
Toward Optimal Learning of the Gesture in Laparoscopic Surgery: Methodology and Performance


 , , ,
, , , 
Abstract
:1. Introduction
2. Surgery Evaluation Criteria
2.1. Gesture Learning
- Cognitive stage: The first stage is the acquisition of the basic gestural technique.
- Contextual stage: The second stage is the acquisition of basic or advanced techniques in a situation, on a mechanical or animal model, by specialty. The basic gestures being acquired, it is a question of now restoring this gesture in its environment. Each manipulation is evaluated by a specific score in order to develop a performance score. The performance score includes the gesture scores (measured by the MoCap system) and a suture one (evaluated on a specific score established by the vascular laparoscopic expert).
- Operational stage: The third stage is the acquisition of operative surgical strategies, by the transmission of traps and operative solutions.
- Feedback stage: The fourth stage is the transmission of the acquired knowledge.
2.2. Augmented Reality and Surgical Learning
3. Emotions and Surgical Learning
3.1. Epistemic Emotions and Confusion
3.2. Self-Efficacy
4. Materials and Methods
4.1. Population
4.1.1. Experimental Design
4.1.2. Hypothesis
4.2. Protocol
4.3. Work Environment
4.3.1. Self-Efficacy Instructions
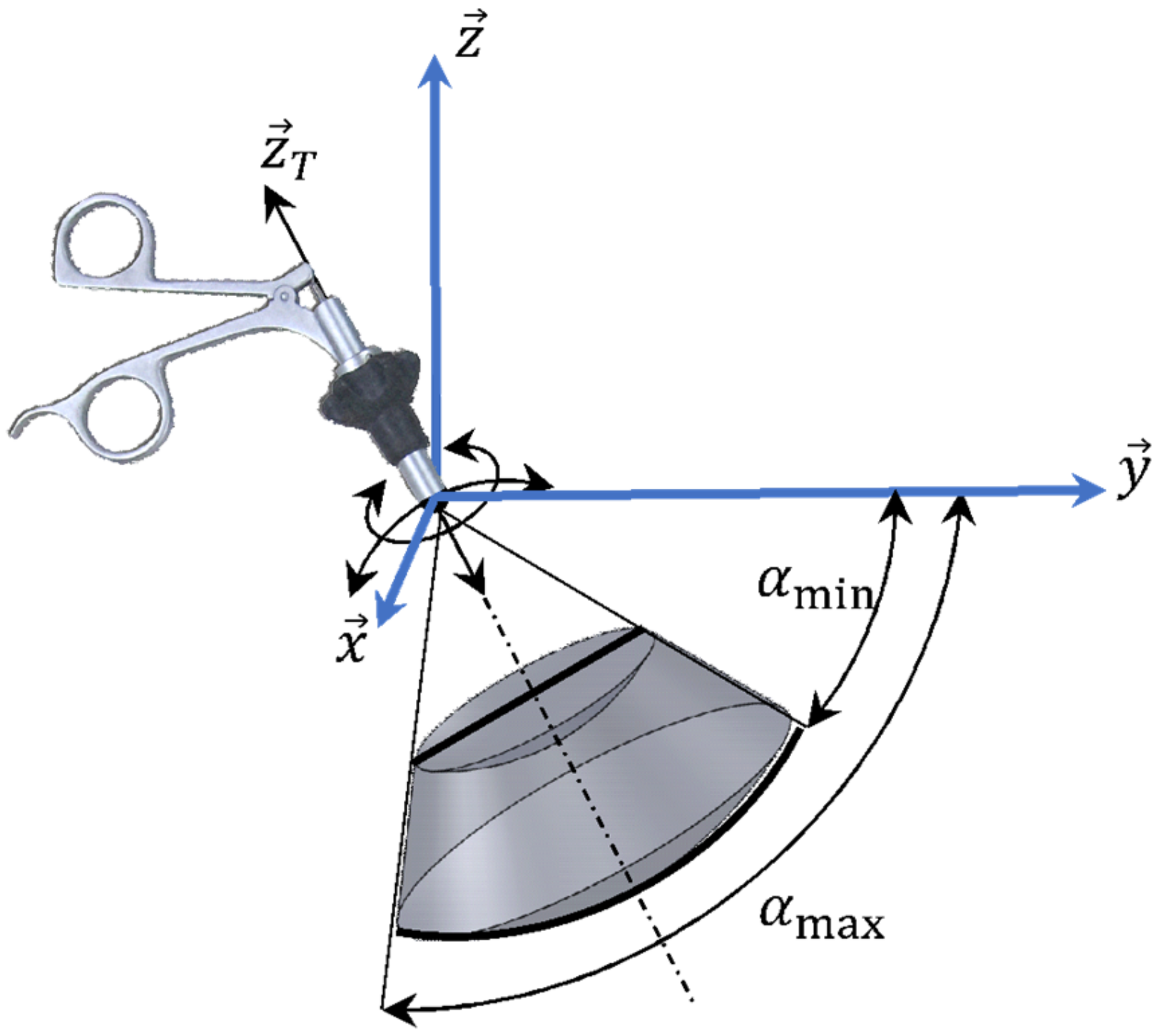
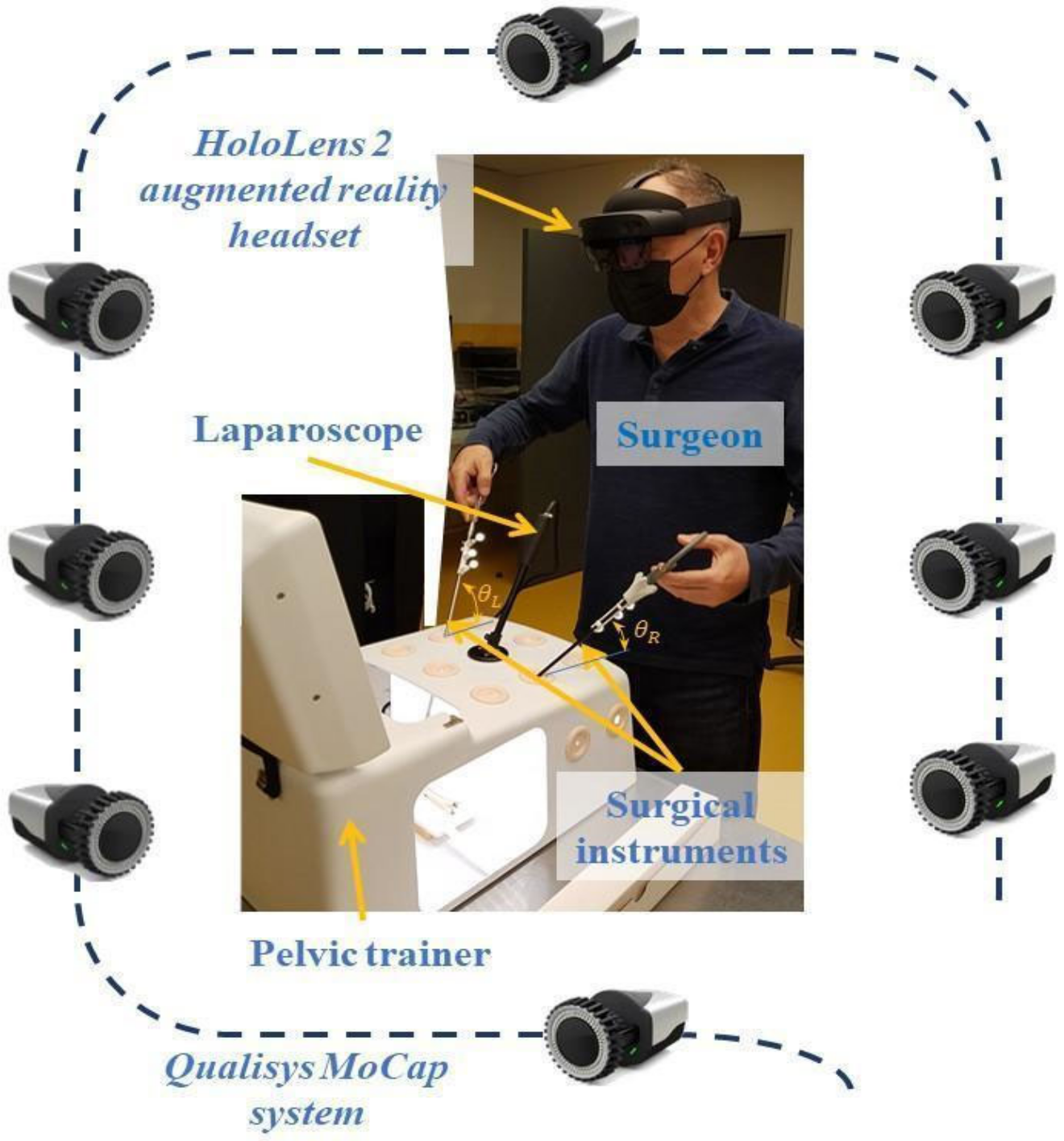
4.3.2. Motion Capture System Setup
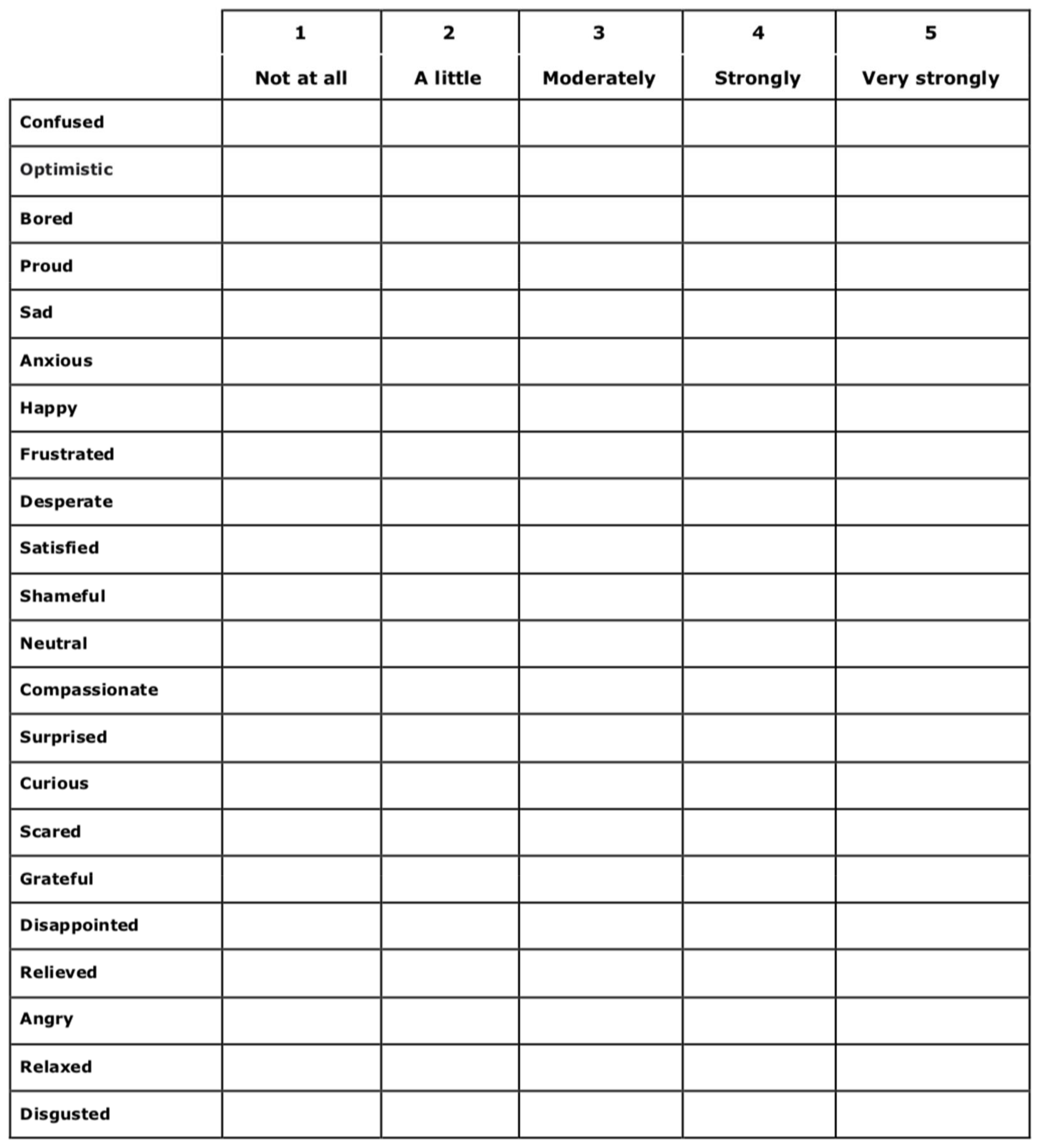
4.3.3. Self-Reported Questionnaire (Emotional State)
4.3.4. HoloLens-2 Headset—Feedback and Disruptive Events
4.4. Statistical Tests Applied
5. Results
5.1. Descriptive Results
5.2. Inferential Results
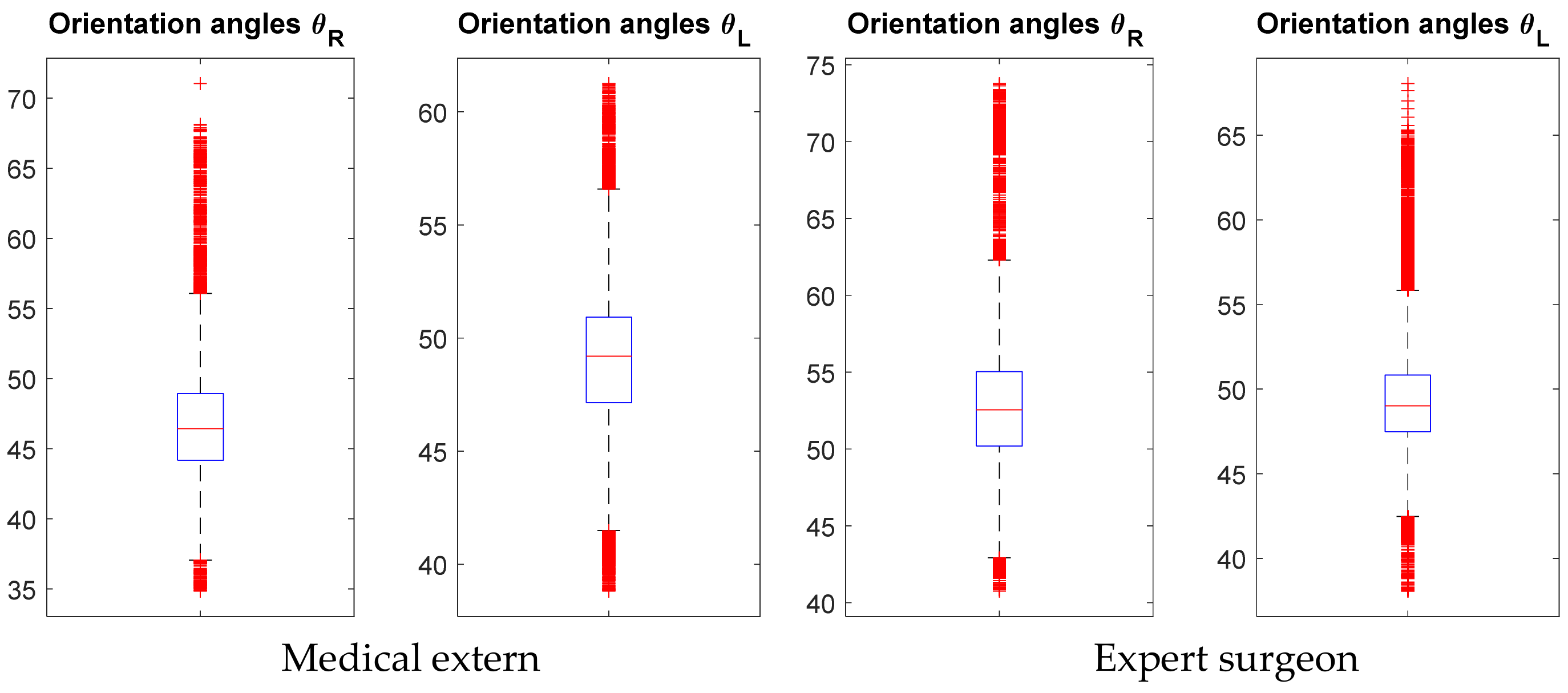
