
Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Inclusion Criteria and Study Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bredy, C.; Ministeri, M.; Kempny, A.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Diller, G.-P.; Gatzoulis, M.A.; Dimopoulos, K. New York Heart Association (NYHA) classification in adults with congenital heart disease: Relation to objective measures of exercise and outcome. Eur. Hear. J. Qual. Care Clin. Outcomes 2017, 4, 51–58. [Google Scholar] [CrossRef] [PubMed]
- The CAPACITY-COVID Collaborative Consortium and LEOSS Study Group; Linschoten, M.; Uijl, A.; Schut, A.; Jakob, C.E.M.; Romão, L.R.; Bell, R.M.; McFarlane, E.; Stecher, M.; Zondag, A.G.M.; et al. Clinical presentation, disease course, and outcome of COVID-19 in hospitalized patients with and without pre-existing cardiac disease: A cohort study across 18 countries. Eur. Hear. J. 2021, ehab656. [Google Scholar] [CrossRef]
- Maehl, N.; Bleckwenn, M.; Riedel-Heller, S.G.; Mehlhorn, S.; Lippmann, S.; Deutsch, T.; Schrimpf, A. The Impact of the COVID-19 Pandemic on Avoidance of Health Care, Symptom Severity, and Mental Well-Being in Patients with Coronary Artery Disease. Front. Med. 2021, 8, 760265. [Google Scholar] [CrossRef] [PubMed]
- Augustine, R.; S, A.; Nayeem, A.; Salam, S.A.; Augustine, P.; Dan, P.; Maureira, P.; Mraiche, F.; Gentile, C.; Hansbro, P.M.; et al. Increased complications of COVID-19 in people with cardiovascular disease: Role of the renin-angiotensin-aldosterone system (RAAS) dysregulation. Chem. Interact. 2021, 351, 109738. [Google Scholar] [CrossRef]
- Albashir, A.A.D. Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors and Coronavirus Disease 2019 (COVID-19). South Med. J. 2021, 114, 51–56. [Google Scholar] [CrossRef]
- Patel, V.; Zhong, J.-C.; Grant, M.B.; Oudit, G.Y. Role of the ACE2/Angiotensin 1–7 Axis of the Renin-Angiotensin System in Heart Failure. Circ. Res. 2016, 118, 1313–1326. [Google Scholar] [CrossRef] [Green Version]
- Thum, T. SARS-CoV-2 receptor ACE2 expression in the human heart: Cause of a post-pandemic wave of heart failure? Eur. Heart J. 2020, 41, 1807–1809. [Google Scholar] [CrossRef]
- Bargehr, J.; Rericha, P.; Petchey, A.; Colzani, M.; Moule, G.; Malgapo, M.C.; Rassl, D.; Tarkin, J.; Mellor, G.; Sampaziotis, F.; et al. Car-diovascular ACE2 receptor expression in patients undergoing heart transplantation. ESC Heart Fail. 2021, 8, 4119–4129. [Google Scholar] [CrossRef]
- Gopal, R.; Marinelli, M.A.; Alcorn, J.F. Immune Mechanisms in Cardiovascular Diseases Associated with Viral Infection. Front. Immunol. 2020, 11, 570681. [Google Scholar] [CrossRef]
- Watson, A.; Wilkinson, T.M.A. Respiratory viral infections in the elderly. Ther. Adv. Respir. Dis. 2021, 15, 1753466621995050. [Google Scholar] [CrossRef]
- Lozahic, C.; Maddock, H.; Sandhu, H. Anti-cancer Therapy Leads to Increased Cardiovascular Susceptibility to COVID-19. Front. Cardiovasc. Med. 2021, 8, 634291. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Bottino, R.; Carbone, A.; Rago, A.; Papa, A.A.; Golino, P.; Nigro, G. COVID-19 and Heart: From Clinical Features to Pharmacological Implications. J. Clin. Med. 2020, 9, 1944. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, P.; Calcaterra, I.; Molino, A.; Moretta, P.; Lupoli, R.; Spedicato, G.A.; Papa, A.; Motta, A.; Maniscalco, M.; Di Minno, M.N.D. Persistent Endothelial Dysfunction in Post-Acute COVID-19 Syndrome: A Case-Control Study. Biomedicines 2021, 9, 957. [Google Scholar] [CrossRef] [PubMed]
- Maruhashi, T.; Higashi, Y. Pathophysiological Association of Endothelial Dysfunction with Fatal Outcome in COVID-19. Int. J. Mol. Sci. 2021, 22, 5131. [Google Scholar] [CrossRef]
- Available online: https://www.cardioportal.ro/wp-content/uploads/2018/04/comunicat-presa-insuficien%C8%9B%C4%83-cardiac%C4%83_20-martie-2018-final_dv1.pdf (accessed on 29 January 2022).
