
Assessment of Non-Invasive Measurements of Oxygen Saturation and Heart Rate with an Apple Smartwatch: Comparison with a Standard Pulse Oximeter

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
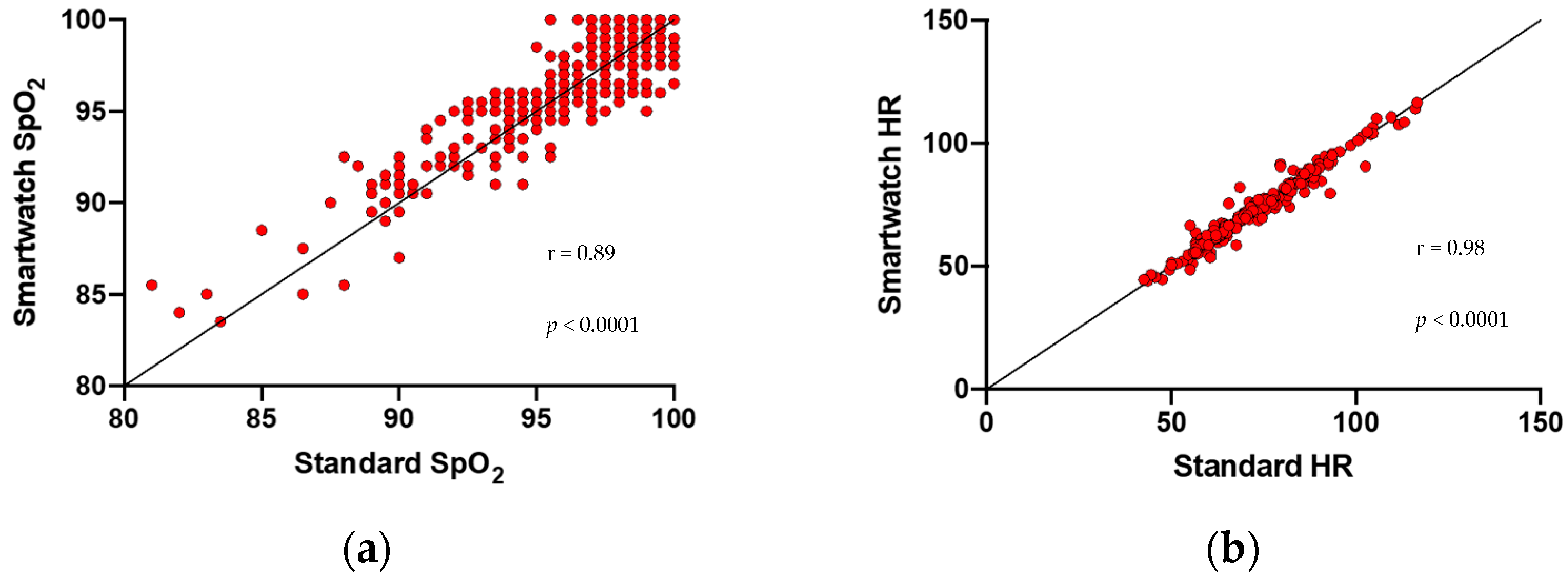
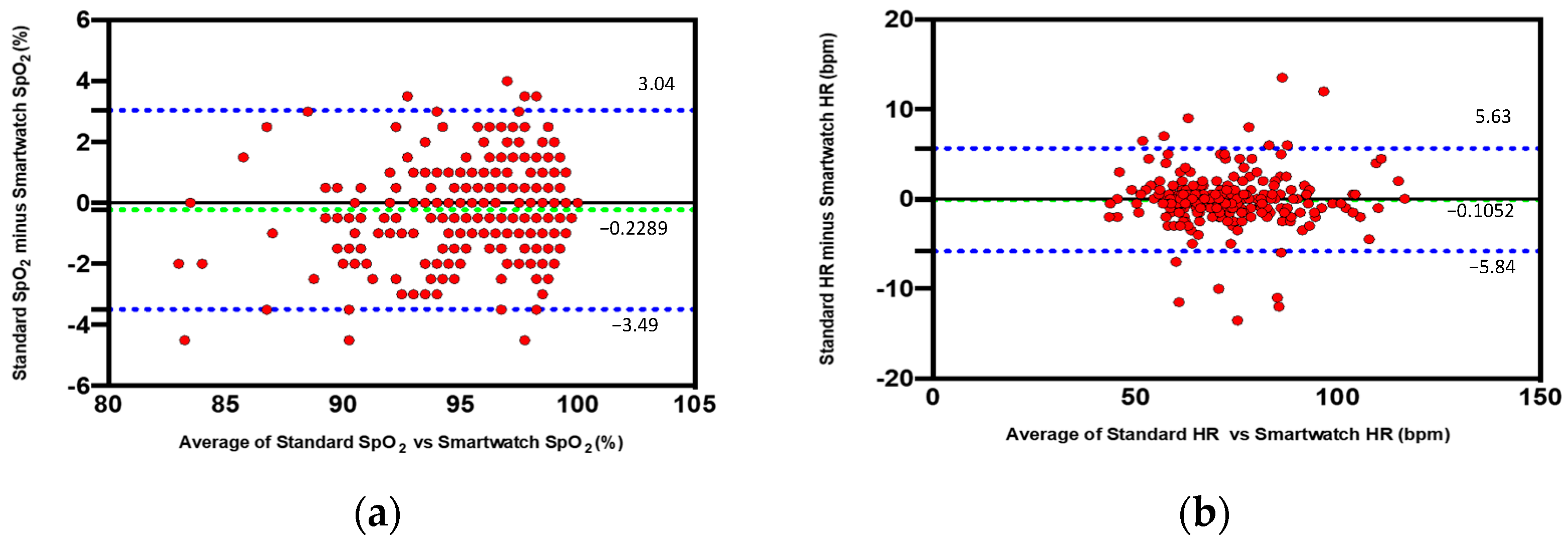
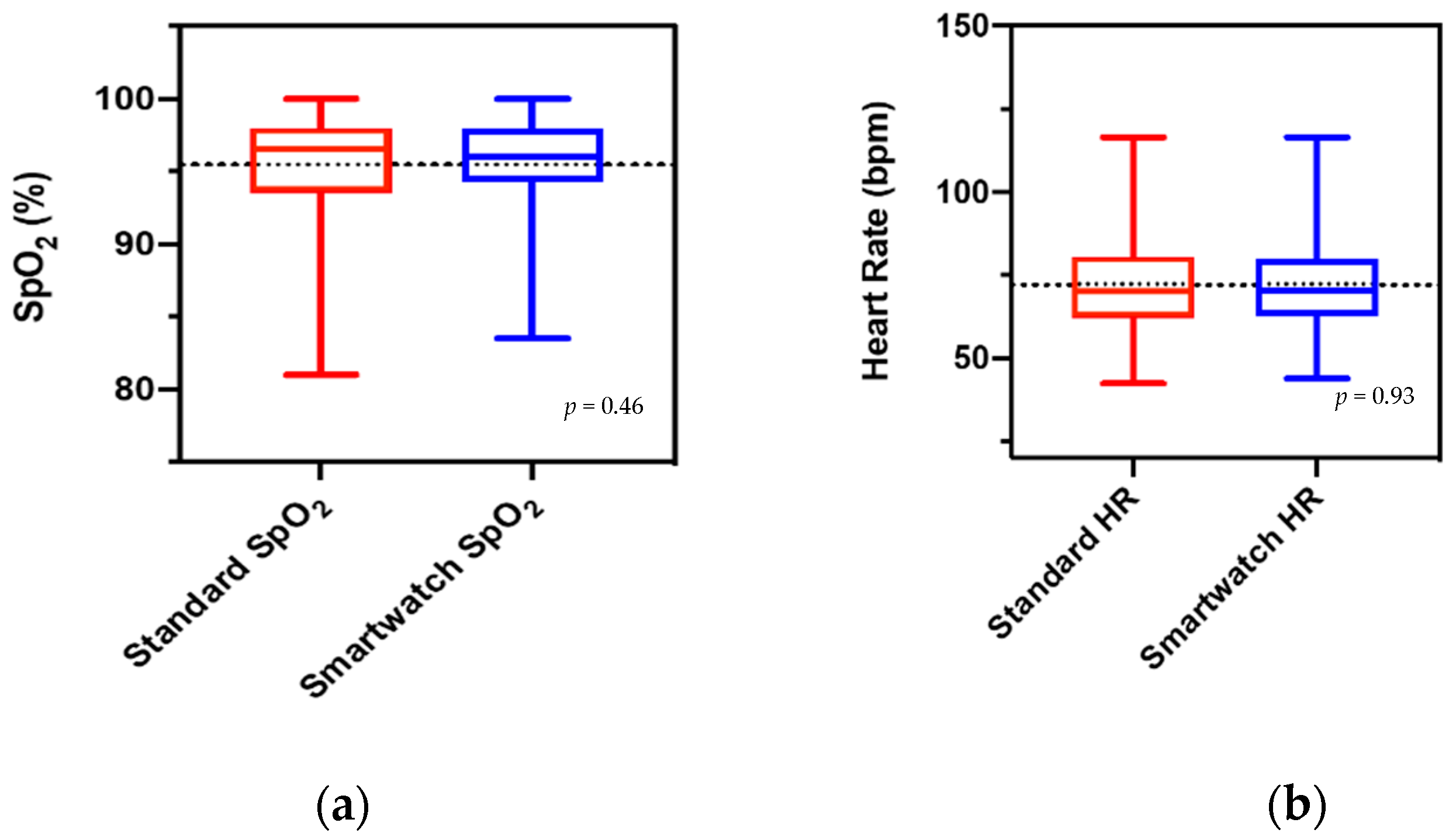
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse oximetry: Understanding its basic principles facilitates appreciation of its limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHS England. Specialty Guides for Patient Management during the Coronavirus Pandemic: Guidance for the Role and Use of Non-Invasive Respiratory Support in Adult Patients with Coronavirus (Confirmed or Suspected). Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/CLEARED_Specialty-guide_-NIV-respiratory-support-and-coronavirus-v2-26-March-003.pdf (accessed on 26 January 2022).
- Apple.com. Available online: https://www.apple.com/Apple-Watch-Series-6/ (accessed on 26 January 2022).
- Tison, G.; Sanchez, J.M.; Ballinger, B.; Singh, A.; Olgin, J.E.; Pletcher, M.J.; Vittinghoff, E.; Lee, E.S.; Fan, S.M.; Gladstone, R.A.; et al. Passive Detection of Atrial Fibrillation Using a Commercially Available Smartwatch. JAMA Cardiol. 