
Morphology and Vessel Density of the Macula in Preterm Children Using Optical Coherence Tomography Angiography

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
3. Statistical Analysis
4. Results
4.1. Macular Hypoplasia
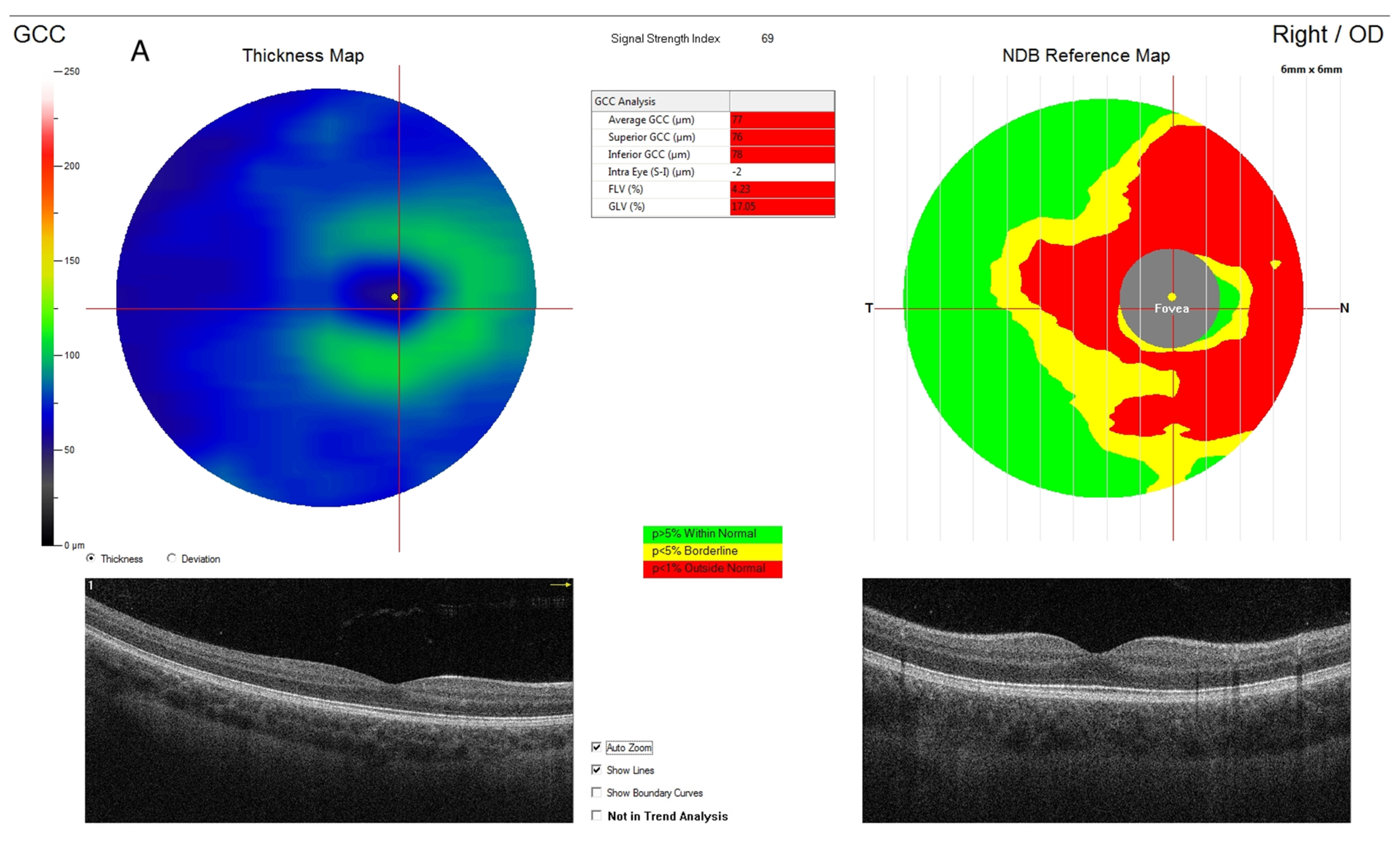
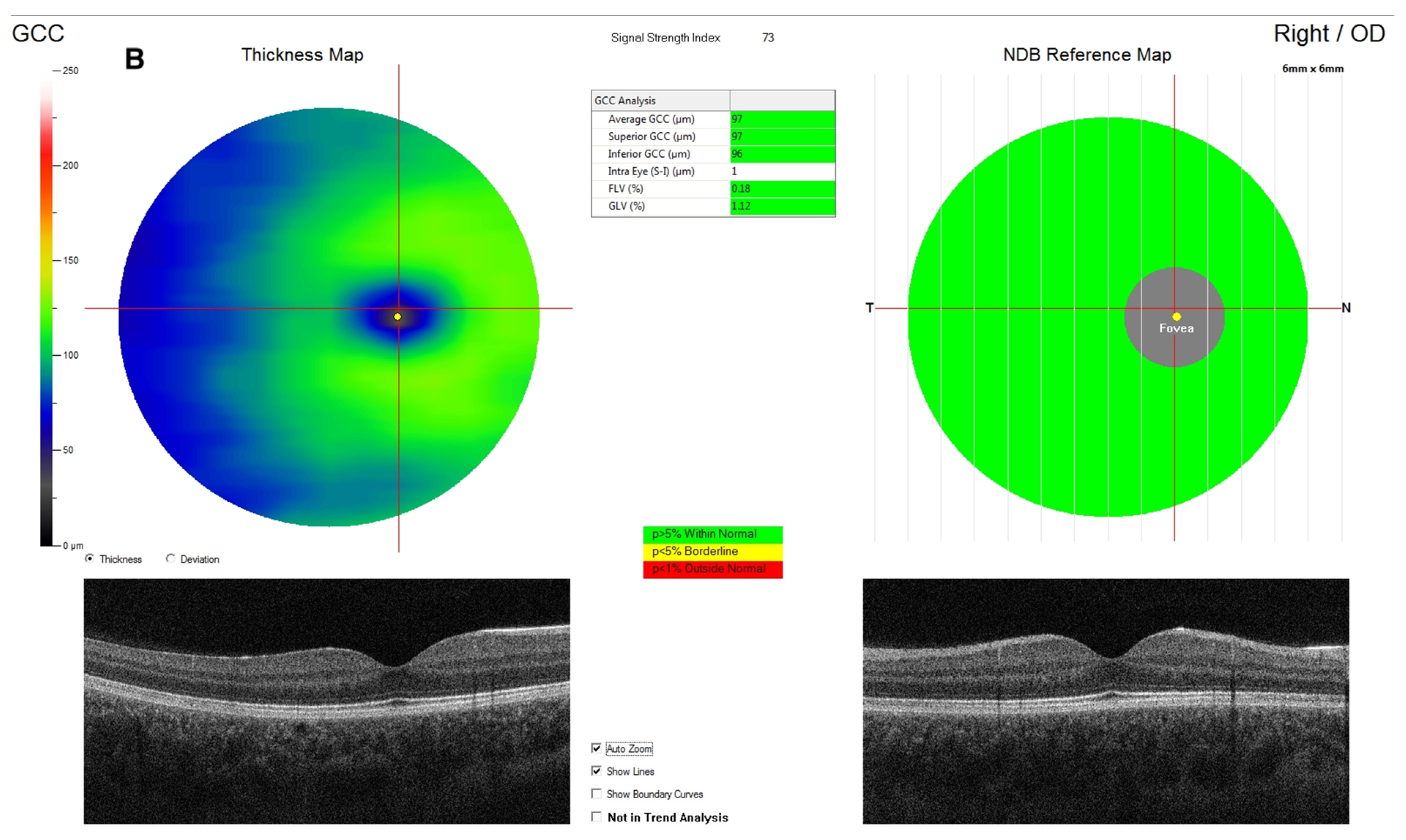
4.2. Ganglion Cell Complex
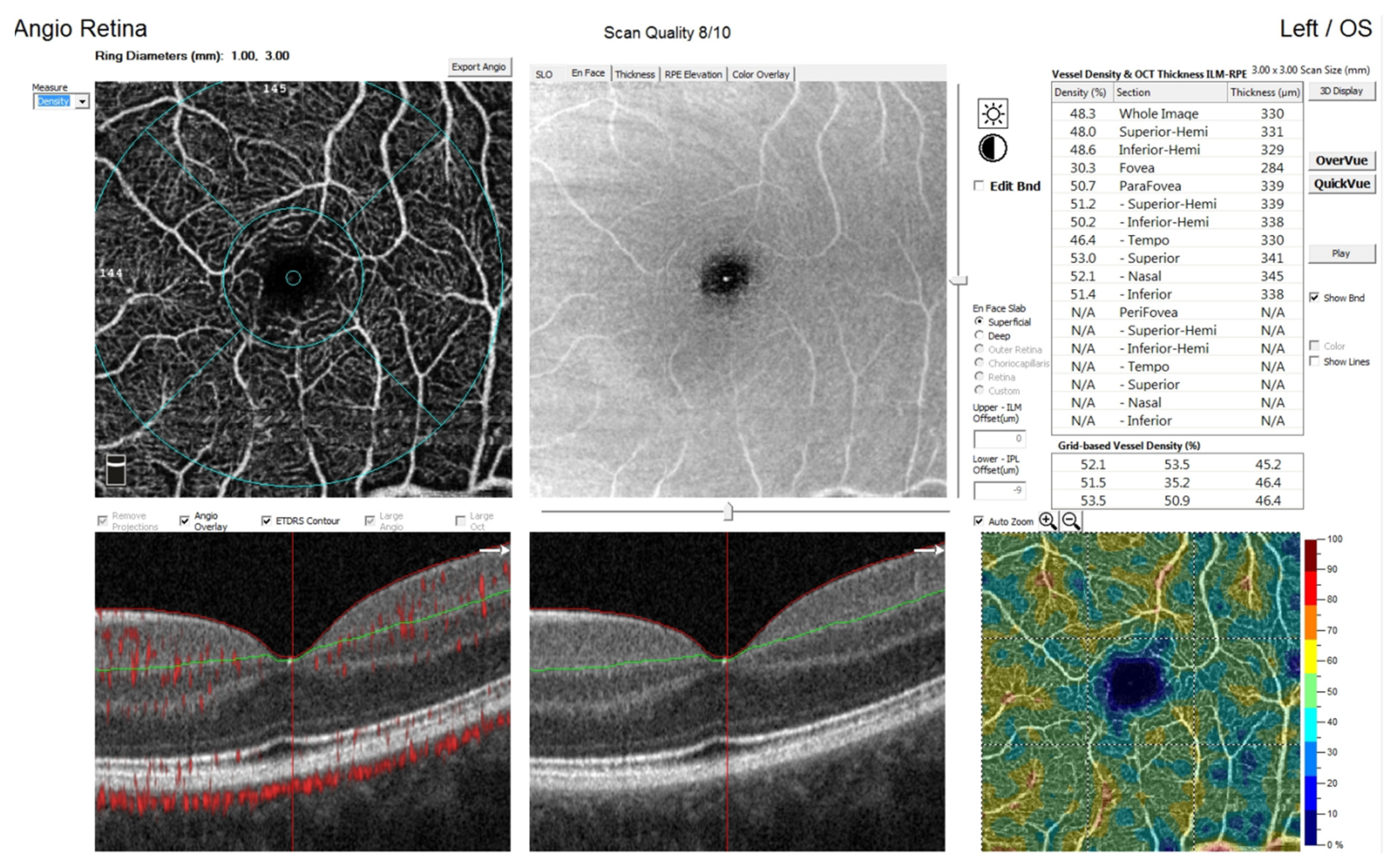
4.3. Vessel Density
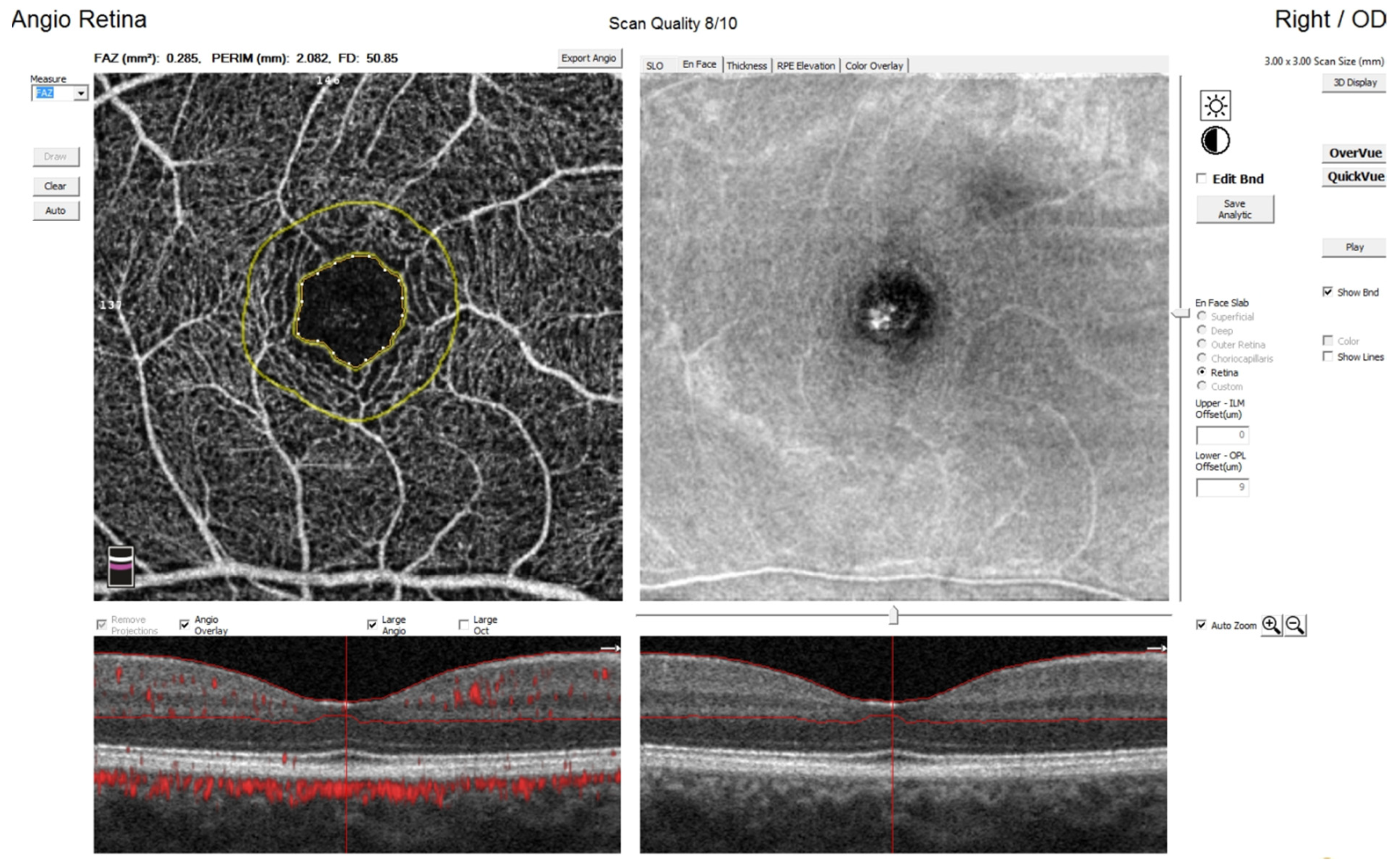
4.4. Foveal Avascular Zone
4.5. Retinal and Choroidal Thickness
4.6. The Influence of Stage of Retinopathy and Laser Treatment on OCT and OCTA Parameters
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, J.; Wu, Z.; Lam, W.; Yang, M.; Chen, L.; Zheng, L.; Zhang, F.; Zeng, J.; Wang, J.; Zhang, G. Comparison of OCT angiography in children with a history of intravitreal injection of ranibizumab versus laser photocoagulation for retinopathy of prematurity. Br. J. Ophthalmol. 2020, 104, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Borrelli, E.; Lonngi, M.; Velez, F.; Sarraf, D.; Sadda, S.R.; Tsui, I. Visual Function and Optical Coherence Tomography Angiography Features in Children Born Preterm. Retina 2019, 39, 2233–2239. [Google Scholar] [CrossRef] [PubMed]
- Falavarjani, K.G.; Iafe, N.A.; Velez, F.G.; Schwartz, S.D.; Sadda, S.R.; Sarraf, D.; Tsui, I. Optical Coherence Tomography Angiography of the Fovea in Children Born Preterm. Retina 2017, 37, 2289–2294. [Google Scholar] [CrossRef]
- Gole, G.A.; Ells, A.L.; Katz, X.; Holmstrom, G.; Fielder, A.R.; Capone, A.; Flynn, J.T.; Good, W.G.; Holmes, J.M.; McNamara, J.A.; et al. The International Classification of Retinopathy of Prematurity Revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Early Treatment for Retinopathy of Prematurity Cooperative Group. Revised indications for the treatment of retinopathy of prematurity: Results of the early treatment for retinopathy of prematurity randomized trial. Arch. Ophthalmol. 2003, 121, 168494, Clinical Trial. [Google Scholar] [CrossRef] [Green Version]
- Takagi, M.; Maruko, I.; Yamaguchi, A.; Kakehashi, M.; Hasegawa, T.; Iida, T. Foveal abnormalities determined by optical coherence tomography angiography in children with history of retinopathy of prematurity. Eye 2019, 33, 1890–1896. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Chang, S.H.L.; Wu, S.-C.; See, L.-C.; Yang, M.-L.; Wu, W.-C. The inner retinal structures of the eyes of children with a history of retinopathy of prematurity. Eye 2017, 32, 104–112. [Google Scholar] [CrossRef]