- Sisti, N.; Valente, S.; Mandoli, G.E.; Santoro, C.; Sciaccaluga, C.; Franchi, F.; Cameli, P.; Mondillo, S.; Cameli, M. COVID-19 in patients with heart failure: The new and the old epidemic. Postgrad. Med. J. 2021, 97, 175–179. [Google Scholar] [CrossRef]
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of heart failure on the outcome of COVID-19—A meta analysis and systematic review. Am. J. Emerg. Med. 2020, 46, 204–211. [Google Scholar] [CrossRef]
- Abu Ghosh, Z.; Zwas, D.R.; Keren, A.; Elbaz-Greener, G.; Israeli, V.; Amir, O.; Gotsman, I. The Impact of COVID-19 Pandemic on Management and Outcome in Patients with Heart Failure. J. Clin. Med. 2021, 10, 5577. [Google Scholar] [CrossRef]
- Castagna, F.; Kataria, R.; Madan, S.; Ali, S.Z.; Diab, K.; Leyton, C.; Arfaras-Melainis, A.; Kim, P.; Giorgi, F.M.; Vukelic, S.; et al. A History of Heart Failure Is an Independent Risk Factor for Death in Patients Admitted with Coronavirus 19 Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 77. [Google Scholar] [CrossRef]
- Sokolski, M.; Reszka, K.; Suchocki, T.; Adamik, B.; Doroszko, A.; Drobnik, J.; Gorka-Dynysiewicz, J.; Jedrzejczyk, M.; Kaliszewski, K.; Kilis-Pstrusinska, K.; et al. History of Heart Failure in Patients Hospitalized Due to COVID-19: Relevant Factor of In-Hospital Complications and All-Cause Mortality up to Six Months. J. Clin. Med. 2022, 11, 241. [Google Scholar] [CrossRef]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef]