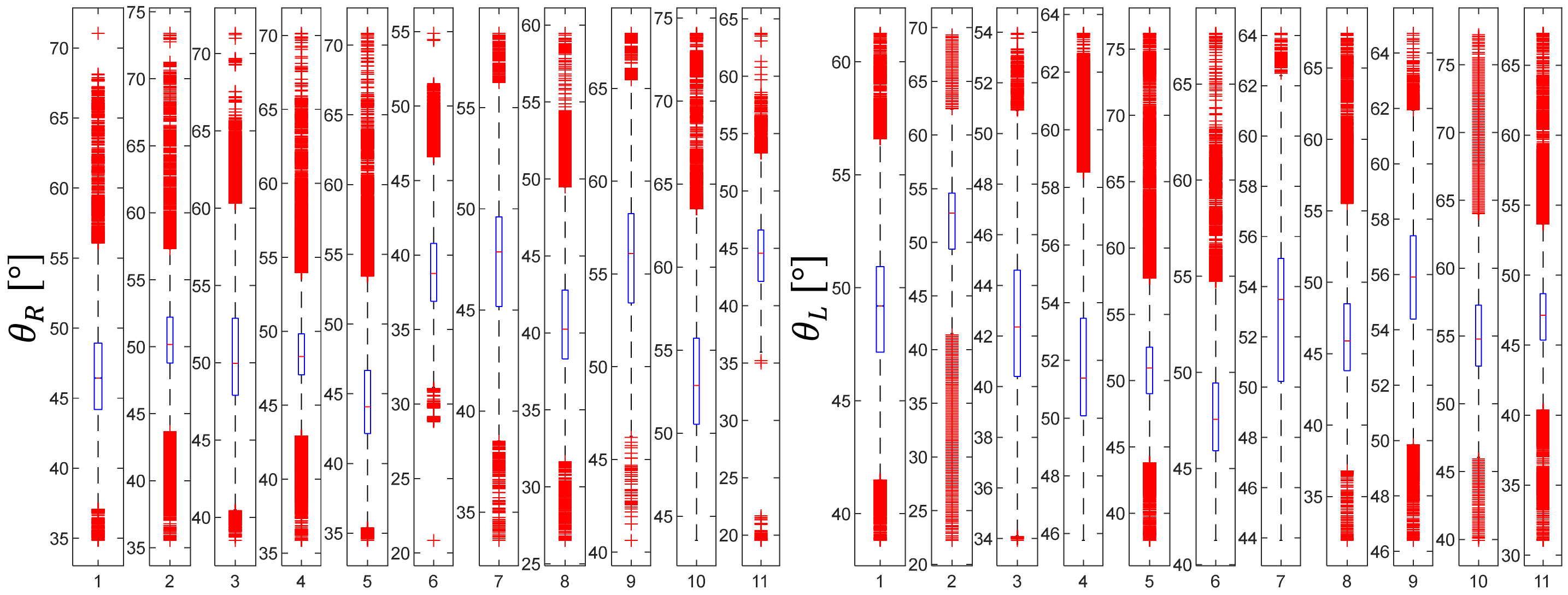
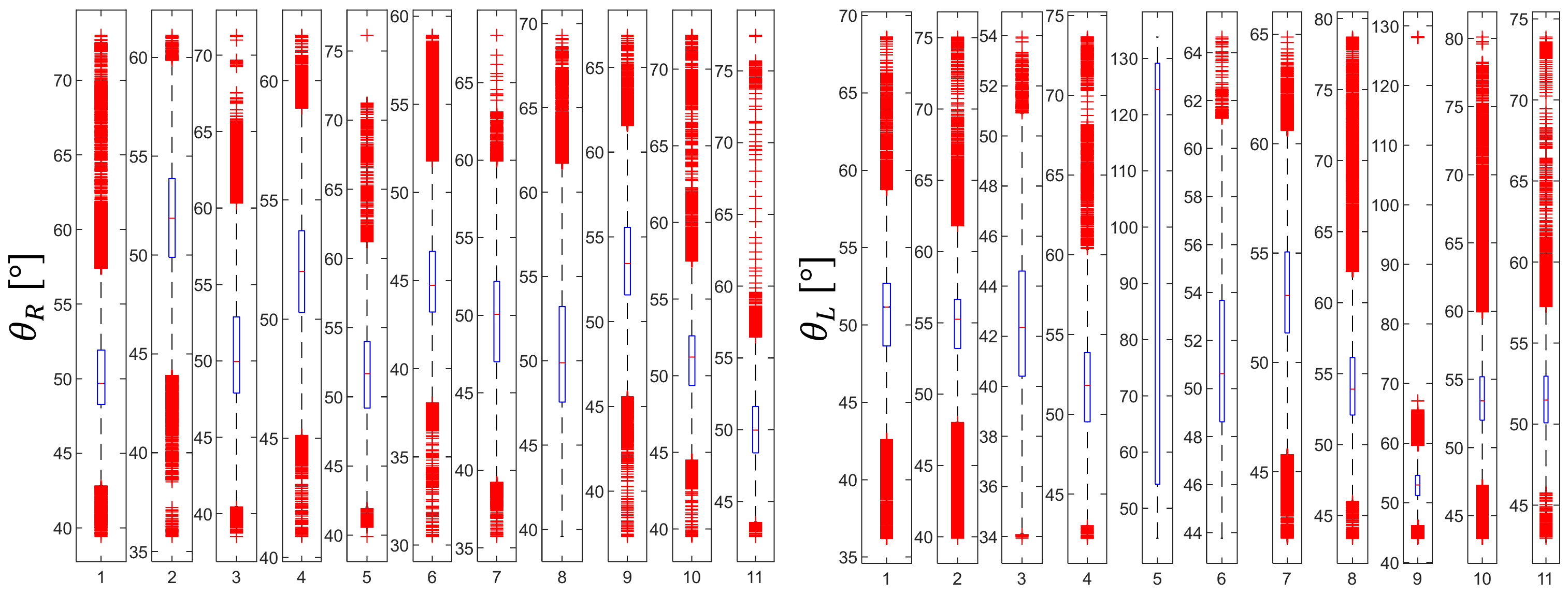
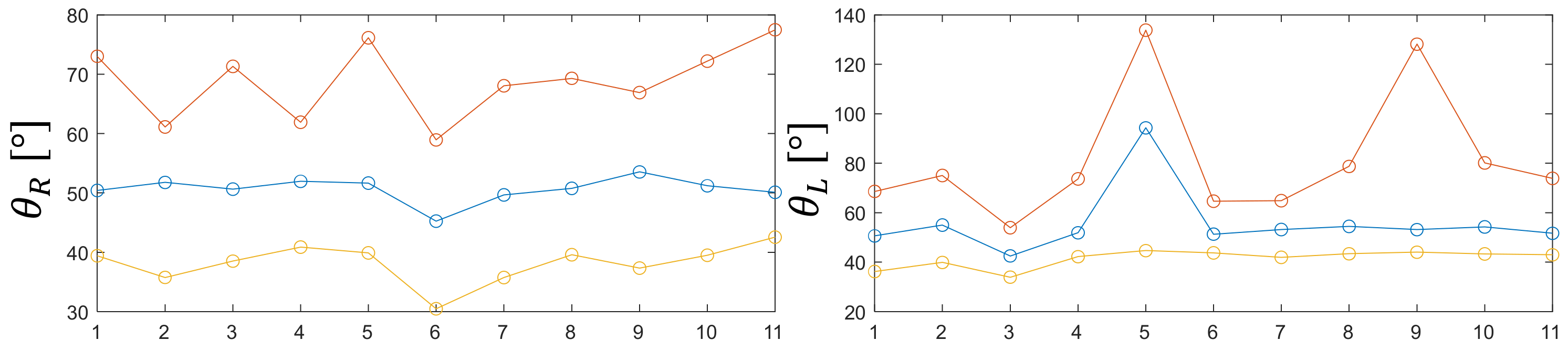
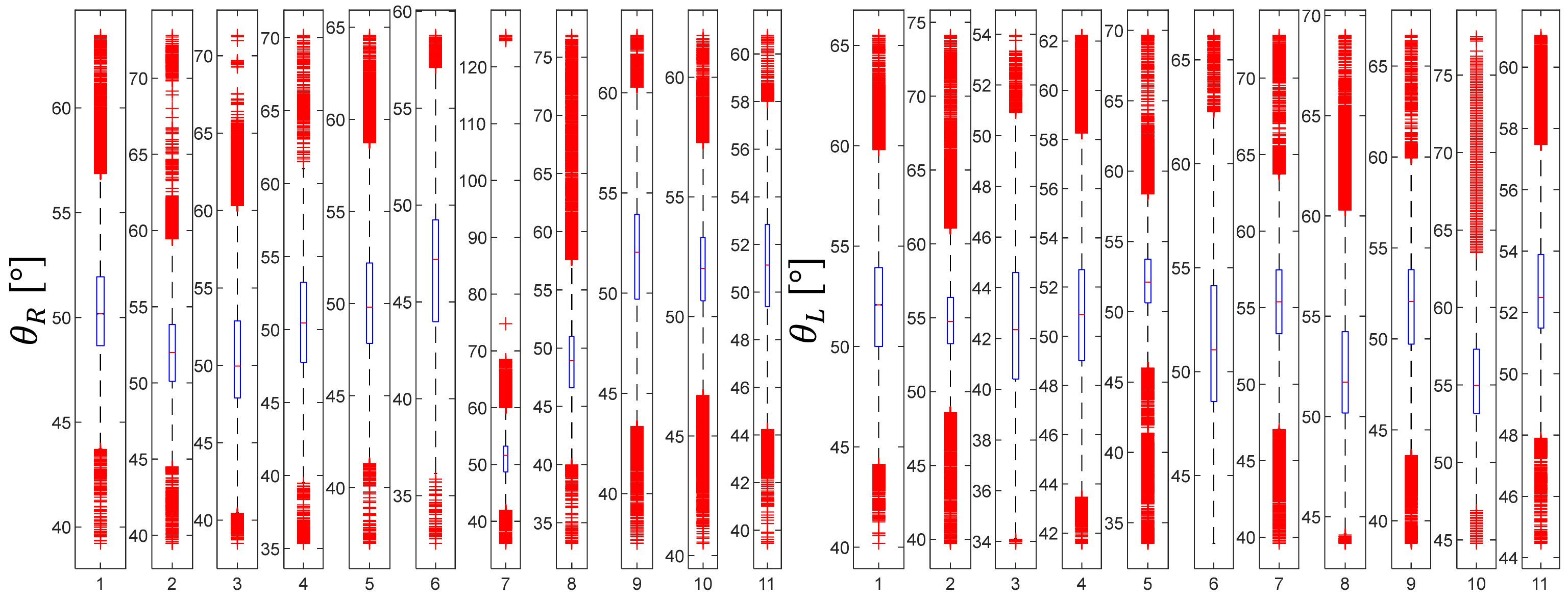
5.3. Motion Capture Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Self-Efficacy Belief and Task Instructions (SEB Group)
Appendix B. Self-Reported Questionnaire (Medical Emotion Scale) Given to the Participants before and after the Task

Appendix C. Template of the Feedbacks/Disruptive Events via HoloLens-2 for SEB and NSEB Groups
References
- Elek, R.N.; Haidegger, T. Robot-assisted minimally invasive surgical skill assessment—Manual and automated platforms. Acta Polytech. Hung. 2019, 16, 141–169. [Google Scholar]
- Funke, I.; Mees, S.T.; Weitz, J.; Speidel, S. Video-based surgical skill assessment using 3D convolutional neural networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1217–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, M.; McKechnie, T.; Khalid, S.; Grantcharov, T.P.; Goldenberg, M. Automated methods of technical skill assessment in surgery: A systematic review. J. Surg. Educ. 2019, 76, 1629–1639. [Google Scholar] [CrossRef] [PubMed]
- Pons, F.; de Rosnay, M.; Cuisinier, F. Cognition and emotion. In Learning and Cognition—Vol. 5, E. Baker, P. Peterson, & B.McGaw (Eds) International Encyclopedia of Education, 3rd ed.; Aukrust, V.G., Ed.; Elsevier: Oxford, UK, 2010. [Google Scholar]
- Fiedler, K.; Beier, K. Affect and cognitive processes in educational contexts. In International Handbook of Emotions in Education; Perkun, R., Linnenbrink-Garcia, L., Eds.; Routledge: New York, NY, USA, 2014. [Google Scholar]