- Stoica, F.; Chirita-Emandi, A.; Andreescu, N.; Stanciu, A.; Zimbru, C.-G.; Puiu, M. Clinical relevance of retinal structure in children with laser-treated retinopathy of prematurity versus controls—Using optical coherence tomography. Acta Ophthalmol. 2017, 96, e222–e228. [Google Scholar] [CrossRef]
- Wu, W.-C.; Shih, C.-P.; Wang, N.-K.; Lien, R.; Chen, Y.-P.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C.; et al. Choroidal Thickness in Patients with a History of Retinopathy of Prematurity. JAMA Ophthalmol. 2013, 131, 1451–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garey, L.J. Structural development of the visual system of man. Hum. Neurobiol. 1984, 3, 75–80. [Google Scholar]
- Yuodelis, C.; Hendrickson, A. A qualitative and quantitative analysis of the human fovea during development. Vis. Res. 1986, 26, 847–855. [Google Scholar] [CrossRef]
- Hendrickson, A.E.; Yuodelis, C. The Morphological Development of the Human Fovea. Ophthalmology 1984, 91, 603–612. [Google Scholar] [CrossRef]
- Cabrera, M.T.; Maldonado, R.; Toth, C.A.; O’Connell, R.V.; Chen, B.B.; Chiu, S.J.; Farsiu, S.; Wallace, D.K.; Stinnett, S.S.; Panayotti, G.M.M.; et al. Subfoveal Fluid in Healthy Full-term Newborns Observed by Handheld Spectral-Domain Optical Coherence Tomography. Am. J. Ophthalmol. 2012, 153, 167–175.e3. [Google Scholar] [CrossRef] [Green Version]
- Gołębiewska, J.; Olechowski, A.; Wysocka-Mincewicz, M.; Odrobina, D.; Baszyńska-Wilk, M.; Groszek, A.; Szalecki, M.; Hautz, W. Optical coherence tomography angiography vessel density in children with type 1 diabetes. PLoS ONE 2017, 12, e0186479. [Google Scholar] [CrossRef] [PubMed]
- Vinekar, A.; Sinha, S.; Mangalesh, S.; Jayadev, C.; Shetty, B. Optical coherence tomography angiography in preterm-born children with retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 2131–2137. [Google Scholar] [CrossRef]
- Nonobe, N.; Kaneko, H.; Ito, Y.; Takayama, K.; Kataoka, K.; Tsunekawa, T.; Matsuura, T.; Suzumura, A.; Shimizu, H.; Terasaki, H. Optical Coherence Tomography Angiography of the Foveal Avascular Zone in Children with a History of Treatment-Requiring Retinopathy of Prematurity. Retina 2019, 39, 111–117. [Google Scholar] [CrossRef]
- Rogowska, A.; Obrycki, Ł.; Kułaga, Z.; Kowalewska, C.; Litwin, M. Remodeling of Retinal Microcirculation is Associated with Subclinical Arterial Injury in Hypertensive Children. Hypertension 2021, 77, 1203–1211. [Google Scholar] [CrossRef]
- Akbari, M.; Abdi, P.; Fard, M.A.; Afzali, M.; Ameri, A.; Yazdani-Abyaneh, A.; Mohammadi, M.; Moghimi, S. Retinal Ganglion Cell Loss Precedes Retinal Nerve Fiber Thinning in Nonarteritic Anterior Ischemic Optic Neuropathy. J. Neuro-Ophthalmol. 2016, 36, 141–146. [Google Scholar] [CrossRef]