- Nguyen, K.; Fan, W.; Bertoni, A.; Budoff, M.J.; Defilippi, C.; Lombardo, D.; Maisel, A.; Szklo, M.; Wong, N.D. N-terminal Pro B-type Natriuretic Peptide and High-sensitivity Cardiac Troponin as Markers for Heart Failure and Cardiovascular Disease Risks According to Glucose Status (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am. J. Cardiol. 2020, 125, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Tersalvi, G.; Vicenzi, M.; Calabretta, D.; Biasco, L.; Pedrazzini, G.; Winterton, D. Elevated Troponin in Patients with Coronavirus Disease 2019: Possible Mechanisms. J. Card. Fail. 2020, 26, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Wang, X.Q.; Iwashyna, T.J.; Prescott, H.C. Readmission and Death After Initial Hospital Discharge Among Patients With COVID-19 in a Large Multihospital System. JAMA 2021, 325, 304–306. [Google Scholar] [CrossRef] [PubMed]




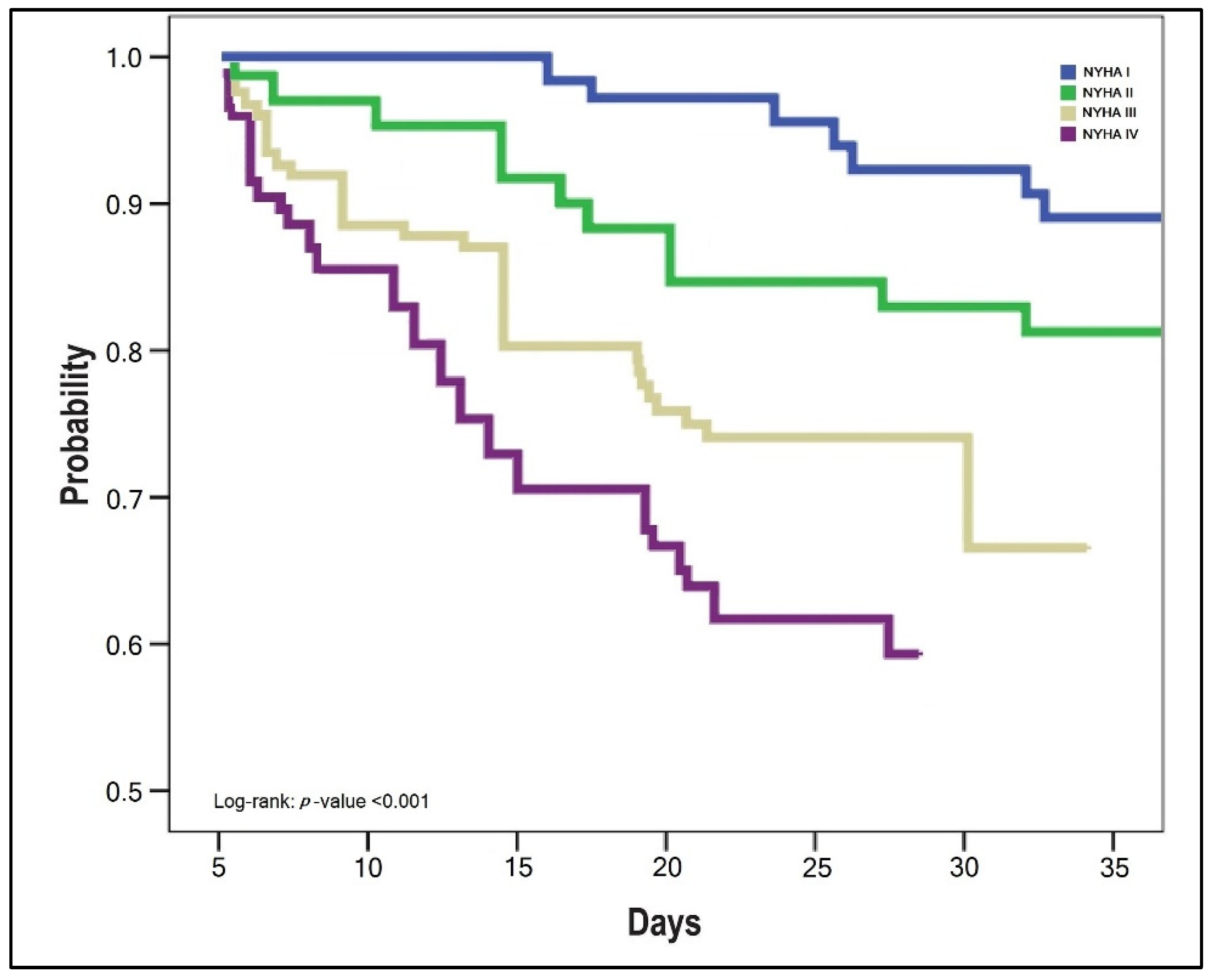{kind=link}
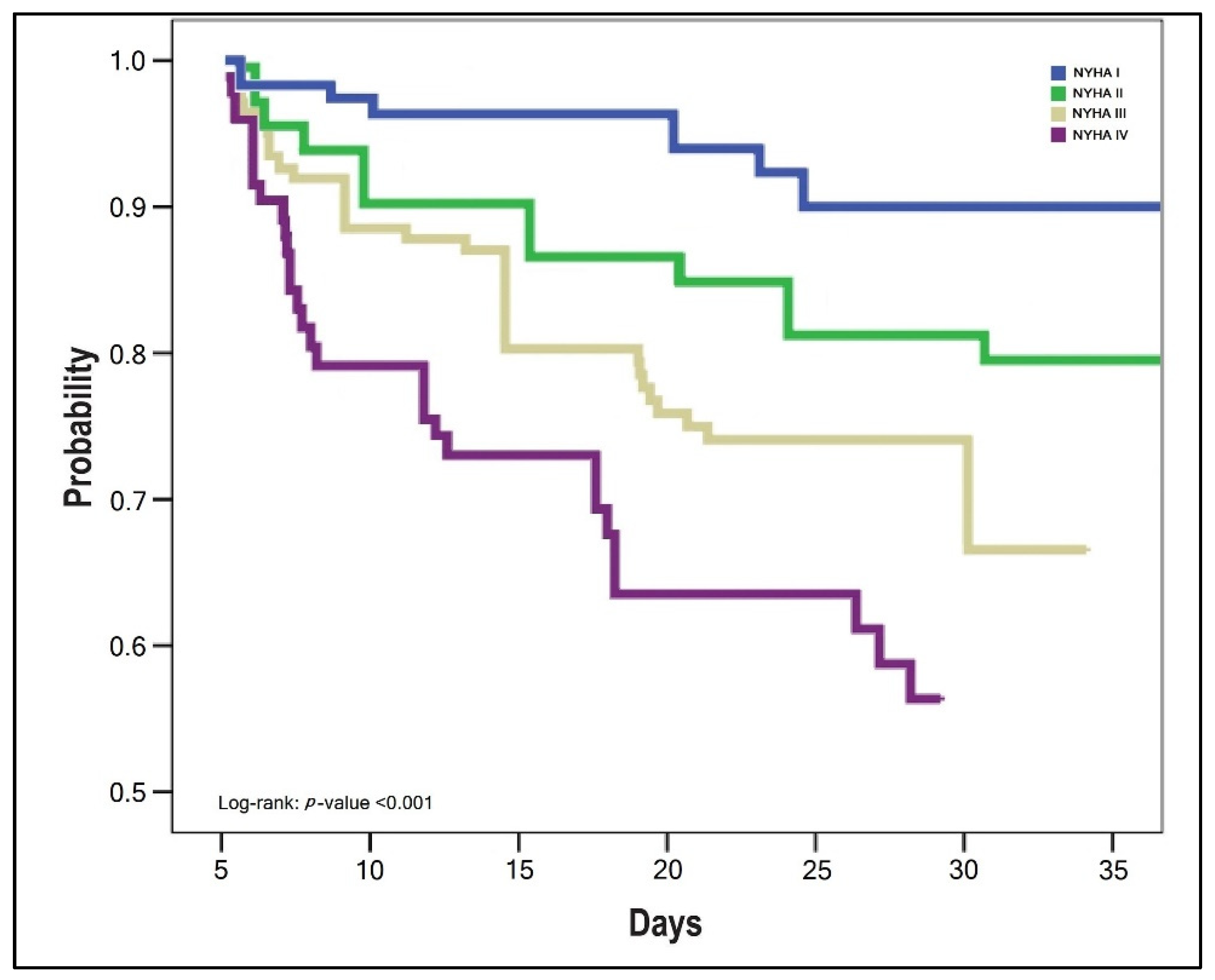{kind=link}
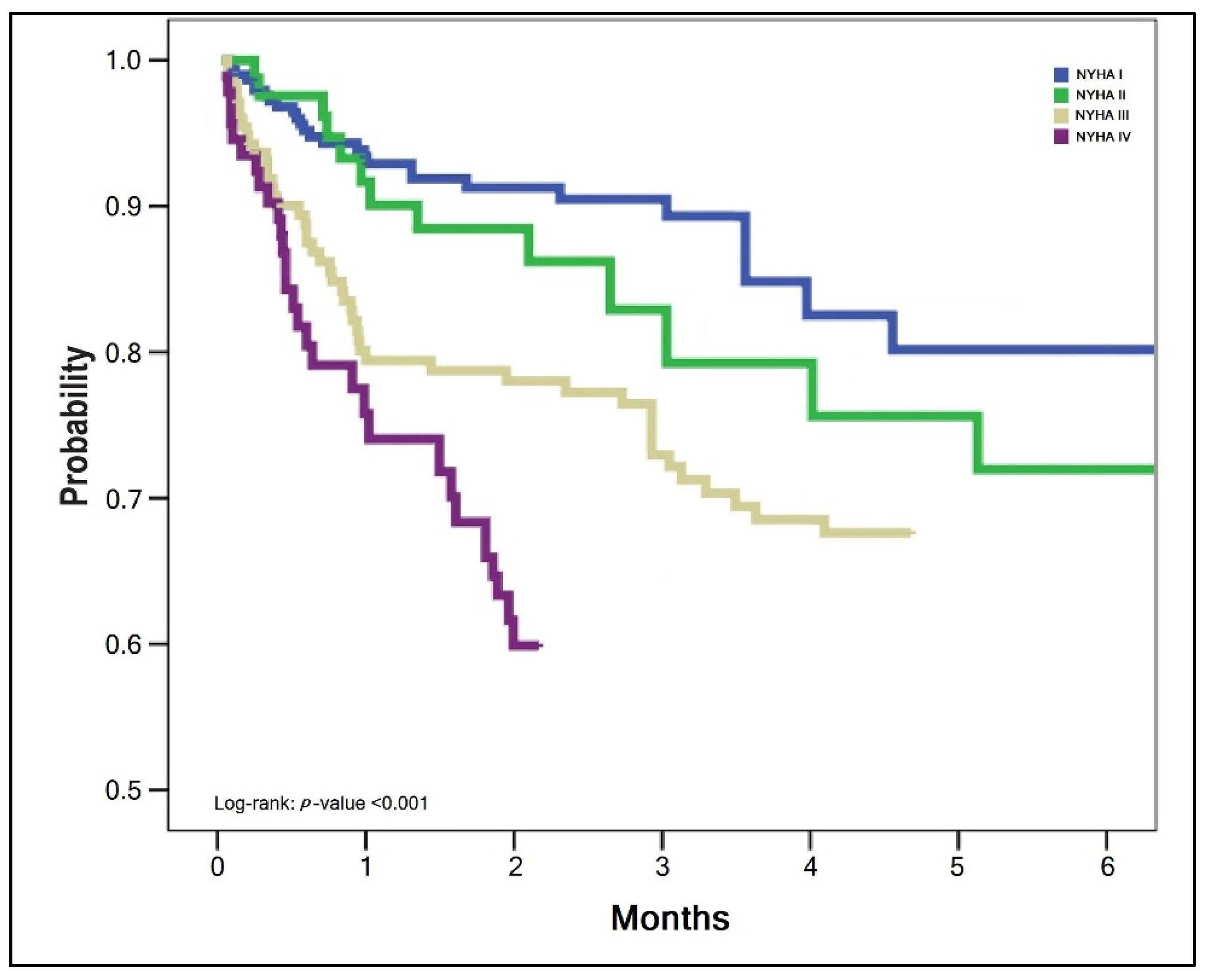{kind=link}
| Variables * | NYHA I (n = 29) | NYHA II (n = 44) | NYHA III (n = 35) | NYHA IV (n = 23) | p-Value |
|---|---|---|---|---|---|
| Age, years | <0.001 | ||||
| 18–35 | 4 (13.8%) | 1 (2.3%) | - | - | |
| 35–65 | 18 (62.1%) | 20 (45.4%) | 11 (31.4%) | 6 (26.1%) | |
| >65 | 7 (24.1%) | 23 (52.3%) | 24 (68.6%) | 17 (73.9%) | |
| Sex | 0.019 | ||||
| Men | 10 (34.5%) | 28 (63.6%) | 25 (71.4%) | 14 (60.9%) | |
| Women | 19 (65.5%) | 16 (36.4%) | 10 (28.6%) | 9 (39.1%) | |
| Weight, BMI (kg/m2) | 0.633 | ||||
| <25 | 4 (13.8%) | 4 (9.1%) | 4 (11.4%) | 1 (4.4%) | |
| 25–30 | 7 (24.1%) | 5 (13.4%) | 8 (22.9%) | 5 (21.7%) | |
| >35 | 18 (62.1%) | 35 (79.5%) | 23 (65.7%) | 17 (73.9%) | |