- King, D.; Ritchie, S.; Sandhu, M.; Henderson, S. Emotionally intense science activities. Int. J. Sci. Educ. 2015, 37, 1886–1914. [Google Scholar] [CrossRef] [Green Version]
- Arguel, A.; Lockyer, L.; Lipp, O.V.; Lodge, J.M.; Kennedy, G. Inside Out Detecting Learners’ Confusion to Improve Interactive Digital Learning Environments. J. Educ. Comput. Res. 2017, 55, 5526–5551. [Google Scholar] [CrossRef] [Green Version]
- Brun, A.; Caniato, F.; Caridi, M.; Castelli, C.; Miragliotta, G.; Ronchi, S.; Sianesi, A.; Spina, G. Logistics and supply chain management in luxury fashion retail: Empirical investigation of italian firms. Int. J. Prod. Econ. 2008, 114, 554–570. [Google Scholar] [CrossRef]
- Elgin, C.Z. Emotion and understanding. In Epistemology and Emotions; Routledge: New York, NY, USA, 2008; pp. 33–50. [Google Scholar]
- Mayer, R.E. Multimedia Learning, 3rd ed.; Cambridge University Press: Cambridge, UK, 2021. [Google Scholar]
- Morton, A. Epistemic emotions. In The Oxford Handbook of Philosophy of Emotion; Peter, G., Ed.; Oxford University Press: Oxford, UK, 2010; pp. 385–399. [Google Scholar]
- Arguel, A.; Lockyer, L.; Kennedy, G.; Lodge, J.M.; Pachman, M. Seeking optimal confusion: A review on epistemic emotion management in interactive digital learning environments. Interact. Learn. Environ. 2019, 27, 200–210. [Google Scholar] [CrossRef]
- Lodge, J.M.; Kennedy, G.; Lockyer, L.; Arguel, A.; Pachman, M. Understanding Difficulties and Resulting Confusion in Learning: An Integrative Review. Front. Educ. 2018, 3, 49. [Google Scholar] [CrossRef] [Green Version]
- Fitts, P.M.; Posner, M.I. Human Performance; Brooks/Cole: Belmont, CA, USA, 1967. [Google Scholar]
