
Activation of the Carboxypeptidase U (CPU, TAFIa, CPB2) System in Patients with SARS-CoV-2 Infection Could Contribute to COVID-19 Hypofibrinolytic State and Disease Severity Prognosis

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Collection and Biochemical Analyses
2.3. Statistical Analysis
3. Results and Discussion
3.1. Patient Characteristics
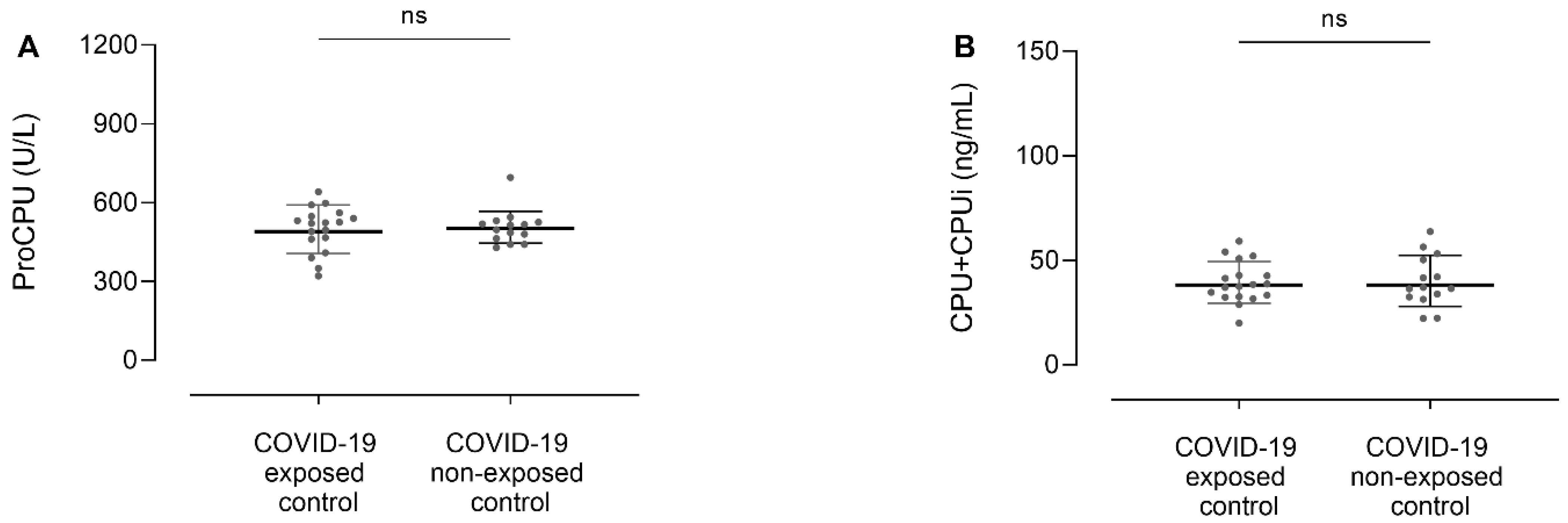
3.2. ProCPU and CPU+CPUi Antigen Levels Do Not Differ between COVID-19 Exposed and Non-Exposed Controls
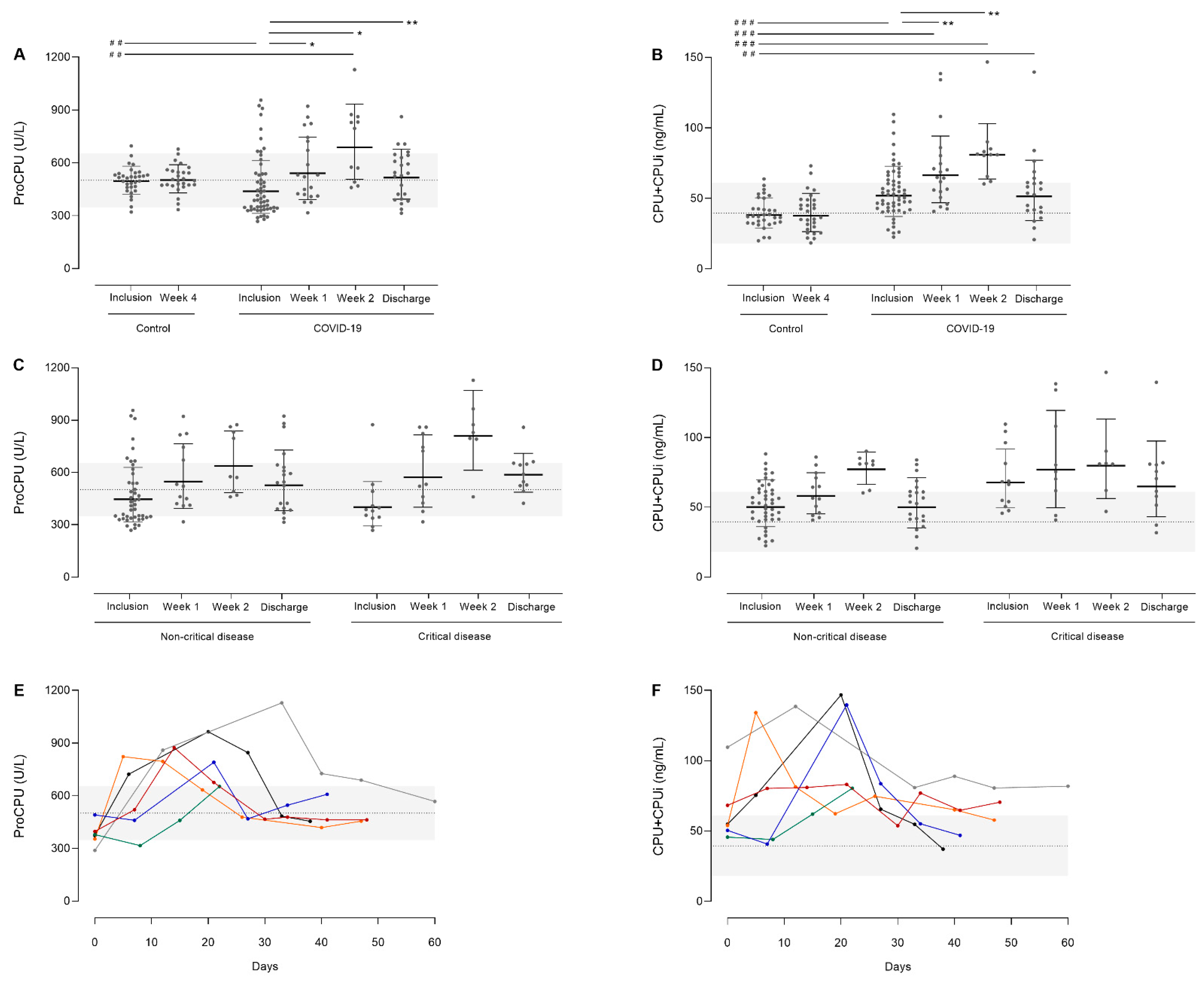
3.3. ProCPU Consumption with Concomitant CPU Generation in COVID-19 Patients upon Hospital Admission
3.4. Time Course of CPU-Related Parameters
3.4.1. Total Study Population
3.4.2. Critical versus Non-Critical Disease
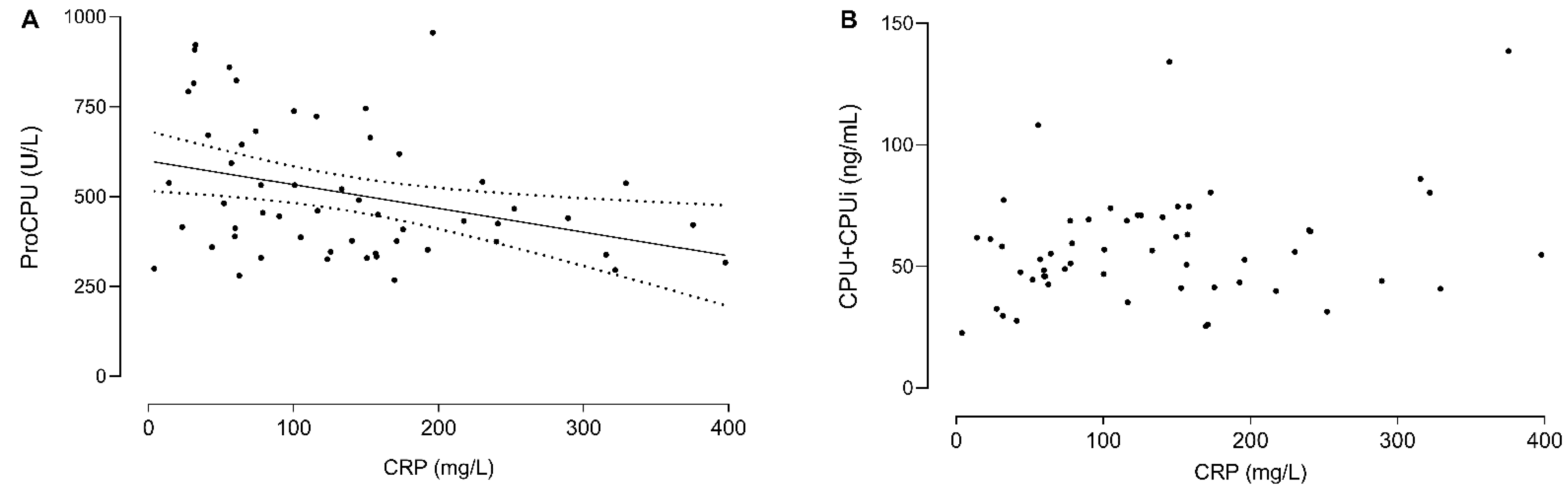
3.5. C-Reactive Protein (CRP) Levels Correlate with the Decrease in ProCPU Levels Early after Disease Onset
