
Multidimensional Family-Centred Early Intervention in Children with Hearing Loss: A Conceptual Model


{kind=link}
Abstract
:1. Introduction
1.1. Children with Hearing Loss
1.2. Families with Children with HL
1.3. Early Intervention
2. Aims and Methods
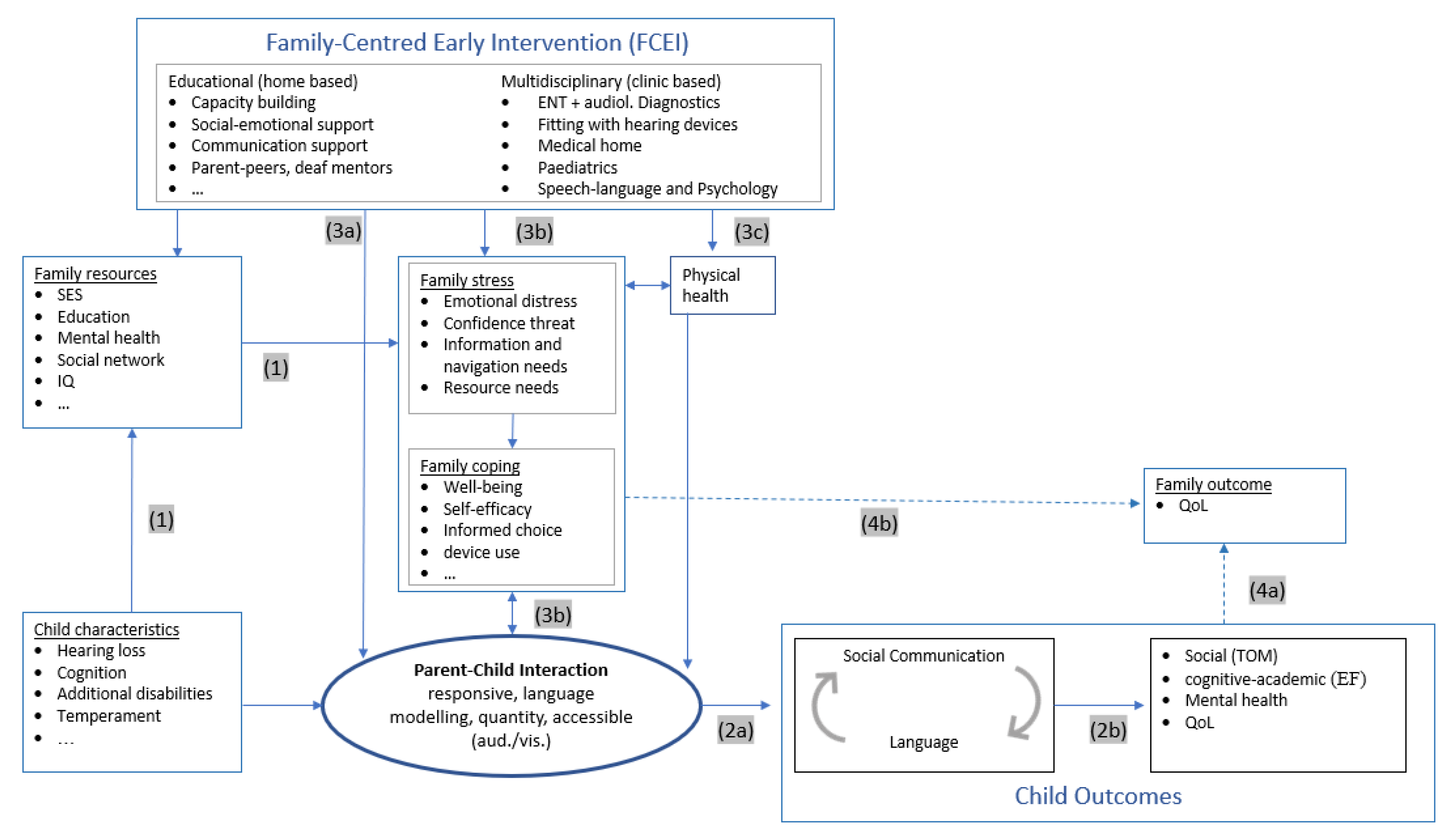
- Effects of a child’s HL on the family (1);
- Effects of parent–child interaction on child language/communication (2a) and more distal domains of child development (2b);
- Effects of Early Intervention on parent–child interaction and child developmental outcomes:
- Family-centred education early intervention (3a) and
- Multidisciplinary clinical intervention (3b).
- Effects of Early intervention on family quality of life (4).
3. Conceptual Model

3.1. Effects of a Child’s HL on the Family (1)
3.1.1. Family Emotional Distress
3.1.2. Confidence Threat
3.1.3. Resource Needs
3.1.4. Navigation and Information Needs
3.1.5. Family Stress over the Course of Time
3.2. Effects of Parent–Child interaction on Child Development (2a)
3.2.1. Style of Parent–Child Interaction
3.2.2. Quantity of Parent–Child Interaction
3.2.3. Quality of Parent–Child Communication
3.2.4. Social Communication
3.2.5. Effects of Social Communication and Language Skills
3.3. Effects of Family-Centred Early Intervention on Parent–Child Interaction and Child Developmental Outcomes
3.3.1. Direct Influences of Early Intervention on Parent–Child Interaction
3.3.2. Indirect Influence of Early Intervention on Parent–Child Interaction
3.3.3. Effects of Multidisciplinary Intervention
Early Identification of HL
Device Fitting
Diagnostic and Genetic Counselling
Effect on Child Physical Health (3c)
Case Management of Children with Additional/Multiple Disabilities
Developmental Surveillance
3.4. Influences on Family Quality of Life (4)
4. Implications for Practice and Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Childhood Hearing Loss: Strategies for Prevention and Care. Available online: https://www.who.int/publications/i/item/childhood-hearing-loss-strategies-for-prevention-and-care (accessed on 18 January 2022).
- Bussé, A.M.L.; Hoeve, H.L.J.; Nasserinejad, K.; Mackey, A.R.; Simonsz, H.J.; Goedegebure, A. Prevalence of permanent neonatal hearing impairment: Systematic review and Bayesian meta-analysis. Int. J. Audiol. 2020, 59, 475–485. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Estimates on Prevalence of Hearing Loss: Prevention of Deafness. Available online: https://www.who.int/pbd/deafness/estimates/en/ (accessed on 22 January 2022).
- Gallaudet Research Institute. Regional and National Summary Report of Data from the 2009–2010 Annual Survey of Deaf and Hard of Hearing Children and Youth. Available online: https://research.gallaudet.edu/Demographics/2010_National_Summary.pdf (accessed on 20 January 2022).