- Rosser, J.C. The Impact of Video Games on Training Surgeons in the 21st Century. Arch. Surg. 2007, 142, 181. [Google Scholar] [CrossRef] [Green Version]
- Allcoat, D.; von Mühlenen, A. Learning in virtual reality: Effects on performance, emotion and engagement. Res. Learn. Technol. 2018, 26, 2140. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.A.; Dafoulas, G.A.; Augusto, J.C. Collaborative Educational Environments Incorporating Mixed Reality Technologies: A Systematic Mapping Study. IEEE Trans. Learn. Technol. 2019, 12, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Kitchenham, B.A.; Charters, S. Guidelines for Performing Systematic Literature Reviews in Software Engineering (EBSE 2007-001); Keele University and Durham University Joint Report; EBSE: Keele, UK, 2007. [Google Scholar]
- Bacca, J.; Baldiris, S.; Fabregat, R. Insights Into the Factors Influencing Student Motivation in Augmented Reality Learning Experiences in Vocational Education and Training. Front. Psychol. 2018, 9, 1486. [Google Scholar] [CrossRef] [PubMed]
- Tamim, R.M.; Bernard, R.M.; Borokhovski, E.; Abrami, P.C.; Schmid, R.F. What Forty Years of Research Says About the Impact of Technology on Learning: A Second-Order Meta-Analysis and Validation Study. Rev. Educ. Res. 2011, 81, 4–28. [Google Scholar] [CrossRef] [Green Version]
- Dewey, J. Experience and Education; Collier: New York, NY, USA, 1938. [Google Scholar]
- Botden, S.M.; Jakimowicz, J.J. What is going on in augmented reality simulation in laparoscopic surgery? Surg. Endosc. 2008, 23, 1693–1700. [Google Scholar] [CrossRef] [Green Version]
- Pekrun, R. The control-value theory of achievement emotions: Assumptions, corollaries, and implications for educational research and practice. Educ. Psychol. Rev. 2006, 18, 315–341. [Google Scholar] [CrossRef]