2018, 3, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bumgarner, J.M.; Lambert, C.T.; Hussein, A.A.; Cantillon, D.J.; Baranowski, B.; Wolski, K.; Lindsay, B.D.; Wazni, O.M.; Tarakji, K.G. Smartwatch Algorithm for Automated Detection of Atrial Fibrillation. J. Am. Coll. Cardiol. 2018, 71, 2381–2388. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; Balasubramanian, V.; Russo, A.M.; Rajmane, A.; Cheung, L.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N. Engl. J. Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Spaccarotella, C.A.M.; Polimeni, A.; Migliarino, S.; Principe, E.; Curcio, A.; Mongiardo, A.; Sorrentino, S.; De Rosa, S.; Indolfi, C. Multichannel Electrocardiograms Obtained by a Smartwatch for the Diagnosis of ST-Segment Changes. JAMA Cardiol. 2020, 5, 1176–1180. [Google Scholar] [CrossRef] [PubMed]
- Spaccarotella, C.A.M.; Migliarino, S.; Mongiardo, A.; Sabatino, J.; Santarpia, G.; De Rosa, S.; Curcio, A.; Indolfi, C. Measurement of the QT interval using the Apple Watch. Sci. Rep. 2021, 11, 10817. [Google Scholar] [CrossRef] [PubMed]