- Van Naarden Braun, K.; Christensen, D.; Doernberg, N.; Schieve, L.; Rice, C.; Wiggins, L.; Schendel, D.; Yeargin-Allsopp, M. Trends in the prevalence of autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, and vision impairment, metropolitan atlanta, 1991–2010. PLoS ONE 2015, 10, e0124120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GeneReviews® [Internet]; Shearer, A.E.; Hildebrand, M.S.; Smith, R.J.H. (Eds.) University of Washington: Seattle, WA, USA, 2017. [Google Scholar]
- Moeller, M.P. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 2000, 106, E43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinaga-Itano, C.; Sedey, A.L.; Coulter, D.K.; Mehl, A.L. Language of early- and later-identified children with hearing loss. Pediatrics 1998, 102, 1161–1171. [Google Scholar] [CrossRef] [Green Version]
- Watkin, P.; McCann, D.; Law, C.; Mullee, M.; Petrou, S.; Stevenson, J.; Worsfold, S.; Yuen, H.M.; Kennedy, C. Language ability in children with permanent hearing impairment: The influence of early management and family participation. Pediatrics 2007, 120, e694–e701. [Google Scholar] [CrossRef]
- Pimperton, H.; Blythe, H.; Kreppner, J.; Mahon, M.; Peacock, J.L.; Stevenson, J.; Terlektsi, E.; Worsfold, S.; Yuen, H.M.; Kennedy, C.R. The impact of universal newborn hearing screening on long-term literacy outcomes: A prospective cohort study. Arch. Dis. Child. 2016, 101, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Yoshinaga-Itano, C.; Sedey, A.L.; Wiggin, M.; Chung, W. Early Hearing Detection and Vocabulary of Children with Hearing Loss. Pediatrics 2017, 140, e20162964. [Google Scholar] [CrossRef] [Green Version]
- Sarant, J.Z.; Holt, C.M.; Dowell, R.C.; Rickards, F.W.; Blamey, P.J. Spoken language development in oral preschool children with permanent childhood deafness. J. Deaf Stud. Deaf Educ. 2009, 14, 205–217. [Google Scholar] [CrossRef] [Green Version]
- Cupples, L.; Ching, T.Y.; Button, L.; Seeto, M.; Zhang, V.; Whitfield, J.; Gunnourie, M.; Martin, L.; Marnane, V. Spoken language and everyday functioning in 5-year-old children using hearing aids or cochlear implants. Int. J. Audiol. 2018, 57, S55–S69. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Dillon, H. Major findings of the LOCHI study on children at 3 years of age and implications for audiological management. Int. J. Audiol. 2013, 52 (Suppl. S2), S65–S68. [Google Scholar] [CrossRef] [Green Version]
- Szarkowski, A.; Toe, D. Pragmatics in Deaf and Hard of Hearing Children: An Introduction. Pediatrics 2020, 146, S231–S236. [Google Scholar] [CrossRef] [PubMed]
- Crowe, K.; Dammeyer, J. A Review of the Conversational Pragmatic Skills of Children WITH Cochlear Implants. J. Deaf Stud. Deaf Educ. 2021, 26, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Goberis, D.; Beams, D.; Dalpes, M.; Abrisch, A.; Baca, R.; Yoshinaga-Itano, C. The missing link in language development of deaf and hard of hearing children: Pragmatic language development. Semin. Speech Lang. 2012, 33, 297–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theunissen, S.C.P.M.; Rieffe, C.; Netten, A.P.; Briaire, J.J.; Soede, W.; Schoones, J.W.; Frijns, J.H.M. Psychopathology and its risk and protective factors in hearing-impaired children and adolescents: A systematic review. JAMA Pediatr. 2014, 168, 170–177. [Google Scholar] [CrossRef]
- Sarant, J.Z.; Harris, D.C.; Galvin, K.L.; Bennet, L.A.; Canagasabey, M.; Busby, P.A. Social Development in Children with Early Cochlear Implants: Normative Comparisons and Predictive Factors, Including Bilateral Implantation. Ear Hear. 2018, 39, 770–782. [Google Scholar] [CrossRef]
- Luckner, J.L.; Handley, C.M. A summary of the reading comprehension research undertaken with students who are deaf or hard of hearing. Am. Ann. Deaf 2008, 153, 6–36. [Google Scholar] [CrossRef]
- Geers, A.E.; Hayes, H. Reading, writing, and phonological processing skills of adolescents with 10 or more years of cochlear implant experience. Ear Hear. 2011, 32, 49S–59S. [Google Scholar] [CrossRef] [Green Version]
- Meinzen-Derr, J.; Wiley, S.; Grove, W.; Altaye, M.; Gaffney, M.; Satterfield-Nash, A.; Folger, A.T.; Peacock, G.; Boyle, C. Kindergarten Readiness in Children Who Are Deaf or Hard of Hearing Who Received Early Intervention. Pediatrics 2020, 146, e20200557. [Google Scholar] [CrossRef]
- Schick, B.; de Villiers, P.; de Villiers, J.; Hoffmeister, R. Language and theory of mind: A study of deaf children. Child Dev. 2007, 78, 376–396. [Google Scholar] [CrossRef]
- Netten, A.P.; Rieffe, C.; Soede, W.; Dirks, E.; Korver, A.M.H.; Konings, S.; Briaire, J.J.; Oudesluys-Murphy, A.M.; Dekker, F.W.; Frijns, J.H.M. Can You Hear What I Think? Theory of Mind in Young Children with Moderate Hearing Loss. Ear Hear. 2017, 38, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Beer, J.; Kronenberger, W.G.; Castellanos, I.; Colson, B.G.; Henning, S.C.; Pisoni, D.B. Executive functioning skills in preschool-age children with cochlear implants. J. Speech Lang. Hear. Res. 2014, 57, 1521–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronenberger, W.G.; Colson, B.G.; Henning, S.C.; Pisoni, D.B. Executive functioning and speech-language skills following long-term use of cochlear implants. J. Deaf Stud. Deaf Educ. 2014, 19, 456–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueras, B.; Edwards, L.; Langdon, D. Executive function and language in deaf children. J. Deaf Stud. Deaf Educ. 2008, 13, 362–377. [Google Scholar] [CrossRef]
- Sameroff, A.J.; Fiese, B.H. Transactional regulation and early intervention. In Handbook of Early Childhood Intervention; Meisels, S.J., Shonkoff, J.P., Eds.; Cambridge University Press: Cambridge, UK, 1990; pp. 119–149. [Google Scholar]
- Mitchell, R.E.; Karchmer, M.A. Chasing the Mythical Ten Percent: Parental Hearing Status of Deaf and Hard of Hearing Students in the United States. Sign Lang. Stud. 2004, 4, 138–163. [Google Scholar] [CrossRef]