- Pekrun, R.; Bühner, M. Self-report Measures of Academic Emotions. In International Handbook of Emotions in Education; Routledge: New York, NY, USA, 2014; pp. 561–579. [Google Scholar]
- Efklides, A. Affect, epistemic emotions, metacognition, and self-regulated learning. Teach. Coll. Rec. 2017, 119, 1–22. [Google Scholar] [CrossRef]
- Bandura, A.; Adams, N.E.; Hardy, A.B.; Howells, G.N. Tests of the generality of self-efficacy theory. Cogn. Ther. Res. 1980, 4, 39–66. [Google Scholar] [CrossRef]
- Lecomte, J. Les applications du sentiment d’efficacité personnelle. Savoirs 2004, 5, 59–90. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Gist, M.E.; Mitchell, T.R. Self-Efficacy: A Theoretical Analysis of Its Determinants and Malleability. Acad. Manag. Rev. 1992, 17, 183–211. [Google Scholar] [CrossRef]
- Duffy, M.C.; Lajoie, S.P.; Pekrun, R.; Lachapelle, K. Emotions in medical education: Examining the validity of the Medical Emotion Scale (MES) across authentic medical learning environments. Learn. Instr. 2020, 70, 101150. [Google Scholar] [CrossRef]
- Baker, R.S.; D’Mello, S.K.; Rodrigo, M.T.; Graesser, A.C. Better to be frustrated than bored: The incidence, persistence, and impact of learners’ cognitive–affective states during interactions with three different computer-based learning environments. Int. J. Hum. Comput. Stud. 2010, 68, 223–241. [Google Scholar] [CrossRef] [Green Version]
- Laribi, M.A.; Riviere, T.; Arsicault, M.; Zeghloul, S. A design of slave surgical robot based on motion capture. In Proceedings of the 2012 IEEE International Conference on Robotics and Biomimetics (ROBIO), Guangzhou, China, 11–14 December 2012; pp. 600–605. [Google Scholar] [CrossRef]