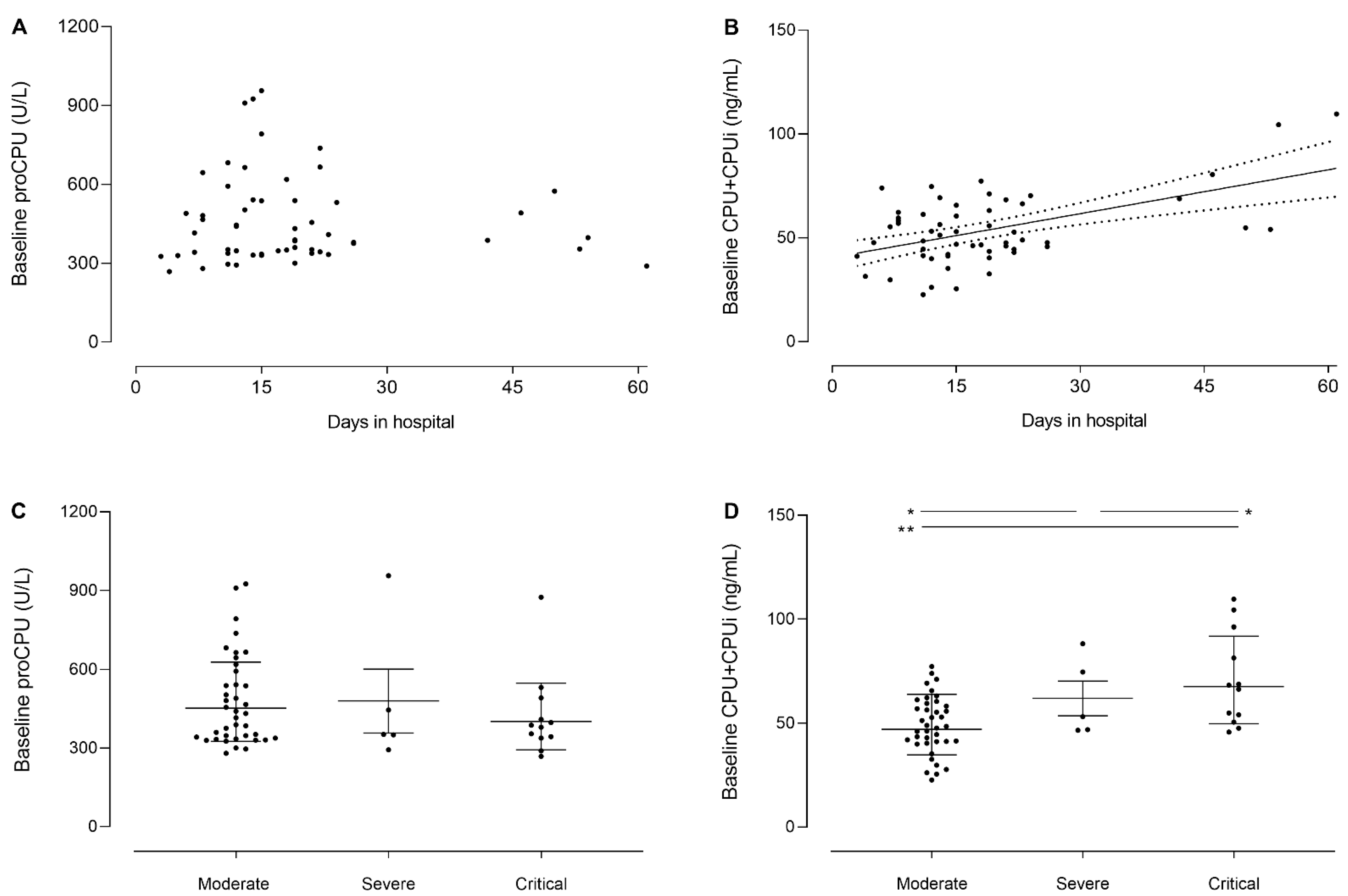
3.6. Baseline CPU+CPUi Antigen Levels Correlate with Disease Severity and the Duration of Hospitalization
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus (COVID-19). Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 27 December 2021).
- Wiersinga, W.; Rhodes, A.; Cheng, A.; Peacock, S.; Prescott, H. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Nougier, C.; Benoit, R.; Simon, M.; Desmurs-Clavel, H.; Marcotte, G.; Argaud, L.; David, J.S.; Bonnet, A.; Negrier, C.; Dargaud, Y. Hypofibrinolytic state and high thrombin generation may play a major role in SARS-COV2 associated thrombosis. J. Thromb. Haemost. 2020, 18, 2215–2219. [Google Scholar] [CrossRef]
- Seheult, J.N.; Seshadri, A.; Neal, M.D. Fibrinolysis Shutdown and Thrombosis in Severe COVID-19. J. Am. Coll. Surg. 2020, 231, 203–204. [Google Scholar] [CrossRef]