- American Academy of Pediatrics, Joint Committee on Infant Hearing. Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Pediatrics 2007, 120, 898–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeller, M.P.; Carr, G.; Seaver, L.; Stredler-Brown, A.; Holzinger, D. Best practices in family-centered early intervention for children who are deaf or hard of hearing: An international consensus statement. J. Deaf Stud. Deaf Educ. 2013, 18, 429–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinaga-Itano, C. Principles and guidelines for early intervention after confirmation that a child is deaf or hard of hearing. J. Deaf Stud. Deaf Educ. 2014, 19, 143–175. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Is early intervention effective? Early Child. Educ J 1974, 2, 14–18. [Google Scholar] [CrossRef]
- Dunst, C.J.; Espe-Sherwindt, M. Family-Centered Practices in Early Childhood Intervention. In Handbook of Early Childhood Special Education; Reichow, B., Boyd, B.A., Barton, E.E., Odom, S.L., Eds.; Springer: Cham, Switzerland, 2016; pp. 37–55. ISBN 978-3-319-28490-3. [Google Scholar]
- Espe-Sherwindt, M.; Serrano, A. It takes two: The role of family-centered practices in communication intervention. Revista de Logopedia, Foniatría y Audiología 2016, 36, 162–169. [Google Scholar] [CrossRef]
- Guralnick, M.J. Effective Early Intervention: The Developmental Systems Approach, 1st ed.; Brookes Publishing: Newburyport, MA, USA, 2019; ISBN 9781681252896. [Google Scholar]
- Trivette, C.M.; Dunst, C.J.; Hamby, D.W. Influences of Family-Systems Intervention Practices on Parent-Child Interactions and Child Development. Top. Early Child. Spec. Educ. 2010, 30, 3–19. [Google Scholar] [CrossRef]
- Dunst, C.J.; Trivette, C.M.; Hamby, D.W. Meta-analysis of family-centered helpgiving practices research. Ment. Retard. Dev. Disabil. Res. Rev. 2007, 13, 370–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, U. Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1997; ISBN 9780674224575. [Google Scholar]
- Bronfenbrenner, U. Environments in developmental perspective: Theoretical and operational models. In Measuring Environment Across the Life Span: Emerging Methods and Concepts, 1st ed.; Friedman, S.L., Wachs, T.D., Eds.; American Psychological Assoc: Washington, DC, USA, 1999; pp. 3–28. ISBN 1-55798-561-8. [Google Scholar]
- Roberts, M.Y.; Kaiser, A.P. The Effectiveness of Parent-Implemented Language Interventions: A Meta-Analysis. Am. J. Speech Lang. Pathol. 2011, 20, 180–199. [Google Scholar] [CrossRef]
- Tamis-LeMonda, C.S.; Bornstein, M.H. Maternal responsiveness and early language acquisition. In Advances in Child Development and Behavior, 1st ed.; Reese, H.W., Kail, R.V., Eds.; Elsevier: Amsterdam, The Netherlands, 2002; pp. 89–127. ISBN 9780120097296. [Google Scholar]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.P.; Bruinsma, Y.; et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buschmann, A. Heidelberger Elterntraining frühe Sprachförderung: HET Late Talkers, 3rd ed.; Elsevier: München, Germany, 2017; ISBN 9783437444975. [Google Scholar]
- Roberts, M.Y.; Kaiser, A.P. Assessing the Effects of a Parent-Implemented Language Intervention for Children with Language Impairments Using Empirical Benchmarks: A Pilot Study. J. Speech Lang. Hear. Res. 2012, 55, 1655–1670. [Google Scholar] [CrossRef]
- Russ, S.A.; Kuo, A.A.; Poulakis, Z.; Barker, M.; Rickards, F.; Saunders, K.; Jarman, F.C.; Wake, M.; Oberklaid, F. Qualitative analysis of parents’ experience with early detection of hearing loss. Arch. Dis. Child. 2004, 89, 353–358. [Google Scholar] [CrossRef]
- Wood Jackson, C.; Turnbull, A. Impact of Deafness on Family Life. Top. Early Child. Spec. Educ. 2004, 24, 15–29. [Google Scholar] [CrossRef]
- Taylor, D.; Le Coz, P. Announcing the diagnosis: Counselling the parents. Handb. Clin. Neurol. 2013, 111, 93–99. [Google Scholar] [CrossRef]
- Watkin, P.M.; Baldwin, M. Confirmation of deafness in infancy. Arch. Dis. Child. 1999, 81, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Young, A.; Tattersall, H. Universal newborn hearing screening and early identification of deafness: Parents’ responses to knowing early and their expectations of child communication development. J. Deaf Stud. Deaf Educ. 2007, 12, 209–220. [Google Scholar] [CrossRef]
- Luterman, D. Counseling the Communicatively Disordered and Their Families, 1st ed.; Little Brown: Boston, 1984; ISBN 9780316537513. [Google Scholar]
- Luterman, D.; Kurtzer-White, E. Identifying Hearing Loss. Am. J. Audiol. 1999, 8, 13–18. [Google Scholar] [CrossRef]
- Eleweke, C.J.; Gilbert, S.; Bays, D.; Austin, E. Information about Support Services for Families of Young Children with Hearing Loss: A Review of Some Useful Outcomes and Challenges. Deaf. Educ. Int. 2008, 10, 190–212. [Google Scholar] [CrossRef]
- Isarin, J.; van Zadelhoff, I.; Wolters-Leermakers, N.; Speksnijder-Bregman, M.; Hannink, M.; Knoors, H. A World of Difference. Parental Perspectives on Cochlear Implantation in Deaf Children with Additional Disabilities. Deaf. Educ. Int. 2015, 17, 219–230. [Google Scholar] [CrossRef]
- Zaidman-Zait, A.; Curle, D.; Jamieson, J.R.; Chia, R.; Kozak, F.K. Cochlear implantation among deaf children with additional disabilities: Parental perceptions of benefits, challenges, and service provision. J. Deaf Stud. Deaf Educ. 2015, 20, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtzer-White, E.; Luterman, D. Families and children with hearing loss: Grief and coping. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Paradis, G.; Koester, L.S. Emotional Availability and Touch in Deaf and Hearing Dyads. Am. Ann. Deaf 2015, 160, 303–315. [Google Scholar] [CrossRef]
- Pipp-Siegel, S.; Biringen, Z. Assessing the quality of relationships between parents and children: The emotional availability scales. Volta Rev. 1998, 100, 237–249. [Google Scholar]
- Papoušek, H.; Bornstein, M. Didactic interactions: Intuitive parental support of vocal and verbal development in human infants. In Nonverbal Vocal Communication: Comparative and Developmental Approaches; Papoušek, H., Jürgens, U., Papoušek, M., Eds.; Cambridge University Press: Cambridge, MA, USA, 1992; pp. 209–229. [Google Scholar]
- Meadow-Orlans, K.P.; Steinberg, A.G. Effects of infant hearing loss and maternal support on mother-infant interactions at 18 months. J. Appl. Dev. Psychol. 1993, 14, 407–426. [Google Scholar] [CrossRef]