- Laribi, M.A.; Riviere, T.; Arsicault, M.; Zeghloul, S. A new teleoperated robotic system for minimally invasive surgery: Modeling and identification. In Proceedings of the 2013 International Conference on Control, Decision and Information Technologies (CoDIT), Hammamet, Tunisia, 6–8 May 2013; pp. 659–664. [Google Scholar]
- Cau, J.; Ricco, J.B.; Marchand, C.; Lecis, A.; Abbibeh, H.; Guillou, M.; Febrer, G.; Bossavy, J. Laparoscopic aortic repair for occlusive and aneurysmal disease: First 95 cases. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 567–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cau, J.; Ricco, J.B.; Marchand, E.; Marchand, C.; Corpataux, J.M. Totally laparoscopic aorto-renal bypass after failed PTA. J. Vasc. Surg. 2011, 53, 87–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Mello, S.; Graesser, A. Confusion and its dynamics during device comprehension with breakdown scenarios. Acta Psychol. 2014, 151, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Bradley, M.M.; Lang, P.J. Measuring emotion: Behavior, feeling, and physiology. In Series in Affective Science. Cognitive Neuroscience of Emotion; Lane, R.D., Nadel, L., Eds.; Oxford University Press: Oxford, UK, 2000; pp. 242–276. [Google Scholar]
- Calvo, R.A.; D’Mello, S. Affect detection: An interdisciplinary review of models, methods, and their applications. IEEE Trans. Affect. Comput. 2010, 1, 18–37. [Google Scholar] [CrossRef]
- Fowles, D.C. The Three Arousal Model: Implications of Gray’s Two-Factor Learning Theory for Heart Rate, Electrodermal Activity, and Psychopathy. Psychophysiology 1980, 17, 87–104. [Google Scholar] [CrossRef]