- Zivkovic, M.; Dayanir, V.; Zlatanovic, M.; Zlatanovic, G.; Jaksic, V.; Jovanovic, P.; Radenkovic, M.; Djordjevic-Jocic, J.; Stankovic-Babic, G.; Jovanovic, S. Ganglion Cell-Inner Plexiform Layer Thickness in Different Glaucoma Stages Measured by Optical Coherence Tomography. Ophthalmic Res. 2018, 59, 148–154. [Google Scholar] [CrossRef]
- Kaur, C.; Foulds, W.S.; Ling, E.-A. Hypoxia-ischemia and retinal ganglion cell damage. Clin. Ophthalmol. 2008, 2, 879–889. [Google Scholar] [CrossRef] [Green Version]
- Hellström, A.; Smith, L.E.; Dammann, O. Retinopathy of prematurity. Lancet 2013, 382, 1445–1457. [Google Scholar] [CrossRef] [Green Version]
- Pueyo, V.; González, I.; Altemir, I.; Pérez, T.; Gómez, G.; Prieto, E.; Oros, D. Microstructural Changes in the Retina Related to Prematurity. Am. J. Ophthalmol. 2015, 159, 797–802. [Google Scholar] [CrossRef]
- Miki, A.; Yamada, Y.; Nakamura, M. The Size of the Foveal Avascular Zone Is Associated with Foveal Thickness and Structure in Premature Children. J. Ophthalmol. 2019, 2019, 8340729. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.F.; Ramasamy, B.; Lythgoe, D.T.; Clark, D. Choroidal thickness in regressed retinopathy of prematurity. Eye 2014, 28, 1461–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.A.; Oh, S.Y. Analysis of spectral-domain optical coherence tomography in preterm children: Retinal layer thickness and choroidal thickness profiles. Investig. Ophthalmol. Vis. Sci. 2012, 53, 7201–7207. [Google Scholar] [CrossRef] [Green Version]
- Wangsa-Wirawan, N.D.; Linsenmeier, R.A. Retinal oxygen: Fundamental and clinical aspects. Arch. Ophthalmol. 2003, 121, 547–557. [Google Scholar] [CrossRef]
- Wang, J.; Spencer, R.; Leffler, J.N.; Birch, E.E. Critical Period for Foveal Fine Structure in Children with Regressed Retinopathy of Prematurity. Retina 2012, 32, 330–339. [Google Scholar] [CrossRef]
- Provis, J.M. Development of the Primate Retinal Vasculature. Prog. Retin. Eye Res. 2001, 20, 799–821. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Chen, Y.-T.; Chen, S.-N. Foveal microvascular anomalies on optical coherence tomography angiography and the correlation with foveal thickness and visual acuity in retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 23–30. [Google Scholar] [CrossRef]
- Miki, A.; Honda, S.; Inoue, Y.; Yamada, Y.; Nakamura, M. Foveal Depression and Related Factors in Patients with a History of Retinopathy of Prematurity. Ophthalmologica 2018, 240, 106–110. [Google Scholar] [CrossRef]