- Papoušek, H.; Papoušek, M. Intuitive parenting: A dialectic counterpart to the infant’s integrative competence. In Handbook of Infant Development; Osofsky, D., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 1987; pp. 669–720. [Google Scholar]
- Fitzpatrick, E.; Angus, D.; Durieux-Smith, A.; Graham, I.D.; Coyle, D. Parents’ Needs Following Identification of Childhood Hearing Loss. Am. J. Audiol. 2008, 17, 38–49. [Google Scholar] [CrossRef]
- Lederberg, A.R.; Golbach, T. Parenting stress and social support in hearing mothers of deaf and hearing children: A longitudinal study. J. Deaf Stud. Deaf Educ. 2002, 7, 330–345. [Google Scholar] [CrossRef] [Green Version]
- Kolemen, A.B.; Akyuz, E.; Toprak, A.; Deveci, E.; Yesil, G. Evaluation of The Parents’ Anxiety Levels Before and After the Diagnosis of Their Child with A Rare Genetic Disease: The Necessity of Psychological Support. Orphanet J. Rare Dis. 2021, 16, 402. [Google Scholar] [CrossRef]
- Svinndal, E.V.; Solheim, J.; Rise, M.B.; Jensen, C. Hearing loss and work participation: A cross-sectional study in Norway. Int. J. Audiol. 2018, 57, 646–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limbers, C.A.; Gutierrez, A.; Cohen, L.A. The Patient-Centered Medical Home: Mental Health and Parenting Stress in Mothers of Children with Autism. J. Prim. Care Community Health 2020, 11, 2150132720936067. [Google Scholar] [CrossRef] [PubMed]
- Dorros, C.; Kurtzer-White, E.; Ahlgren, M.; Simon, P.; Vohr, B. Medical home for children with hearing loss: Physician perspectives and practices. Pediatrics 2007, 120, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strickland, B.; McPherson, M.; Weissman, G.; van Dyck, P.; Huang, Z.J.; Newacheck, P. Access to the medical home: Results of the National Survey of Children with Special Health Care Needs. Pediatrics 2004, 113, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- McPherson, M.; Arango, P.; Fox, H.; Lauver, C.; McManus, M.; Newacheck, P.W.; Perrin, J.M.; Shonkoff, J.P.; Strickland, B. A new definition of children with special health care needs. Pediatrics 1998, 102, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Schmulian, D.; Lind, C. Parental experiences of the diagnosis of permanent childhood hearing loss: A phenomenological study. Int. J. Audiol. 2020, 59, 54–60. [Google Scholar] [CrossRef]
- Quittner, A.L.; Glueckauf, R.L.; Jackson, D.N. Chronic parenting stress: Moderating versus mediating effects of social support. J. Pers. Soc. Psychol. 1990, 59, 1266–1278. [Google Scholar] [CrossRef]
- Quittner, A.L.; Steck, J.T.; Rouiller, R.L. Cochlear implants in children: A study of parental stress and adjustment. Am. J. Otol. 1991, 12, 95–104. [Google Scholar]
- Åsberg, K.K.; Vogel, J.J.; Bowers, C.A. Exploring Correlates and Predictors of Stress in Parents of Children Who are Deaf: Implications of Perceived Social Support and Mode of Communication. J. Child. Fam. Stud. 2008, 17, 486–499. [Google Scholar] [CrossRef]
- Quittner, A.L.; Barker, D.H.; Cruz, I.; Snell, C.; Grimley, M.E.; Botteri, M. Parenting Stress among Parents of Deaf and Hearing Children: Associations with Language Delays and Behavior Problems. Parent. Sci. Pract. 2010, 10, 136–155. [Google Scholar] [CrossRef] [Green Version]
- Sarant, J.; Garrard, P. Parenting stress in parents of children with cochlear implants: Relationships among parent stress, child language, and unilateral versus bilateral implants. J. Deaf Stud. Deaf Educ. 2014, 19, 85–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abidin, R.R. Parenting Stress Index: Manual, Administration Booklet, [and] Research Update; Pediatric Psychology Press: Charlottesville, VA, USA, 1983. [Google Scholar]
- Prendergast, S.G.; McCollum, J.A. Let’s talk: The effect of maternal hearing status on interactions with toddlers who are deaf. Am. Ann. Deaf 1996, 141, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Calkins, S.D.; Hungerford, A.; Dedmon, S.E. Mothers’ interactions with temperamentally frustrated infants. Infant Ment. Health J. 2004, 25, 219–239. [Google Scholar] [CrossRef]
- Noel, M.; Peterson, C.; Jesso, B. The relationship of parenting stress and child temperament to language development among economically disadvantaged preschoolers. J. Child Lang. 2008, 35, 823–843. [Google Scholar] [CrossRef] [Green Version]
- Nittrouer, S.; Lowenstein, J.H.; Antonelli, J. Parental Language Input to Children with Hearing Loss: Does It Matter in the End? J. Speech Lang. Hear. Res. 2020, 63, 234–258. [Google Scholar] [CrossRef]
- Quittner, A.L.; Cruz, I.; Barker, D.H.; Tobey, E.; Eisenberg, L.S.; Niparko, J.K. Effects of maternal sensitivity and cognitive and linguistic stimulation on cochlear implant users’ language development over four years. J. Pediatr. 2013, 162, 343–348.e3. [Google Scholar] [CrossRef] [Green Version]
- Blank, A.; Frush Holt, R.; Pisoni, D.B.; Kronenberger, W.G. Associations Between Parenting Stress, Language Comprehension, and Inhibitory Control in Children with Hearing Loss. J. Speech Lang. Hear. Res. 2020, 63, 321–333. [Google Scholar] [CrossRef]
- Cejas, I.; Mitchell, C.M.; Barker, D.H.; Sarangoulis, C.; Eisenberg, L.S.; Quittner, A.L. Parenting Stress, Self-Efficacy, and Involvement: Effects on Spoken Language Ability Three Years After Cochlear Implantation. Otol. Neurotol. 2021, 42, S11–S18. [Google Scholar] [CrossRef]
- Calderon, R.; Greenberg, M.T. Stress and Coping in Hearing Mothers of Children with Hearing Loss: Factors Affecting Mother and Child Adjustment. Am. Ann. Deaf 1999, 144, 7–18. [Google Scholar] [CrossRef]
- Hintermair, M. Parental resources, parental stress, and socioemotional development of deaf and hard of hearing children. J. Deaf Stud. Deaf Educ. 2006, 11, 493–513. [Google Scholar] [CrossRef] [Green Version]
- Topol, D.; Girard, N.; St Pierre, L.; Tucker, R.; Vohr, B. The effects of maternal stress and child language ability on behavioral outcomes of children with congenital hearing loss at 18–24 months. Early Hum. Dev. 2011, 87, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Dirks, E.; Uilenburg, N.; Rieffe, C. Parental stress among parents of toddlers with moderate hearing loss. Res. Dev. Disabil. 2016, 55, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.; Curtin, M.; Botting, N. The interplay between early social interaction, language and executive function development in deaf and hearing infants. Infant Behav. Dev. 2021, 64, 101591. [Google Scholar] [CrossRef] [PubMed]