- Strik, M.; Caillol, T.; Ramirez, F.D.; Abu-Alrub, S.; Marchand, H.; Welte, N.; Ritter, P.; Haïssaguerre, M.; Ploux, S.; Bordachar, P. Validating QT-Interval Measurement Using the Apple Watch ECG to Enable Remote Monitoring During the COVID-19 Pandemic. Circulation 2020, 142, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Spaccarotella, C.; Santarpia, G.; Curcio, A.; Indolfi, C. The smartwatch detects ECG abnormalities typical of Brugada syndrome. J. Cardiovasc. Med. 2021, 22, e24–e25. [Google Scholar] [CrossRef] [PubMed]
- Medtronic.com. Available online: https://www.medtronic.com/content/dam/covidien/library/us/en/product/pulse-oximetry/nellcor-portable-spo2-patient-monitoring-system-sell-sheet.pdf (accessed on 26 January 2022).
- Modi, A.M.; Kiourkas, R.D.; Li, J.; Scott, J.B. Reliability of Smartphone Pulse Oximetry in Subjects at Risk for Hypoxemia. Respir. Care 2021, 66, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Tang, W.; Chen, G.; Lu, Y.; Feng, C.; Tu, X.M. Correlation and agreement: Overview and clarification of competing concepts and measures. Shanghai Arch. Psychiatry 2016, 28, 115–120. [Google Scholar] [PubMed]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Macworld.co.uk. Available online: https://www.macworld.co.uk/news/how-many-apple-watches-sold-3801687/ (accessed on 26 January 2022).