| Cardiovascular risk factors | |||||
| Smoking | 10 (34.4%) | 12 (27.3%) | 17 (48.6%) | 14 (60.9%) | 0.036 |
| Arterial hypertension | 9 (31.0%) | 15 (34.1%) | 24 (68.7%) | 17 (73.9%) | 0.003 |
| Diabetes mellitus | 8 (27.6%) | 10 (22.7%) | 12 (34.3%) | 15 (65.2%) | 0.004 |
| Dyslipidemia | 7 (24.1%) | 9 (20.5%) | 13 (37.1%) | 13 (56.5%) | 0.016 |
| Comorbidities at admission | |||||
| Cerebrovascular disease | 2 (6.9%) | 4 (9.1%) | 5 (14.3%) | 7 (30.4%) | 0.061 |
| Chronic kidney disease | 3 (10.3%) | 3 (6.8%) | 7 (20.0%) | 7 (30.4%) | 0.053 |
| COPD | 2 (6.9%) | 2 (4.5%) | 6 (17.1%) | 5 (21.7%) | 0.103 |
| Daily medication | |||||
| Beta-blockers | 22 (75.9%) | 37 (84.1%) | 31 (88.6%) | 19 (82.6%) | 0.599 |
| Calcium channel blockers | 10 (34.5%) | 25 (56.8%) | 19 (54.3%) | 16 (69.6%) | 0.078 |
| Angiotensin receptor blockers | 8 (27.6%) | 12 (27.3%) | 12 (34.3%) | 5 (21.7%) | 0.768 |
| ACE inhibitors | 21 (72.4%) | 32 (72.7%) | 32 (91.4%) | 20 (86.9%) | 0.107 |
| Loop diuretics | 23 (79.3%) | 40 (90.1%) | 31 (88.6%) | 23 (100%) | 0.115 |
| Potassium-sparing diuretics | 14 (48.3%) | 16 (36.4%) | 30 (85.7%) | 21 (91.3%) | <0.001 |
| Aldosterone antagonists | 8 (27.6%) | 12 (27.3%) | 17 (48.6%) | 17 (73.9%) | <0.001 |
| Antiplatelet drugs | 7 (24.1%) | 17 (38.6%) | 12 (34.3%) | 10 (43.5%) | 0.477 |
| Nitrates | 7 (24.1%) | 20 (45.5%) | 19 (54.3%) | 8 (34.8%) | 0.082 |
| Variables * | NYHA I (n = 29) | NYHA II (n = 44) | NYHA III (n = 35) | NYHA IV (n = 23) | p-Value |
|---|---|---|---|---|---|
| COVID-19 severity | <0.001 | ||||