- Rezar-Dreindl, S.; Eibenberger, K.; Told, R.; Neumayer, T.; Steiner, I.; Sacu, S.; Schmidt-Erfurth, U.; Stifter, E. Retinal vessel architecture in retinopathy of prematurity and healthy controls using swept-source optical coherence tomography angiography. Acta Ophthalmol. 2021, 99, e232–e239. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics Committee on Fetus and Newborn. American College of obstetricians and gynecologists committee on obstetric practice. The Apgar Score. Pediatrics 2015, 136, 819–822. [Google Scholar] [CrossRef] [Green Version]
- Sacchi, C.; Marino, C.; Nosarti, C.; Vieno, A.; Visentin, S.; Simonelli, A. Association of Intrauterine Growth Restriction and Small for Gestational Age Status with Childhood Cognitive Outcomes: A systematic review and meta-analysis. JAMA Pediatr. 2020, 174, 772–781. [Google Scholar] [CrossRef]
- Tan, O.; Chopra, V.; Lu, A.T.-H.; Schuman, J.; Ishikawa, H.; Wollstein, G.; Varma, R.; Huang, D. Detection of Macular Ganglion Cell Loss in Glaucoma by Fourier-Domain Optical Coherence Tomography. Ophthalmology 2009, 116, 2305–2314.e2. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Kumar, A.; Mohammad, S.; Proudlock, F.A.; Engle, E.C.; Andrews, C.; Chan, W.-M.; Thomas, S.; Gottlob, I. Structural Grading of Foveal Hypoplasia Using Spectral-Domain Optical Coherence Tomography: A Predictor of Visual Acuity? Ophthalmology 2011, 118, 1653–1660. [Google Scholar] [CrossRef] [Green Version]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K. Image artifacts in optical coherence tomography angiography. Retina 2015, 35, 2163–2180. [Google Scholar] [CrossRef]
- Rosén, R.M.; Hellgren, K.M.; Venkataraman, A.P.; Vicent, A.D.; Nilsson, M. Increased foveal ganglion cell and inner plexiform layer thickness in children aged 6.5 years born extremely preterm. Retina 2020, 40, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Yanni, S.E.; Wang, J.; Chan, M.; Carroll, J.; Farsiu, S.; Leffler, J.N.; Spencer, R.; Birch, E.E. Foveal avascular zone and foveal pit formation after preterm birth. Br. J. Ophthalmol. 2012, 96, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Darlow, B.A.; Hutchinson, J.L.; Henderson-Smart, D.J.; Donoghue, D.A.; Simpson, J.M.; Evans, N.J. Prenatal Risk Factors for Severe Retinopathy of Prematurity among Very Preterm Infants of the Australian and New Zealand Neonatal Network. Pediatrics 2005, 115, 990–996. [Google Scholar] [CrossRef]
- Shah, V.A.; Yeo, C.L.; Ling, Y.L.F.; Ho, L.Y. Incidence, risk factors of retinopathy of prematurity among very low birth weight infants in Singapore. Ann. Acad. Med. Singap. 2005, 34, 169–178. [Google Scholar]