- Wright, F.L.; Vogler, T.O.; Moore, E.E.; Moore, H.B.; Wohlauer, M.V.; Urban, S.; Nydam, T.L.; Moore, P.K.; McIntyre, R.C. Fibrinolysis Shutdown Correlation with Thromboembolic Events in Severe COVID-19 Infection. J. Am. Coll. Surg. 2020, 231, 193–203.e1. [Google Scholar] [CrossRef]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.; Li, L.; Liu, X.; Zhu, C. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef] [Green Version]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Zuo, Y.; Warnock, M.; Harbaugh, A.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Knight, J.S.; Kanthi, Y.; Lawrence, D.A. Plasma tissue plasminogen activator and plasminogen activator inhibitor-1 in hospitalized COVID-19 patients. Sci. Rep. 2021, 11, 1580. [Google Scholar] [CrossRef]
- Della-Morte, D.; Pacifici, F.; Ricordi, C.; Massoud, R.; Rovella, V.; Proietti, S.; Iozzo, M.; Lauro, D.; Bernardini, S.; Bonassi, S.; et al. Low level of plasminogen increases risk for mortality in COVID-19 patients. Cell Death Dis. 2021, 12, 773. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Hendriks, D.; Wang, W.; Scharpé, S.; Lommaert, M.P.; van Sande, M. Purification and characterization of a new arginine carboxypeptidase in human serum. BBA Gen. Subj. 1990, 1034, 86–92. [Google Scholar] [CrossRef]
- Claesen, K.; Mertens, J.C.; Leenaerts, D.; Hendriks, D. Carboxypeptidase U (CPU, TAFIa, CPB2) in thromboembolic disease: What do we know three decades after its discovery? Int. J. Mol. Sci. 2021, 22, 883. [Google Scholar] [CrossRef]
- Plug, T.; Meijers, J.C.M. Structure-function relationships in thrombin-activatable fibrinolysis inhibitor. J. Thromb. Haemost. 2016, 14, 633–644. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Immune Repertoire Sequencing-NCT04368143-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04368143 (accessed on 8 October 2021).