| Mild | 14 (48.3%) | 10 (22.7%) | 8 (22.9%) | 4 (17.4%) | |
| Moderate | 10 (34.5%) | 27 (61.4%) | 9 (25.7%) | 4 (17.4%) | |
| Severe | 5 (17.2%) | 7 (15.9%) | 18 (51.4%) | 15 (65.2%) | |
| Days from first symptoms until admission (median, [IQR]) | 7 [3–11] | 6 [2–9] | 4 [1–7] | 2 [1–4] | <0.001 |
| Days of hospitalization (median, [IQR]) | 10 [7–14] | 14 [9–16] | 18 [8–25] | 20 [10–29] | <0.001 |
| Vitals | |||||
| Pulse, mean ± SD | 87.1 ± 16.1 | 91.0 ± 16.6 | 95.1 ± 18.3 | 98.7 ± 19.0 | 0.083 |
| Temperature, mean ± SD | 38.4 ± 1.8 | 38.7 ± 1.7 | 38.0 ± 1.8 | 37.7 ± 1.2 | 0.089 |
| Systolic blood pressure, mean ± SD | 151 ± 21.2 | 136 ± 22.4 | 112 ± 17.6 | 108 ± 23.7 | <0.001 |
| Dyastolic blood pressure, mean ± SD | 86 ± 10.8 | 74 ± 10.2 | 68 ± 9.4 | 66 ± 9.1 | <0.001 |
| O2 saturation at admission (%), mean ± SD | 94 ± 4.8 | 92 ± 5.0 | 88 ± 3.9 | 86 ± 3.6 | <0.001 |
| Oxygen supplementation | <0.001 | ||||
| No supplementation | 6 (20.7%) | 6 (13.6%) | - | - | |
| Non-invasive ventilation | 17 (58.6%) | 28 (63.6%) | 18 (51.4%) | 11 (47.8%) | |
| Invasive ventilation | 6 (20.7%) | 10 (22.8%) | 17 (48.6%) | 12 (52.2%) | |
| Outcomes | |||||
| Severe in-hospital complications ** | 5 (17.2%) | 7 (15.9%) | 10 (28.6%) | 11 (47.8%) | 0.023 |
| Intensive-care unit admission | 6 (20.7%) | 10 (22.8%) | 17 (48.6%) | 12 (52.2%) | 0.009 |
| In-hospital mortality | 2 (6.9%) | 6 (13.6%) | 10 (28.6%) | 11 (47.8%) | 0.025 |
| Overall mortality (6 months) | 3 (10.3%) | 8 (18.2%) | 14 (40.0%) | 15 (65.2%) | <0.001 |
| Discharged and rehospitalized in 1 month | 4/27 (14.8%) | 7/38 (18.4%) | 11/25 (44.0%) | 12/12 (100%) | <0.001 |