- Allegaert, K.; De Coen, K.; Devlieger, H. Threshold retinopathy at threshold of viability: The EpiBel study. Br. J. Ophthalmol. 2004, 88, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, Y.J.; Hong, K.E.; Yum, H.R.; Lee, J.H.; Kim, K.S.; Youn, Y.A.; Park, S.H. Characteristic clinical features associated with aggressive posterior retinopathy of prematurity. Eye 2017, 31, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.-H.; Jin, J.; Yuan, T.-M.; Yu, H.-M. Risk Factors and Outcomes for Retinopathy of Prematurity in Neonatal Infants with a Birth Weight of 1501–2000 g in a Chinese Neonatal Unit. Med Princ. Pract. 2011, 20, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Magrath, G.N.; Say, E.A.T.; Sioufi, K.; Ferenczy, S.; Samara, W.A.; Shields, C.L. Variability in foveal avascular zone and capillary density using optical coherence tomography angiography machines in healthy eyes. Retina 2017, 37, 2102–2111. [Google Scholar] [CrossRef]
- Hughes, S.; Yang, H.; Chan-Ling, T. Vascularization of the human fetal retina: Roles (39) of vasculogenesis and angiogenesis. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1217–1228. [Google Scholar]
- Carpineto, P.; Mastropasqua, R.; Marchini, G.; Toto, L.; Di Nicola, M.; Di Antonio, L. Reproducibility and repeatability of foveal avascular zone measurements in healthy subjects by optical coherence tomography angiography. Br. J. Ophthalmol. 2016, 100, 671–676. [Google Scholar] [CrossRef]
- Mintz-Hittner, H.A.; Knight-Nanan, D.M.; Satriano, D.R.; Kretzer, F.L. A small foveal avascular zone may be an historic mark of prematurity. Ophthalmology 1999, 106, 1409–1413. [Google Scholar] [CrossRef]
- Hartnett, M.E. Retinopathy of Prematurity: Evolving Treatment with Anti–Vascular Endothelial Growth Factor. Am. J. Ophthalmol. 2020, 218, 208–213. [Google Scholar] [CrossRef]
- Celiker, H.; Sahin, O. Angiographic findings in cases with a history of severe retinopathy of prematurity treated with anti-VEGFs: Follow-up to age 6 years. Int. Ophthalmol. 2021, 1–21. [Google Scholar] [CrossRef]
- Houston, S.K.; Wykoff, C.C.; Berrocal, A.M.; Hess, D.J.; Murray, T.G. Laser treatment for retinopathy of prematurity. Lasers Med Sci. 2013, 28, 683–692. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Number (%) or Median (IQR) |
|---|---|
| Preterm children | 123 |
| Males | 66 (53.66%) |
| Age (years) | 10.58 (8.12–12.77) |
| Birth weight (g) | 1350 (930–1678) |
| Birth weight < 1500 g | 75 (62.5%) |
| IUGR | 14 (11.38%) |
| Gestational Age (weeks) | 29 (27–32) |