- Traci, M.; Koester, L. Parent–Infant Interactions: A Transactional Approach to Understanding the Development of Deaf Infants. In The Oxford Handbook of Deaf Studies, Language, and Education; Marschark, M., Spencer, P., Eds.; Oxford University Press: Oxford, UK, 2003; pp. 190–202. [Google Scholar]
- Fagan, M.K.; Bergeson, T.R.; Morris, K.J. Synchrony, complexity and directiveness in mothers’ interactions with infants pre- and post-cochlear implantation. Infant Behav. Dev. 2014, 37, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Holt, R.F.; Beer, J.; Kronenberger, W.G.; Pisoni, D.B.; Lalonde, K. Contribution of Family Environment to Pediatric Cochlear Implant Users’ Speech and Language Outcomes: Some Preliminary Findings. J. Speech Lang. Hear. Res. 2012, 55, 848–864. [Google Scholar] [CrossRef]
- Pressman, L.; Pipp-Siegel, S.; Yoshinaga-Itano, C.; Deas, A. Maternal sensitivity predicts language gain in preschool children who are deaf and hard of hearing. J. Deaf Stud. Deaf Educ. 1999, 4, 294–304. [Google Scholar] [CrossRef]
- Niparko, J.K.; Tobey, E.A.; Thal, D.J.; Eisenberg, L.S.; Wang, N.-Y.; Quittner, A.L.; Fink, N.E. Spoken language development in children following cochlear implantation. JAMA 2010, 303, 1498–1506. [Google Scholar] [CrossRef] [Green Version]
- Isabella, R.A.; Belsky, J. Interactional synchrony and the origins of infant-mother attachment: A replication study. Child Dev. 1991, 62, 373–384. [Google Scholar] [CrossRef]
- Holzinger, D.; Dall, M.; Sanduvete-Chaves, S.; Saldaña, D.; Chacón-Moscoso, S.; Fellinger, J. The Impact of Family Environment on Language Development of Children with Cochlear Implants: A Systematic Review and Meta-Analysis. Ear Hear. 2020, 41, 1077–1091. [Google Scholar] [CrossRef]
- Huttenlocher, J.; Haight, W.; Bryk, A.; Seltzer, M.; Lyons, T. Early vocabulary growth: Relation to language input and gender. Dev. Psychol. 1991, 27, 236–248. [Google Scholar] [CrossRef]
- Hart, B.; Risley, T. Meaningful Differences in the Everyday Experience of Young American Children; Paul H Brookes Publishing: Baltimore, MD, USA, 1995. [Google Scholar]
- DesJardin, J.L.; Eisenberg, L.S. Maternal contributions: Supporting language development in young children with cochlear implants. Ear Hear. 2007, 28, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, S.E.; Walker, E.A.; Unflat-Berry, L.M.; Oleson, J.J.; Moeller, M.P. Quantity and Quality of Caregivers’ Linguistic Input to 18-Month and 3-Year-Old Children Who Are Hard of Hearing. Ear Hear. 2015, 36 (Suppl. S1), 48S–59S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VanDam, M.; Ambrose, S.E.; Moeller, M.P. Quantity of parental language in the home environments of hard-of-hearing 2-year-olds. J. Deaf Stud. Deaf Educ. 2012, 17, 402–420. [Google Scholar] [CrossRef] [PubMed]
- Dirks, E.; Rieffe, C. Are You There for Me? Joint Engagement and Emotional Availability in Parent-Child Interactions for Toddlers with Moderate Hearing Loss. Ear Hear. 2019, 40, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Cruz, I.; Quittner, A.L.; Marker, C.; DesJardin, J.L. Identification of effective strategies to promote language in deaf children with cochlear implants. Child Dev. 2013, 84, 543–559. [Google Scholar] [CrossRef]
- Rowe, M.L. A longitudinal investigation of the role of quantity and quality of child-directed speech in vocabulary development. Child Dev. 2012, 83, 1762–1774. [Google Scholar] [CrossRef]
- Szagun, G.; Stumper, B. Age or Experience? The Influence of Age at Implantation and Social and Linguistic Environment on Language Development in Children with Cochlear Implants. J. Speech Lang. Hear. Res. 2012, 55, 1640–1654. [Google Scholar] [CrossRef] [Green Version]
- Paul, R.; Paatsch, L.; Caselli, N.; Garberoglio, C.L.; Goldin-Meadow, S.; Lederberg, A. Current Research in Pragmatic Language Use Among Deaf and Hard of Hearing Children. Pediatrics 2020, 146, S237–S245. [Google Scholar] [CrossRef]
- Tomasello, M. The social-pragmatic theory of word learning. PRAG 2000, 10, 401–413. [Google Scholar] [CrossRef]
- Bruner, J. The Role of Interaction Formats in Language Acquisition. In Language and Social Situations; Forgas, J.P., Ed.; Springer: New York, NY, USA, 1985; pp. 31–46. ISBN 978-1-4612-9552-5. [Google Scholar]
- Bruner, J.S. From communication to language—A psychological perspective. Cognition 1974, 3, 255–287. [Google Scholar] [CrossRef]
- Law, J.; Rush, R.; Clegg, J.; Peters, T.; Roulstone, S. The role of pragmatics in mediating the relationship between social disadvantage and adolescent behavior. J. Dev. Behav. Pediatr. 2015, 36, 389–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, T.Y.C.; Cupples, L.; Leigh, G.; Hou, S.; Wong, A. Predicting Quality of Life and Behavior and Emotion from Functional Auditory and Pragmatic Language Abilities in 9-Year-Old Deaf and Hard-of-Hearing Children. J. Clin. Med. 2021, 10, 5357. [Google Scholar] [CrossRef] [PubMed]
- Zaidman-Zait, A.; Most, T. Pragmatics and Peer Relationships Among Deaf, Hard of Hearing, and Hearing Adolescents. Pediatrics 2020, 146, S298–S303. [Google Scholar] [CrossRef] [PubMed]
- Dammeyer, J. Psychosocial development in a Danish population of children with cochlear implants and deaf and hard-of-hearing children. J. Deaf Stud. Deaf Educ. 2010, 15, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Fellinger, J.; Holzinger, D.; Pollard, R. Mental health of deaf people. Lancet 2012, 379, 1037–1044. [Google Scholar] [CrossRef]
- Theunissen, S.C.P.M.; Rieffe, C.; Kouwenberg, M.; de Raeve, L.J.I.; Soede, W.; Briaire, J.J.; Frijns, J.H.M. Behavioral problems in school-aged hearing-impaired children: The influence of sociodemographic, linguistic, and medical factors. Eur. Child Adolesc. Psychiatry 2014, 23, 187–196. [Google Scholar] [CrossRef]
- Huber, M. Health-related quality of life of Austrian children and adolescents with cochlear implants. Int. J. Pediatric Otorhinolaryngol. 2005, 69, 1089–1101. [Google Scholar] [CrossRef]