| Days from discharge until rehospitalization (median, [IQR]) | 24 [18–28] | 21 [15–26] | 16 [11–20] | 10 [4–14] | <0.001 |
| Variables * | NYHA I (n = 29) | NYHA II (n = 44) | NYHA III (n = 35) | NYHA IV (n = 23) | p-Value |
|---|---|---|---|---|---|
| Cardiac ultrasound | |||||
| Left ventricle ejection fraction | 0.040 | ||||
| ≥40% | 7 (24.1%) | 8 (18.2%) | 5 (14.3%) | 2 (8.7%) | |
| 40–30% | 9 (31.0%) | 11 (25.0%) | 4 (11.4%) | 1 (4.4%) | |
| <30% | 13 (44.9%) | 25 (56.8%) | 26 (72.3%) | 20 (86.9%) | |
| Atrial fibrillation/flutter | 8 (27.6%) | 10 (22.7%) | 9 (25.7%) | 9 (39.1%) | 0.547 |
| Cardiac thrombus | 2 (6.9%) | 3 (6.8%) | 3 (8.6%) | 2 (8.7%) | 0.986 |
| Mitral valve stenosis | - | 3 (6.8%) | 4 (11.4%) | 2 (8.7%) | 0.361 |
| Mitral valve regurgitation | 4 (13.8%) | 5 (11.4%) | 3 (8.6%) | 3 (13.0%) | 0.918 |
| Aortic valve stenosis | 1 (3.4%) | 1 (2.3%) | 1 (2.9%) | - | 0.858 |
| Aortic valve regurgitation | 2 (6.9%) | 3 (6.8%) | 1 (2.9%) | 2 (8.7%) | 0.744 |
| Segmental wall motion abnormality | 4 (13.8%) | 4 (9.1%) | 3 (8.6%) | 5 (21.7%) | 0.415 |
| Pericardial effusion | 2 (6.9%) | 3 (6.8%) | 2 (5.7%) | 2 (8.7%) | 0.978 |
| Right ventricular dysfunction | 3 (10.3%) | 3 (6.8%) | 1 (2.9%) | 2 (8.7%) | 0.671 |
| High pulmonary artery pressure ** | - | 2 (4.5%) | 1 (2.9%) | 1 (4.4%) | 0.710 |
| Lung injury on CT scan | 0.014 | ||||
| Mild (˂30%) | 14 (48.3%) | 17 (38.6%) | 11 (31.4%) | 3 (13.0%) | |
| Moderate (30–60%) | 8 (27.6%) | 19 (43.2%) | 9 (25.7%) | 7 (30.4%) | |
| Severe (>60%) | 7 (24.1%) | 8 (18.2%) | 15 (42.9%) | 13 (56.5%) |
