. 2005, 70, 61–66. [Google Scholar] [CrossRef] [PubMed]
- De Troyer, A. Interaction between the canine diaphragm and intercostal muscles in lung expansion. J. Appl. Physiol. 2005, 98, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Cimen, S.G.; Oğuz, E.; Gundogmus, A.G.; Cimen, S.; Sandikci, F.; Ayli, M.D. Listening to music during arteriovenous fistula surgery alleviates anxiety: A randomized single-blind clinical trial. World J. Transplant. 2020, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Cortinez, L.I.; Hsu, Y.W.; Sum-Ping, S.T.; Young, C.; Keifer, J.C.; Macleod, D.; Robertson, K.M.; Wright, D.R.; Moretti, E.W.; Somma, J.; et al. Dexmedetomidine Pharmacodynamics: Part II Crossover Comparison of the Analgesic Effect of Dexmedetomidine and Remifentanil in Healthy Volunteers. Anesthesiol. J. Am. Soc. Anesthesiol. 2004, 101, 1077–1083. [Google Scholar]
- Vetter, D.; Barth, J.; Uyulmaz, S.; Vonlanthen, R.; Belli, G.; Montorsi, M.; Bismuth, H.; Witt, C.M.; Clavien, P.-A. Effects of art on surgical patients: A systematic review and meta-analysis. Ann. Surg. 2015, 262, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erkilic, E.; Kesimci, E.; Soykut, C.; Doger, C.; Gumus, T.; Kanbak, O. Factors associated with preoperative anxiety levels of Turkish surgical patients: From a single center in Ankara. Patient Prefer. Adherence 2017, 11, 291. [Google Scholar] [CrossRef] [PubMed]
- Karanci, A.; Dirik, G. Predictors of pre-and postoperative anxiety in emergency surgery patients. J. Psychosom. Res. 2003, 55, 363–369. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Music Group (n = 9) | Control Group (n = 9) | p | |
|---|---|---|---|
| Sex | 0.576 | ||
| Male | 6 (66.7%) | 8 (88.9%) | |
| Female | 3 (33.3%) | 1 (11.1%) | |
| Type of cardiac disease | |||
| Coronary heart disease (n = 7) | 3 (33.3%) | 4 (44.4%) | |
| Valvular heart disease (n = 6) | 2 (22.2%) | 4 (44.4%) | |
| Aortic dissection (n = 3) | 2 (22.2%) | 1 (11.1%) | |
| Atrial septal defect (n = 1) | 1 (11.1%) | 0 (0.0%) | |
| Cardiac tumor (n = 1) | 1 (11.1%) | 0 (0.0%) |
| Music Group (n = 9) | Control Group (n = 9) | W | |
|---|---|---|---|
| Age | 58.44 ± 10.06 | 63.11 ± 11.80 | 0.380 |
| Height (cm) | 164.18 ± 8.15 | 165.53 ± 9.46 | 0.749 |
| Weight (kg) | 73.79 ± 10.23 | 70.03 ± 6.40 | 0.364 |
| Body mass index (kg/m2) | 27.43 ± 3.81 | 25.74 ± 3.52 | 0.343 |
| Heartbeat (bpm) | 78 ± 12.40 | 85 ± 8.54 | 0.196 |
| Systolic blood pressure (mmHg) | 132.11 ± 21.44 | 125.67 ± 18.26 | 0.502 |
| Diastolic blood pressure (mmHg) | 72.11 ± 17.86 | 65.22 ± 9.85 | 0.326 |
| Blood oxygen saturation (%) | 96.44 ± 2.96 | 97.33 ± 2.23 | 0.483 |
| Vital capacity (mL/kg) | 27.82 ± 10.38 | 23.76 ± 5.46 | 0.315 |
| Maximal inspiratory pressure (cmH2O) | 73.33 ± 24.68 | 56.33 ± 18.24 | 0.116 |
| Maximal expiratory pressure (cmH2O) | 92.44 ± 37.38 | 67.89 ± 16.04 | 0.089 |
| Peak expiratory flow rate (L/min) | 377.78 ± 129.69 | 371.11 ± 125.44 | 0.913 |
| State anxiety scale | 55.22 ± 11.16 | 52.22 ± 8.23 | 0.525 |
| Trait anxiety scale | 49.33 ± 14.12 | 55.78 ± 7.98 | 0.251 |
| Assessment | Group | Time | Group × Time | |||
|---|---|---|---|---|---|---|
| p | η2 | p | η2 | p | η2 | |
| PEFR | 0.957 | 0.000 | <0.001 | 0.831 | 0.022 | 0.451 |
| VC | 0.567 | 0.018 | <0.001 | 0.811 | 0.045 | 0.417 |
| MIP | 0.145 | 0.105 | <0.001 | 0.755 | <0.001 | 0.673 |
| MEP | 0.382 | 0.041 | <0.001 | 0.844 | 0.243 | 0.306 |
| Assessment | Group | Time | Group × Time | |||
|---|---|---|---|---|---|---|
| p | η2 | p | η2 | p | η2 | |
| HR | 0.420 | 0.458 | 0.066 | 0.396 | 0.306 | 0.285 |
| SBP | 0.797 | 0.004 | 0.049 | 0.412 | 0.115 | 0.363 |
| DBP | 0.756 | 0.005 | 0.170 | 0.335 | 0.468 | 0.238 |
| SpO2 | 0.010 | 0.268 | 0.010 | 0.484 | 0.003 | 0.523 |
| VAS | 0.046 | 0.178 | <0.001 | 0.739 | 0.155 | 0.353 |
| Group | Δmean | S.E. | F | p-Value | |
|---|---|---|---|---|---|
| STAI-S | Music | −5.667 | 5.7228 | 0.956 | 0.171 |
| Control | −0.444 | 9.3020 | |||
| STAI-T | Music | 4.111 | 12.3130 | 0.392 | 0.671 |
| Control | 1.889 | 9.2256 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.-Y.; Guo, L.-Y.; Chuang, I.-C.; Kuo, H.-C.; Tsai, Y.-C.; Liu, S.-F. Effect of Music Intervention on Lung Expansion Exercises after Cardiothoracic Surgery. J. Clin. Med. 2022, 11, 1589. https://doi.org/10.3390/jcm11061589
Chen G-Y, Guo L-Y, Chuang I-C, Kuo H-C, Tsai Y-C, Liu S-F. Effect of Music Intervention on Lung Expansion Exercises after Cardiothoracic Surgery. Journal of Clinical Medicine. 2022; 11(6):1589. https://doi.org/10.3390/jcm11061589
Chicago/Turabian StyleChen, Guan-Yi, Lan-Yuen Guo, I-Chun Chuang, Ho-Chang Kuo, Yuh-Chyn Tsai, and Shih-Feng Liu. 2022. "Effect of Music Intervention on Lung Expansion Exercises after Cardiothoracic Surgery" Journal of Clinical Medicine 11, no. 6: 1589. https://doi.org/10.3390/jcm11061589