- Bandura, A. Regulation of cognitive processes through perceived self-efficacy. Dev. Psychol. 1989, 25, 729–735. [Google Scholar] [CrossRef]
- Glanemann, R.; Reichmuth, K.; Matulat, P.; am Zehnhoff-Dinnesen, A. Muenster Parental Programme empowers parents in communicating with their infant with hearing loss. Int. J. Pediatric Otorhinolaryngol. 2013, 77, 2023–2029. [Google Scholar] [CrossRef]
- Pepper, J.; Weitzman, E. It Takes Two to Talk: A Practical Guide for Parents of Children with Language Delays; The Hanen Centre: Toronto, ON, Canada, 2004. [Google Scholar]
- Manolson, A. It takes two to talk. In A Parent’s Guide to Helping Children Communicate; Hanen Centre: Toronto, ON, Canada, 1992. [Google Scholar]
- Lam-Cassettari, C.; Wadnerkar-Kamble, M.B.; James, D.M. Enhancing Parent-Child Communication and Parental Self-Esteem with a Video-Feedback Intervention: Outcomes with Prelingual Deaf and Hard-of-Hearing Children. J. Deaf Stud. Deaf Educ. 2015, 20, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Davids, R.S.; Roman, N.V.; Schenck, C.J. Interventions on parenting styles of hearing parents parenting children with a hearing loss: A scoping review. Deaf. Educ. Int. 2018, 20, 41–58. [Google Scholar] [CrossRef]
- Roberts, M.Y. Parent-Implemented Communication Treatment for Infants and Toddlers with Hearing Loss: A Randomized Pilot Trial. J. Speech Lang. Hear. Res. 2019, 62, 143–152. [Google Scholar] [CrossRef] [PubMed]
- DesJardin, J.L. Maternal Perceptions of Self-Efficacy and Involvement in the Auditory Development of Young Children with Prelingual Deafness. J. Early Interv. 2005, 27, 193–209. [Google Scholar] [CrossRef]
- Szarkowski, A.; Dirks, E. Fathers of Young Deaf or Hard-of-Hearing Children: A Systematic Review. J. Deaf Stud. Deaf Educ. 2021, 26, 187–208. [Google Scholar] [CrossRef] [PubMed]
- Dirks, E.; Szarkowski, A. Family-Centered Early Intervention (FCEI) Involving Fathers and Mothers of Children Who Are Deaf or Hard of Hearing: Parental Involvement and Self-Efficacy. J. Clin. Med. 2022, 11, 492. [Google Scholar] [CrossRef]
- Jackson, C.W. Family supports and resources for parents of children who are deaf or hard of hearing. Am. Ann. Deaf 2011, 156, 343–362. [Google Scholar] [CrossRef]
- Henderson, R.J.; Johnson, A.; Moodie, S. Parent-to-parent support for parents with children who are deaf or hard of hearing: A conceptual framework. Am. J. Audiol. 2014, 23, 437–448. [Google Scholar] [CrossRef] [Green Version]
- Gale, E.; Berke, M.; Benedict, B.; Olson, S.; Putz, K.; Yoshinaga-Itano, C. Deaf adults in early intervention programs. Deaf. Educ. Int. 2021, 23, 3–24. [Google Scholar] [CrossRef]
- Gale, E. Collaborating with Deaf Adults in Early Intervention. Young Except. Child. 2021, 24, 225–236. [Google Scholar] [CrossRef]
- Hintermair, M. Hearing impairment, social networks, and coping: The need for families with hearing-impaired children to relate to other parents and to hearing-impaired adults. Am. Ann. Deaf 2000, 145, 41–53. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. American Academy of Pediatrics Ad Hoc Task Force on Definition of the Medical Home: The medical home. Pediatrics 1992, 90, 774. [Google Scholar]
- Farmer, J.E.; Clark, M.J.; Drewel, E.H.; Swenson, T.M.; Ge, B. Consultative care coordination through the medical home for CSHCN: A randomized controlled trial. Matern. Child Health J. 2011, 15, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Golnik, A.; Maccabee-Ryaboy, N.; Scal, P.; Wey, A.; Gaillard, P. Shared decision making: Improving care for children with autism. Intellect. Dev. Disabil. 2012, 50, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Tschudy, M.M.; Toomey, S.L.; Cheng, T.L. Merging systems: Integrating home visitation and the family-centered medical home. Pediatrics 2013, 132 (Suppl. S2), S74–S81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlthau, K.A.; Bloom, S.; van Cleave, J.; Knapp, A.A.; Romm, D.; Klatka, K.; Homer, C.J.; Newacheck, P.W.; Perrin, J.M. Evidence for family-centered care for children with special health care needs: A systematic review. Acad. Pediatr. 2011, 11, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Jackson, G.L.; Powers, B.J.; Chatterjee, R.; Bettger, J.P.; Kemper, A.R.; Hasselblad, V.; Dolor, R.J.; Irvine, R.J.; Heidenfelder, B.L.; Kendrick, A.S.; et al. The patient centered medical home. A systematic review. Ann. Intern. Med. 2013, 158, 169–178. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task Force. Universal screening for hearing loss in newborns: US Preventive Services Task Force recommendation statement. Pediatrics 2008, 122, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Yoshinaga-Itano, C.; Apuzzo, M.L. The development of deaf and hard of hearing children identified early through the high-risk registry. Am. Ann. Deaf 1998, 143, 416–424. [Google Scholar] [CrossRef]
- Holzinger, D.; Fellinger, J.; Beitel, C. Early onset of family centred intervention predicts language outcomes in children with hearing loss. Int. J. Pediatric Otorhinolaryngol. 2011, 75, 256–260. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C. From Screening to Early Identification and Intervention: Discovering Predictors to Successful Outcomes for Children with Significant Hearing Loss. J. Deaf Stud. Deaf Educ. 2003, 8, 11–30. [Google Scholar] [CrossRef] [Green Version]
- DesGeorges, J. Family perceptions of early hearing, detection, and intervention systems: Listening to and learning from families. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Holte, L.; Walker, E.; Oleson, J.; Spratford, M.; Moeller, M.P.; Roush, P.; Ou, H.; Tomblin, J.B. Factors Influencing Follow-Up to Newborn Hearing Screening for Infants Who Are Hard of Hearing. Am. J. Audiol. 2012, 21, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Holzinger, D.; Binder, D.; Raus, D.; Palmisano, G.; Fellinger, J. Development and Implementation of a Low-Cost Tracking System after Newborn Hearing Screening in Upper Austria: Lessons Learned from the Perspective of an Early Intervention Provider. Children 2021, 8, 743. [Google Scholar] [CrossRef] [PubMed]