| Variables * | Normal Range | NYHA I (n = 29) | NYHA II (n = 44) | NYHA III (n = 35) | NYHA IV (n = 23) | p-Value |
|---|---|---|---|---|---|---|
| WBC (thousands/mm3) | 4.5–11.0 | 13.2 ± 4.1 | 12.6 ± 4.5 | 12.8 ± 3.9 | 11.4 ± 5.8 | 0.535 |
| Platelets (thousands/mm3) | 150–450 | 308 ± 28 | 284 ± 31 | 206 ± 23 | 127 ± 44 | 0.009 |
| RBC (millions/mm3) | 4.35–5.65 | 4.41 ± 0.8 | 4.28 ± 0.9 | 4.06 ± 1.1 | 3.81 ± 1.8 | 0.235 |
| AST (U/L) | 10–40 | 25 ± 4.2 | 27 ± 5.4 | 31 ± 5.7 | 36 ± 6.1 | <0.001 |
| ALT (U/L) | 7–35 | 21 ± 3.3 | 22 ± 3.1 | 24 ± 3.8 | 25 ± 4.0 | 0.001 |
| Total bilirubin (g/dL) | 0.3–1.2 | 0.7 ± 0.1 | 0.8 ± 0.3 | 0.8 ± 0.2 | 0.9 ± 0.5 | 0.119 |
| Serum albumin (g/dL) | 3.4–5.4 | 4.1 ± 0.5 | 4.0 ± 0.3 | 3.2 ± 0.3 | 2.6 ± 0.6 | <0.001 |
| Serum glucose (mmol/L) | 60–125 | 92 ± 10.8 | 93 ± 10.3 | 96 ± 9.5 | 101 ± 11.4 | 0.009 |
| eGFR (mL/min/1.73 m2) | >60 | 73.2 ± 5.4 | 70.4 ± 6.1 | 62.8 ± 5.9 | 56.9 ± 7.3 | <0.001 |
| D-Dimers (µg/mL) | <0.5 | 1.3 ± 0.4 | 2.2 ± 0.6 | 3.7 ± 1.0 | 7.4 ± 2.1 | <0.001 |
| Procalcitionin (µg/L) | <0.1 | 0.2 ± 0.1 | 0.4 ± 0.1 | 0.8 ± 0.2 | 1.3 ± 0.2 | <0.001 |
| BNP (pg/mL) | <100 | 241 ± 47 | 308 ± 66 | 559 ± 84 | 1572 ± 146 | <0.001 |
| CK-MB (U/L) | 5–25 | 22 ± 4.1 | 24 ± 4.7 | 29 ± 4.9 | 38 ± 6.2 | <0.001 |
| Myoglobin (nmol/L) | 1.2–3.6 | 1.4 ± 0.2 | 1.9 ± 0.3 | 3.1 ± 0.6 | 4.7 ± 0.9 | <0.001 |
| Troponin I (ng/mL) | 0–0.4 | 0.1 ± 0.1 | 0.2 ± 0.1 | 0.3 ± 0.1 | 0.6 ± 0.2 | <0.001 |
| Troponin T (ng/mL) | <14 | 11 ± 1.3 | 14 ± 1.5 | 22 ± 1.9 | 25 ± 2.7 | <0.001 |