- Heylen, E.; Van Goethem, S.; Willemse, J.; Olsson, T.; Augustyns, K.; Hendriks, D. Development of a sensitive and selective assay for the determination of procarboxypeptidase U (thrombin-activatable fibrinolysis inhibitor) in plasma. Anal. Biochem. 2010, 396, 152–154. [Google Scholar] [CrossRef]
- Mertens, J.C.; Claesen, K.; Leenaerts, D.; Sim, Y.; Lambeir, A.M.; Hendriks, D. Inhibition of the procarboxypeptidase U (proCPU, TAFI, proCPB2) system due to hemolysis. J. Thromb. Haemost. 2019, 17, 878–884. [Google Scholar] [CrossRef]
- Juneja, G.K.; Castelo, M.; Yeh, C.H.; Cerroni, S.E.; Hansen, B.E.; Chessum, J.E.; Abraham, J.; Cani, E.; Dwivedi, D.J.; Fraser, D.D.; et al. Biomarkers of coagulation, endothelial function, and fibrinolysis in critically ill patients with COVID-19: A single-center prospective longitudinal study. J. Thromb. Haemost. 2021, 19, 1546–1557. [Google Scholar] [CrossRef]
- Emonts, M.; De Bruijne, E.L.E.; Guimarães, A.H.C.; Declerck, P.J.; Leebeek, F.W.G.; De Maat, M.P.M.; Rijken, D.C.; Hazelzet, J.A.; Gils, A. Thrombin activatable fibrinolysis inhibitor is associated with severity and outcome of severe meningococcal infection in children. J. Thromb. Haemost. 2008, 6, 268–276. [Google Scholar] [CrossRef]
- Vollrath, J.T.; Marzi, I.; Herminghaus, A.; Lustenberger, T.; Relja, B. Post-traumatic sepsis is associated with increased c5a and decreased TAFI levels. J. Clin. Med. 2020, 9, 1230. [Google Scholar] [CrossRef]
- Zeerleder, S.; Schroeder, V.; Hack, C.E.; Kohler, H.P.; Wuillemin, W.A. TAFI and PAI-1 levels in human sepsis. Thromb. Res. 2006, 118, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Relja, B.; Lustenberger, T.; Puttkammer, B.; Jakob, H.; Morser, J.; Gabazza, E.C.; Takei, Y.; Marzi, I. Thrombin-activatable fibrinolysis inhibitor (TAFI) is enhanced in major trauma patients without infectious complications. Immunobiology 2013, 218, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Bouck, E.G.; Denorme, F.; Holle, L.A.; Middelton, E.A.; Blair, A.M.; De Laat, B.; Schiffman, J.D.; Yost, C.C.; Rondina, M.T.; Wolberg, A.S.; et al. COVID-19 and Sepsis Are Associated with Different Abnormalities in Plasma Procoagulant and Fibrinolytic Activity. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 401–414. [Google Scholar] [CrossRef]
- Park, R.; Song, J.; An, S.S.A. Elevated levels of activated and inactivated thrombin-activatable fibrinolysis inhibitor in patients with sepsis. Korean J. Hematol. 2010, 45, 264. [Google Scholar] [CrossRef] [Green Version]
- Semeraro, F.; Colucci, M.; Caironi, P.; Masson, S.; Ammollo, C.T.; Teli, R.; Semeraro, N.; Magnoli, M.; Salati, G.; Isetta, M.; et al. Platelet drop and fibrinolytic shutdown in patients with sepsis. Crit. Care Med. 2018, 46, E221–E228. [Google Scholar] [CrossRef]
- Totoki, T.; Ito, T.; Kakuuchi, M.; Yashima, N.; Maruyama, I.; Kakihana, Y. An evaluation of circulating activated TAFI in septic DIC: A case series and review of the literature. Thromb. J. 2022, 20, 6–10. [Google Scholar] [CrossRef]
- Komnenov, D.; Scipione, C.A.; Bazzi, Z.A.; Garabon, J.J.W.; Koschinsky, M.L.; Boffa, M.B. Pro-inflammatory cytokines reduce human TAFI expression via tristetraprolin-mediated mRNA destabilisation and decreased binding of HuR. Thromb. Haemost. 2015, 114, 337–349. [Google Scholar] [CrossRef]