- Tomblin, J.B.; Harrison, M.; Ambrose, S.E.; Walker, E.A.; Oleson, J.J.; Moeller, M.P. Language Outcomes in Young Children with Mild to Severe Hearing Loss. Ear Hear. 2015, 36 (Suppl. S1), 76S–91S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, T.Y.C.; Dillon, H.; Leigh, G.; Cupples, L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: Summary of 5-year findings and implications. Int. J. Audiol. 2018, 57, S105–S111. [Google Scholar] [CrossRef] [PubMed]
- Dettman, S.J.; Pinder, D.; Briggs, R.J.S.; Dowell, R.C.; Leigh, J.R. Communication development in children who receive the cochlear implant younger than 12 months: Risks versus benefits. Ear Hear. 2007, 28, 11S–18S. [Google Scholar] [CrossRef]
- Walker, E.A.; Spratford, M.; Moeller, M.P.; Oleson, J.; Ou, H.; Roush, P.; Jacobs, S. Predictors of Hearing Aid Use Time in Children with Mild-to-Severe Hearing Loss. LSHSS 2013, 44, 73–88. [Google Scholar] [CrossRef] [Green Version]
- Duchesne, L.; Marschark, M. Effects of Age at Cochlear Implantation on Vocabulary and Grammar: A Review of the Evidence. Am. J. Speech Lang. Pathol. 2019, 28, 1673–1691. [Google Scholar] [CrossRef]
- McCreery, R.W.; Walker, E.A.; Spratford, M.; Bentler, R.; Holte, L.; Roush, P.; Oleson, J.; van Buren, J.; Moeller, M.P. Longitudinal Predictors of Aided Speech Audibility in Infants and Children. Ear Hear. 2015, 36 (Suppl. S1), 24S–37S. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, K.; Preston, E.; Hicken, S. Pediatric hearing aid use: How can audiologists support parents to increase consistency? J. Am. Acad. Audiol. 2014, 25, 380–387. [Google Scholar] [CrossRef]
- Scarinci, N.; Erbasi, E.; Moore, E.; Ching, T.Y.C.; Marnane, V. The parents’ perspective of the early diagnostic period of their child with hearing loss: Information and support. Int. J. Audiol. 2018, 57, S3–S14. [Google Scholar] [CrossRef] [PubMed]
- Archbold, S.M.; Nikolopoulos, T.P.; Lutman, M.E.; O’Donoghue, G.M. The educational settings of profoundly deaf children with cochlear implants compared with age-matched peers with hearing aids: Implications for management. Int. J. Audiol. 2002, 41, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Crowe, K.; Fordham, L.; McLeod, S.; Ching, T.Y.C. “Part of our world”: Influences on caregiver decisions about communication choices for children with hearing loss. Deaf. Educ. Int. 2014, 16, 61–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Bain, L.; Steinberg, A.G. Parental decision making and the choice of communication modality for the child who is deaf. Arch. Pediatr. Adolesc. Med. 2003, 157, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, A.; Bain, L.; Li, Y.; Delgado, G.; Ruperto, V. Decisions Hispanic families make after the identification of deafness. J. Deaf Stud. Deaf Educ. 2003, 8, 291–314. [Google Scholar] [CrossRef] [Green Version]
- Eleweke, C.J.; Rodda, M. Factors contributing to parents’ selection of a communication mode to use with their deaf children. Am. Ann. Deaf 2000, 145, 375–383. [Google Scholar] [CrossRef]
- Decker, K.B.; Vallotton, C.D.; Johnson, H.A. Parents’ communication decision for children with hearing loss: Sources of information and influence. Am. Ann. Deaf 2012, 157, 326–339. [Google Scholar] [CrossRef]
- The Joint Committee on Infant Hearing. Year 2019 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. J. Early Hear. Detect. Interv. 2019, 4, 1–44. [Google Scholar] [CrossRef]
- Moeller, M.P.; Hoover, B.; Peterson, B.; Stelmachowicz, P. Consistency of Hearing Aid Use in Infants with Early-Identified Hearing Loss. Am. J. Audiol. 2009, 18, 14–23. [Google Scholar] [CrossRef]
- Marnane, V.; Ching, T.Y.C. Hearing aid and cochlear implant use in children with hearing loss at three years of age: Predictors of use and predictors of changes in use. Int. J. Audiol. 2015, 54, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Bakar, Z.A.; Brown, P.M.; Remine, M.D. Sensitivity in Interactions between Hearing Mothers and their Toddlers with Hearing Loss: The Effect of Cochlear Implantation. Deaf. Educ. Int. 2010, 12, 2–15. [Google Scholar] [CrossRef]
- Burger, T.; Spahn, C.; Richter, B.; Eissele, S.; Löhle, E.; Bengel, J. Psychic stress and quality of life in parents during decisive phases in the therapy of their hearing-impaired children. Ear Hear. 2006, 27, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Spahn, C.; Richter, B.; Burger, T.; Löhle, E.; Wirsching, M. A comparison between parents of children with cochlear implants and parents of children with hearing aids regarding parental distress and treatment expectations. Int. J. Pediatric Otorhinolaryngol. 2003, 67, 947–955. [Google Scholar] [CrossRef]
- Mitchell, C.O.; Morton, C.C. Genetics of Childhood Hearing Loss. Otolaryngol. Clin. N. Am. 2021, 54, 1081–1092. [Google Scholar] [CrossRef]
- Sun, Y.; Xiang, J.; Liu, Y.; Chen, S.; Yu, J.; Peng, J.; Liu, Z.; Chen, L.; Sun, J.; Yang, Y.; et al. Increased diagnostic yield by reanalysis of data from a hearing loss gene panel. BMC Med. Genom. 2019, 12, 76. [Google Scholar] [CrossRef] [Green Version]
- Downie, L.; Halliday, J.; Burt, R.; Lunke, S.; Lynch, E.; Martyn, M.; Poulakis, Z.; Gaff, C.; Sung, V.; Wake, M.; et al. Exome sequencing in infants with congenital hearing impairment: A population-based cohort study. Eur. J. Hum. Genet. 2020, 28, 587–596. [Google Scholar] [CrossRef]
- Gooch, C.; Rudy, N.; Smith, R.J.; Robin, N.H. Genetic testing hearing loss: The challenge of non syndromic mimics. Int. J. Pediatric Otorhinolaryngol. 2021, 150, 110872. [Google Scholar] [CrossRef]
- Whatley, M.; Francis, A.; Ng, Z.Y.; Khoh, X.E.; Atlas, M.D.; Dilley, R.J.; Wong, E.Y.M. Usher Syndrome: Genetics and Molecular Links of Hearing Loss and Directions for Therapy. Front. Genet. 2020, 11, 565216. [Google Scholar] [CrossRef]
- Notini, L.; Gaff, C.L.; Savulescu, J.; Vears, D.F. Clinicians’ Views and Experiences with Offering and Returning Results from Exome Sequencing to Parents of Infants with Hearing Loss. J. Clin. Med. 2021, 11, 35. [Google Scholar] [CrossRef]
- Lanphear, B.P. The impact of toxins on the developing brain. Annu. Rev. Public Health 2015, 36, 211–230. [Google Scholar] [CrossRef] [Green Version]
- Irwin, L.; Siddiq, A.; Hertzman, C. Early Childhood Development: A powerful Equalizer: Final Report; World Health Organization: Geneva, Switzerland, 2007.