| LDH (U/L) | 140–280 | 204 ± 28 | 261 ± 33 | 288 ± 37 | 341 ± 41 | <0.001 |
| Factors | Mortality OR (95% CI) | p-Value | Rehospitalization OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age (>65) | 2.07 (1.44–3.01) | 0.008 | 2.64 (1.82–3.97) | 0.004 |
| Cardiovascular risk factors (>2) | 2.35 (2.01–2.94) | 0.002 | 3.09 (1.96–5.44) | 0.001 |
| Severe COVID-19 | 2.92 (1.26–4.05) | 0.001 | 3.35 (2.14–5.83) | <0.001 |
| Invasive ventilation | 3.04 (1.59–4.71) | <0.001 | 3.88 (2.43–6.08) | <0.001 |
| Severe in-hospital complications | 4.38 (3.01–5.64) | <0.001 | 4.92 (2.58–6.67) | <0.001 |
| ICU admission | 3.42 (2.01–4.66) | <0.001 | 5.19 (2.26–6.08) | <0.001 |
| Left ventricle ejection fraction (<30%) | 1.89 (1.16–3.07) | 0.036 | 3.07 (2.19–4.86) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citu, I.M.; Citu, C.; Gorun, F.; Neamtu, R.; Motoc, A.; Burlea, B.; Rosca, O.; Bratosin, F.; Hosin, S.; Manolescu, D.; et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. J. Clin. Med. 2022, 11, 1382. https://doi.org/10.3390/jcm11051382
Citu IM, Citu C, Gorun F, Neamtu R, Motoc A, Burlea B, Rosca O, Bratosin F, Hosin S, Manolescu D, et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. Journal of Clinical Medicine. 2022; 11(5):1382. https://doi.org/10.3390/jcm11051382
Chicago/Turabian StyleCitu, Ioana Mihaela, Cosmin Citu, Florin Gorun, Radu Neamtu, Andrei Motoc, Bogdan Burlea, Ovidiu Rosca, Felix Bratosin, Samer Hosin, Diana Manolescu, and et al. 2022. "Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19" Journal of Clinical Medicine 11, no. 5: 1382. https://doi.org/10.3390/jcm11051382