| Gestational Age < 28 weeks | 35 (28.46%) |
| Apgar score | |
| 0–3 | 23 (18.7%) |
| 4–7 | 67 (54.47%) |
| 8–10 | 22 (17.89%) |
| Lack of data | 11 (8.94%) |
| Ophthalmic characteristics | |
| Parameter | Number of eyes (%) |
| No ROP | 85 (34.55%) |
| ROP | 129 (52.44%) |
| ROP 1 stage | 9 (6.98%) |
| ROP 2 stage | 57 (44.19%) |
| ROP 3 stage | 63 (48.83%) |
| Lack of ROP data | 32 (13.01%) |
| Plus disease | 47 (36.43%) |
| ROP with treatment | 70 (54.26%) |
| Visual Acuity (logMAR) | 0 (0.22–0) |
| Refractive error (Dioptres) | 1.0 (−0.75–2.27) |
| Macular hypoplasia | 56 (24.77%) |
| Lack of data | 20 |
| Variable | Preterm Children | N | Healthy Control | N | p-Value |
|---|---|---|---|---|---|
| Average GCC (μm) | 93 (86–100) | 203 | 100 (96–103) | 165 | <0.001 |
| GCC superior quandrant | 92 (85–98) | 203 | 99 (94–104) | 165 | <0.001 |
| GCC inferior quadrant | 93 (87–101) | 203 | 100 (96–104) | 165 | <0.001 |
| CCT (μm) | 312 (250–360) | 179 | 337.5 (280–381) | 130 | 0.005 |
| FAZ (μm2) | 0.13 (0.07–0.19) | 106 | 0.23 (0.17–0.3) | 133 | <0.001 |
| wsVD | 45.2 (41.7–48) | 106 | 48.7(47–50.3) | 133 | <0.001 |
| wsVD superior quadrant | 45.1 (41.8–47.6) | 106 | 48.7(47–50.2) | 133 | <0.001 |
| wsVD inferior quadrant | 45.5 (42.1–48.2) | 106 | 49.2 (46.9–50.5) | 133 | <0.001 |
| fsVD | 24.95(19.4–31.7) | 106 | 23.9 (19.7–28.7) | 133 | 0.398 |
| psVD | 47.75 (43.8–50.1) | 106 | 51.4 (49.7–53) | 133 | <0.001 |
| psVD superior quadrant | 47.7 (43.7–50.4) | 106 | 51.4 (49.6–53.3) | 133 | <0.001 |
| psVD inferior quadrant | 48.05 (49.3–50.3) | 106 | 51.7 (49.5–53.3) | 133 | <0.001 |
| wdVD | 49.8 (47–52.3) | 106 | 49.8 (46.5–52.7) | 133 | 0.707 |
| wdVD superior quadrant | 50.1 (47.7–52.2) | 106 | 49.8 (46.5–52.7) | 133 | 0.644 |
| wdVD inferior quadrant | 49.35 (46.6–52.2) | 106 | 49.5 (46.4 −52) | 133 | 0.793 |
| fdVD | 41.9 (36.6–46.4) | 106 | 36.9 (51.5–41.5) | 133 | <0.001 |
| pfdVD | 50.8 (48.4–53.7) | 106 | 51.4 (48.9–54.0) | 133 | 0.522 |
| pdVD superior quandrant | 51.6 (48.4–54) | 106 | 51.15 (47.75–53.85) | 133 | 0.706 |
| pdVD Inferior quadrant | 50.5 (47.9–53.8) | 106 | 51.4 (48.5–54.1) | 133 | 0.454 |
| WT (μm) | 310.5 (303–326) | 106 | 321 (312–329,5) | 133 | <0.001 |
| WT superior quadrant (μm) | 313.5 (303–329) | 106 | 323.5 (313–331) | 133 | <0.001 |
| WT inferior quadrant (μm) | 310 (303–325) | 106 | 319.5 (311–329) | 133 | <0.001 |
| FT (μm) | 274.5 (257–298) | 106 | 252 (242–268) | 133 | <0.001 |
| PFT (μm) | 318.5 (312–336) | 106 | 331 (322–339) | 133 | <0.001 |
| PFT superior quadrant (μm) | 320.5 (311–336) | 106 | 331 (322–339) | 133 | <0.001 |