- Pipek, L.Z.; Nascimento, R.F.V.; Acencio, M.M.P.; Teixeira, L.R. Comparison of SpO2 and heart rate values on Apple Watch and conventional commercial oximeters devices in patients with lung disease. Sci. Rep. 2021, 11, 18901. [Google Scholar] [CrossRef] [PubMed]
- Luks, A.M.; Swenson, E.R. Pulse Oximetry for Monitoring Patients with COVID-19 at Home. Potential Pitfalls and Practical Guidance. Ann. Am. Thorac. Soc. 2020, 17, 1040–1046. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Healthy Subjects (n = 56) | Lung Disease (n = 60) | CV Disease (n = 141) | p | |
|---|---|---|---|---|
| Age, y ± SD | 43.18 ± 14.31 | 71.23 ± 10.44 | 69.21 ± 11.53 | <0.001 |
| Male, n (%) | 24 (42.9) | 45 (75) | 99 (70.2) | <0.001 |
| Weight, n ± SD | 69.52 ± 12.15 | 77.59 ± 17.35 | 76.22 ± 15.08 | <0.02 |
| Height, n ± SD | 168.30 ± 9.05 | 166.47 ± 7.37 | 165.51 ± 7.93 | 0.25 |
| BMI, n ± SD | 24.49 ± 3.64 | 27.90 ± 5.41 | 27.71 ± 4.50 | <0.02 |
| Hypertension, n (%) | 10 (17.9) | 52 (86.7) | 126 (89.4) | <0.001 |
| Diabetes mellitus, n (%) | 4 (7.1) | 21 (35) | 47 (33.3) | <0.001 |
| Dyslipidemia, n (%) | 7 (12.5) | 29 (48.3) | 123 (87.2) | <0.001 |
| ACS, n (%) | 0 (0) | 1 (1.7) | 50 (35.5) | <0.001 |
| CCS, n (%) | 0 (0) | 9 (15) | 64 (45.4) | <0.001 |
| Stroke/TIA, n (%) | 0 (0) | 3 (5) | 6 (4.3) | <0.001 |
| Smoke, n (%) | 15 (26.8) | 6 (10.0) | 22 (15.6) | <0.001 |
| COPD, n (%) | 0 (0) | 35 (58.3) | 16 (11.3) | <0.001 |
| OSAS, n (%) | 0 (0) | 16 (26.7) | 10 (7.1) | <0.001 |
| O2 therapy, n (%) | 0 (0) | 24 (40.0) | 18 (12.8) | <0.001 |
| Room temperature, n ± SD | 21.79 ± 1.32 | 21.28 ± 0.55 | 21.32 ± 0.91 | 0.94 |
| Body temperature, n ± SD | 36.18 ± 0.36 | 36.20 ± 0.38 | 36.14 ± 0.40 | 0.98 |
| Wrist circumference, n ± SD | 16.15 ± 1.38 | 16.94 ± 1.15 | 17.03 ± 1.39 | 0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spaccarotella, C.; Polimeni, A.; Mancuso, C.; Pelaia, G.; Esposito, G.; Indolfi, C. Assessment of Non-Invasive Measurements of Oxygen Saturation and Heart Rate with an Apple Smartwatch: Comparison with a Standard Pulse Oximeter. J. Clin. Med. 2022, 11, 1467. https://doi.org/10.3390/jcm11061467
Spaccarotella C, Polimeni A, Mancuso C, Pelaia G, Esposito G, Indolfi C. Assessment of Non-Invasive Measurements of Oxygen Saturation and Heart Rate with an Apple Smartwatch: Comparison with a Standard Pulse Oximeter. Journal of Clinical Medicine. 2022; 11(6):1467. https://doi.org/10.3390/jcm11061467
Chicago/Turabian StyleSpaccarotella, Carmen, Alberto Polimeni, Cinzia Mancuso, Girolamo Pelaia, Giovanni Esposito, and Ciro Indolfi. 2022. "Assessment of Non-Invasive Measurements of Oxygen Saturation and Heart Rate with an Apple Smartwatch: Comparison with a Standard Pulse Oximeter" Journal of Clinical Medicine 11, no. 6: 1467. https://doi.org/10.3390/jcm11061467