- Van Dooren, M.; Janssen, J.H. Emotional sweating across the body: Comparing 16 different skin conductance measurement locations. Physiol. Behav. 2012, 106, 298–304. [Google Scholar] [CrossRef]
- Pintrich, P.R. The role of goal orientation in self-regulated learning. In Handbook of Self-Regulation; Boekaerts, M., Pintrich, P.R., Zeidner, M., Eds.; Academic Press: Cambridge, MA, USA, 2000; pp. 451–502. [Google Scholar]
- Bol, L.; Garner, J.K. Challenges in supporting self-regulation in distance education environments. J. Comput. High. Educ. 2011, 23, 104–123. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. /Psychol. Can. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Lehman, B.; D’Mello, S.; Graesser, A. Confusion and complex learning during interactions with computer learning environments. Internet High. Educ. 2012, 15, 184–194. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Virtual Simulation | (HoloLens-2) | ||
|---|---|---|---|
| With | Without | ||
| Self-efficacy | With | CG | NSEB |
| instruction | Without | - - | SEB |
| Time | Positive | M (SD) | Negative | M (SD) |
|---|---|---|---|---|
| Before | Curious | 3.9 (1.0) | Anxious | 1.8 (0.7) |
| Grateful | 3.7 (0.9) | Scare | 1.5 (0.8) | |
| Happy | 3.5 (1.0) | Surprised | 1.3 (0.8) | |
| Optimistic | 3.0 (0.9) | Confused | 1.2 (0.5) | |
| Determined | 2.9 (1.0) | Frustrated | 1.2 (0.5) | |
| After | Grateful | 3.8 (0.9) | Frustrated | 2.6 (1.3) |
| Curious | 3.7 (1.1) | Disappointed | 2.2 (1.3) | |
| Optimistic | 3.1 (1.1) | Confused | 1.6 (0.8) | |
| Happy | 2.9 (1.1) | Disgust | 1.6 (0.9) | |
| Proud | 2.7 (1.2) | Bored | 1.5 (0.7) |
| Before Task | After Task | |
|---|---|---|