| PFT inferior quadrant (μm) | 319 (312–335) | 106 | 329.5 (321–338) | 133 | <0.001 |
| Gestational Age (Weeks) | Birth Weight (Grams) | Apgar Score (Points) | IUGR | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Weeks | Median (IQR) | p-Value | Weight | Median (IQR) | p-Value | Apgar Score | Median (IQR) | p-Value | IUGR | Median (IQR) | ||
| Avg GCC (μm) | <28 N = 47 | 96 (87–103) | 0.059 | <1500 N = 114 | 93 (87–100) | 0.522 | <4 N = 32 | 89.5 (82–93) | 0.003 | Yes N = 25 | 89 (80–93) | 0.044 |
| ≥28 N = 156 | 92 (86–98) | ≥1500 N = 83 | 93 (86–98) | ≥4 N = 150 | 95 (88–100) | No N = 174 | 94 (87–100) | |||||
| FAZ (μm2) | <28 N = 18 | 0.08 (0.04–0.15) | 0.026 | <1500 N = 55 | 0.08 (0.05–0.14) | <0.001 | <4 N = 15 | 0.13 (0.05–0.19) | 0.975 | Yes N = 19 | 0.106 (0.074–0.208) | 0.796 |
| ≥28 N = 88 | 0.14 (0.07–0.2) | ≥1500 N = 45 | 0.1 (0.14–0.25) | ≥4 N = 80 | 0.1 (0.07–0.18) | No N = 83 | 0.141 (0.067–0.197) | |||||
| wsVD (%) | <28 | 44.65 (38.3–48.5) | 0.604 | <1500 | 44.6 (40.3–47.6) | 0.116 | <4 | 42.3 (38.8–46.1) | 0.046 | Yes N = 19 | 44 (40.4–45.3) | 0.057 |
| ≥28 | 45.25 (42.6–47.9) | ≥1500 | 46.2 (43.2–48) | ≥4 | 49.3 (46.5–51.95) | No N = 83 | 45.6 (42.3–48.1) | |||||
| fsVD (%) | <28 | 30 (23.5–32.8) | 0.059 | <1500 | 26 (21.5–32.8) | <0.001 | <4 | 23.1 (16.4–32.2) | 0.571 | Yes N = 19 | 22.2 (16–27) | 0.184 |
| ≥28 | 24.15 (18.35–30.3) | ≥1500 | 21.5 (16.3–27.4) | ≥4 | 42.25 (36.8–47.05) | No N = 83 | 25 (19,4–31,6) | |||||
| psVD (%) | <28 | 45.55 (38.6–50.1) | 0.222 | <1500 | 46.5 (42–49.1) | 0.011 | <4 | 45.2 (40–48.7) | 0,060 | Yes N = 19 | 47 (43.4–48.7) | 0.220 |
| ≥28 | 47.95 (44.5–50.2) | >1500 | 49 (46.2–50.3) | ≥4 | 47.45 (44.35–50.35) | No N = 83 | 48.5 (44.3–50.3) | |||||
| WT (μm) | <28 | 326.5 (318–347) | <0.001 | <1500 | 317 (302–322) | 0.231 | <4 | 312 (295–344) | 0.543 | Yes N = 19 | 304 (296–318) | 0.052 |
| ≥28 | 308.5 (302–324) | ≥1500 | 317 (302–332) | ≥4 | 31 (306–328) | No N = 83 | 316 (304–329) | |||||
| FT (μm) | <28 | 314 (273–329) | <0.001 | <1500 | 293 (266–315) | <0.001 | <4 | 281 (262–308) | 0.431 | Yes N = 19 | 273 (256–287) | 0.397 |
| ≥28 | 271 (256–288) | ≥1500 | 257 (252–278) | ≥4 | 274.5 (257–298) | No N = 83 | 277 (256–300) | |||||
| PFT (μm) | <28 | 334.5 (323–355) | 0.002 | <1500 | 323 (310–339) | 0.24 | <4 | 318 (302–350) | 0.446 | Yes N = 19 | 314 (304–330) | 0.117 |
| ≥28 | 317.5 (310–332) | ≥1500 | 323 (310–339) | ≥4 | 322.5 (316–336.5) | No N = 83 | 323 (313–338) | |||||
| wdVD (%) | <28 | 48.7 (45.6–50.9) | 0.292 | <1500 | 49.3 (46.4–52.2) | 0.526 | <4 | 50.4 (47.5–54.3) | 0.226 | Yes N = 19 | 50 (48.8–54.2) | 0.470 |