- Michaelson, V.; Pilato, K.A.; Davison, C.M. Family as a health promotion setting: A scoping review of conceptual models of the health-promoting family. PLoS ONE 2021, 16, e0249707. [Google Scholar] [CrossRef] [PubMed]
- Blackman, J.A.; Gurka, M.J.; Gurka, K.K.; Oliver, M.N. Emotional, developmental and behavioural co-morbidities of children with chronic health conditions. J. Paediatr. Child Health 2011, 47, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Reilly, C.; Agnew, R.; Neville, B.G.R. Depression and anxiety in childhood epilepsy: A review. Seizure 2011, 20, 589–597. [Google Scholar] [CrossRef] [Green Version]
- Dellve, L.; Samuelsson, L.; Tallborn, A.; Fasth, A.; Hallberg, L.R.-M. Stress and well-being among parents of children with rare diseases: A prospective intervention study. J. Adv. Nurs. 2006, 53, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Canam, C. Common adaptive tasks facing parents of children with chronic conditions. J. Adv. Nurs. 1993, 18, 46–53. [Google Scholar] [CrossRef] [PubMed]
- McCreery, R.W.; Bentler, R.A.; Roush, P.A. Characteristics of hearing aid fittings in infants and young children. Ear Hear. 2013, 34, 701–710. [Google Scholar] [CrossRef] [Green Version]
- Baruah, P.; Hanvey, K.; Irving, R.; Tzifa, K. Impact of Chronic Suppurative Otitis Media in Pediatric Cochlear Implant Recipients-Insight into the Challenges from a Tertiary Referral Center in UK. Otol. Neurotol. 2017, 38, 672–677. [Google Scholar] [CrossRef]
- Sakkalou, E.; O’Reilly, M.A.; Sakki, H.; Springall, C.; de Haan, M.; Salt, A.T.; Dale, N.J. Mother-infant interactions with infants with congenital visual impairment and associations with longitudinal outcomes in cognition and language. J. Child Psychol. Psychiatry 2021, 62, 742–750. [Google Scholar] [CrossRef]
- Jackson, D.C.; Jones, J.E.; Hsu, D.A.; Stafstrom, C.E.; Lin, J.J.; Almane, D.; Koehn, M.A.; Seidenberg, M.; Hermann, B.P. Language function in childhood idiopathic epilepsy syndromes. Brain Lang. 2019, 193, 4–9. [Google Scholar] [CrossRef]
- Boettcher, J.; Boettcher, M.; Wiegand-Grefe, S.; Zapf, H. Being the Pillar for Children with Rare Diseases-A Systematic Review on Parental Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 4993. [Google Scholar] [CrossRef]
- Cohen, E.; Kuo, D.Z.; Agrawal, R.; Berry, J.G.; Bhagat, S.K.M.; Simon, T.D.; Srivastava, R. Children with medical complexity: An emerging population for clinical and research initiatives. Pediatrics 2011, 127, 529–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valicenti-McDermott, M.; Lawson, K.; Hottinger, K.; Seijo, R.; Schechtman, M.; Shulman, L.; Shinnar, S. Parental Stress in Families of Children With Autism and Other Developmental Disabilities. J. Child Neurol. 2015, 30, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Cupples, L.; Ching, T.Y.C.; Crowe, K.; Seeto, M.; Leigh, G.; Street, L.; Day, J.; Marnane, V.; Thomson, J. Outcomes of 3-year-old children with hearing loss and different types of additional disabilities. J. Deaf Stud. Deaf Educ. 2014, 19, 20–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindblad, B.-M.; Rasmussen, B.H.; Sandman, P.-O. Being invigorated in parenthood: Parents’ experiences of being supported by professionals when having a disabled child. J. Pediatr. Nurs. 2005, 20, 288–297. [Google Scholar] [CrossRef]
- Hands & Voices. Welcome to Hands & Voices Fostering Joy for Families! Available online: https://www.handsandvoices.org/resources/fostering-joy.htm (accessed on 1 February 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzinger, D.; Hofer, J.; Dall, M.; Fellinger, J. Multidimensional Family-Centred Early Intervention in Children with Hearing Loss: A Conceptual Model. J. Clin. Med. 2022, 11, 1548. https://doi.org/10.3390/jcm11061548
Holzinger D, Hofer J, Dall M, Fellinger J. Multidimensional Family-Centred Early Intervention in Children with Hearing Loss: A Conceptual Model. Journal of Clinical Medicine. 2022; 11(6):1548. https://doi.org/10.3390/jcm11061548
Chicago/Turabian StyleHolzinger, Daniel, Johannes Hofer, Magdalena Dall, and Johannes Fellinger. 2022. "Multidimensional Family-Centred Early Intervention in Children with Hearing Loss: A Conceptual Model" Journal of Clinical Medicine 11, no. 6: 1548. https://doi.org/10.3390/jcm11061548