- Boffa, M.B.; Hamill, J.D.; Maret, D.; Brown, D.; Scott, M.L.; Nesheim, M.E.; Koschinsky, M.L. Acute phase mediators modulate thrombin-activable fibrinolysis inhibitor (TAFI) gene expression in HepG2 cells. J. Biol. Chem. 2003, 278, 9250–9257. [Google Scholar] [CrossRef] [Green Version]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef]
- Jenner, W.J.; Gorog, D.A. Incidence of thrombotic complications in COVID-19: On behalf of ICODE: The International COVID-19 Thrombosis Biomarkers Colloquium. J. Thromb. Thrombolysis 2021, 52, 999–1006. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | ||
| Age—years (range) | 58 (29–84) | |
| Sex | ||
| Male—N (%) | 38 (68%) | |
| Female—N (%) | 18 (32%) | |
| Baseline Clinical Parameters | ||
| Comorbidities | ||
| Obesity | 13 (22%) | |
| Diabetes | 9 (16%) | |
| Chronic respiratory disease | 10 (17%) | |
| Cardiovascular disease | 10 (17%) | |
| Cancer | 6 (10%) | |
| SpO2 at admission (%) | 96 ± 4 | |
| WHO severity classification | ||
| Moderate | 39 (70%) | |
| Severe | 5 (9%) | |
| Critical | 12 (21%) | |
| Laboratory Parameters | Reference Value | |
| Platelet count (×109/L) | 181 ± 79 | 166–396 |
| WBC (×109/L) | 8.6 ± 6.0 | 4.2–10.3 |
| CRP (mg/L) | 94 ± 125 | <10 |
| Hospital Care | ||
| Medication use | ||
| Antibiotics | 36 (62%) | |
| Antivirals | 4 (7%) | |
| Antifungals | 1 (2%) | |
| Steroids | 25 (43%) | |
| Vasoactive medications | 7 (12%) | |
| Antiplatelet agent | 2 (3%) | |
| Anticoagulation | 8 (14%) | |
| Respiratory status | ||
| Room air | 6 (10%) | |
| High-flow nasal oxygen | 44 (76%) | |
| Invasive ventilation | 7 (12%) | |
| Extracorporeal life support | 1 (2%) | |
| Outcome | ||
| ICU stay | 9 (16%) | |
| Days in hospital | 19 ± 6 | |
| In-hospital death | 4 (7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claesen, K.; Sim, Y.; Bracke, A.; De bruyn, M.; De Hert, E.; Vliegen, G.; Hotterbeekx, A.; Vujkovic, A.; van Petersen, L.; De Winter, F.H.R.; et al. Activation of the Carboxypeptidase U (CPU, TAFIa, CPB2) System in Patients with SARS-CoV-2 Infection Could Contribute to COVID-19 Hypofibrinolytic State and Disease Severity Prognosis. J. Clin. Med. 2022, 11, 1494. https://doi.org/10.3390/jcm11061494
Claesen K, Sim Y, Bracke A, De bruyn M, De Hert E, Vliegen G, Hotterbeekx A, Vujkovic A, van Petersen L, De Winter FHR, et al. Activation of the Carboxypeptidase U (CPU, TAFIa, CPB2) System in Patients with SARS-CoV-2 Infection Could Contribute to COVID-19 Hypofibrinolytic State and Disease Severity Prognosis. Journal of Clinical Medicine. 2022; 11(6):1494. https://doi.org/10.3390/jcm11061494
Chicago/Turabian StyleClaesen, Karen, Yani Sim, An Bracke, Michelle De bruyn, Emilie De Hert, Gwendolyn Vliegen, An Hotterbeekx, Alexandra Vujkovic, Lida van Petersen, Fien H. R. De Winter, and et al. 2022. "Activation of the Carboxypeptidase U (CPU, TAFIa, CPB2) System in Patients with SARS-CoV-2 Infection Could Contribute to COVID-19 Hypofibrinolytic State and Disease Severity Prognosis" Journal of Clinical Medicine 11, no. 6: 1494. https://doi.org/10.3390/jcm11061494