| Variables 1 | M (SD) | M (SD) |
| Positive activation | 2 (0.4) | 2.4 (0.5) |
| Positive deactivation | 1.9 (0.5) | 2.0 (0.6) |
| Negative activation | 2.1 (0.3) | 2.0 (0.4) |
| Negative deactivation | 1.5 (0.3) | 1.9 (0.3) |
| SEB | NSEB | CG | ||||
|---|---|---|---|---|---|---|
| Variables 1 | M (SD) | Mdn | M (SD) | Mdn | M (SD) | Mdn |
| Positive activation | 2.1 (0.3) | 2 | 2.1 (0.5) | 2 | 1.8 (0.4) | 1.8 |
| Positive deactivation | 2.0 (0.7) | 2 | 2.1 (0.4) | 2 | 1.6 (0.4) | 1.5 |
| Negative activation | 2.1 (0.3) | 2 | 2.05 (0.4) | 2.1 | 2.1 (0.3) | 2.1 |
| Negative deactivation | 1.4 (0.3) | 1.5 | 1.5 (0.3) | 1.5 | 1.5 (0.3) | 1.5 |
| Needle holder | 49 (7.9) | 52.1 | 55 (17.7) | 51.9 | 49.5 (3.6) | 50.8 |
| Clamp | 51.4 (2.4) | 51.5 | 49.1 (3.1) | 50.1 | 47.5 (3.9) | 48.4 |
| Suture | 9.4 (2.3) | 10 | 10.1 (2.3) | 10.5 | 10.9 (2.3) | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cau, M.; Sandoval, J.; Arguel, A.; Breque, C.; Huet, N.; Cau, J.; Laribi, M.A. Toward Optimal Learning of the Gesture in Laparoscopic Surgery: Methodology and Performance. J. Clin. Med. 2022, 11, 1398. https://doi.org/10.3390/jcm11051398
Cau M, Sandoval J, Arguel A, Breque C, Huet N, Cau J, Laribi MA. Toward Optimal Learning of the Gesture in Laparoscopic Surgery: Methodology and Performance. Journal of Clinical Medicine. 2022; 11(5):1398. https://doi.org/10.3390/jcm11051398
Chicago/Turabian StyleCau, Marine, Juan Sandoval, Amaël Arguel, Cyril Breque, Nathalie Huet, Jerome Cau, and Med Amine Laribi. 2022. "Toward Optimal Learning of the Gesture in Laparoscopic Surgery: Methodology and Performance" Journal of Clinical Medicine 11, no. 5: 1398. https://doi.org/10.3390/jcm11051398