| ≥28 | 50 (47.45–52.5) | ≥1500 | 50.1 (47.5–52,5) | ≥4 | 49.3 (46.5–51.95) | No N = 83 | 49.4 (46.7–52.3) | |||||
| fdVD (%) | <28 | 43.4 (40.3–49) | 0.064 | <1500 | 43.4 (40.3–48.9) | <0.001 | <4 | 40,4 (35–48.4) | 0.578 | Yes N = 19 | 41.6 (32.9–44.7) | 0.367 |
| ≥28 | 41.65 (35.55–45.65) | ≥1500 | 38.7 (32.9–43.8) | ≥4 | 42.25 (36.8–47.05) | No N = 83 | 42.2 (36.6–47) | |||||
| pdVD (%) | <28 | 49.65 (47–52.6) | 0.209 | <1500 | 50.1 (47.2–53.6) | 0.124 | <4 | 52.6 (49.7–55.5) | 0.101 | Yes N = 19 | 51.6 (50–55.5) | 0.359 |
| ≥28 | 41.6 (48.5–54.15) | ≥1500 | 51.7 (49.3–54.4) | ≥4 | 50.3 (48.25–53.3) | No N = 83 | 50.4 (48.4–53.6) | |||||
| Gestational Age | Birth Weight | |||||
|---|---|---|---|---|---|---|
| Parameter | N | R Spearman | p-Value | N | R Spearman | p-Value |
| AvgGCC | 203 | −0.085 | 0.228 | 199 | −0.054 | 0.446 |
| wsVD | 106 | 0.051 | 0.604 | 102 | 0.195 | 0.049 |
| fsVD | 106 | −0.376 | <0.001 | 102 | −0.306 | <0.001 |
| psVD | 106 | 0.184 | 0.059 | 102 | 0.298 | 0.002 |
| wdVD | 106 | −0.451 | 0.645 | 102 | 0.013 | 0.898 |
| fdVD | 106 | −0.444 | <0.001 | 102 | −0.339 | <0.001 |
| pdVD | 106 | 0.044 | 0.065 | 102 | 0.089 | 0.372 |
| FAZ | 106 | 0.456 | <0.001 | 102 | 0.472 | <0.001 |
| WF | 106 | −0.389 | <0.001 | 102 | −0.186 | 0.06 |
| FT | 106 | −0.562 | <0.001 | 102 | −0.508 | <0.001 |
| PFT | 106 | 0.465 | <0.001 | 102 | −0.185 | 0.063 |
| Group 0 without ROP | Group 1 ROP without Treatment | Group 2 –Severe ROP Requiring Treatment | p-Value for Overall Kruskal–Wallis Test | p-Value Group 0 vs. Group 1 | p-Value Group 0 vs. Group 2 | p-Value Group 1 vs. Group 2 | |
|---|---|---|---|---|---|---|---|
| GCC | N = 85 | N = 57 | N = 41 | ||||
| Avg GCC | 93 (87–98) | 91 (84–95) | 100 (92–105) | <0.001 | 0.272 | 0.006 | <0.001 |
| OCT Angiography | N = 50 | N = 21 | N = 18 | ||||
| FAZ (μm2) | 0.16 (0.11–0.2) | 0.09 (0.06–0.13) | 0,09 (0.04–0.13) | 0.003 | 0.046 | 0.009 | 1.0 |
| wsVD | 46 (43.2–48.1) | 44.7 (50.5–48.2) | 41.7 (38.3–45.4) | 0.027 | 1.0 | 0.022 | 0.361 |
| fsVD | 22.1 (16.3–26.7) | 26.2 (21–31.7) | 31.55 21.5–33.7) | 0.009 | 0.113 | 0.017 | 1.0 |
| psVD | 49.05 (46.4–50.9) | 47.4 (41.5–50.3) | 44.25 (38.6–47.5) | 0.002 | 0.288 | 0.002 | 0.338 |
| WT | 310.5 (304–325) | 307 (302–324) | 325 (300–347) | 0.187 | 1.0 | 0.339 | 0.261 |
| FT | 261.5 (255–279) | 273 (257–298) | 307 (290–321) | <0.001 | 0.442 | <0.001 | 0.017 |
| PFT (μm) | 51.4 (48.6–54.8) | 316 310–332) | 332.5 (307–355) | 0.250 | 1.0 | 0.688 | 0.296 |
| wdPD | 50.5 (47.4–52.3) | 49.2 (46.6–52.2) | 48.55 (45.9–52.2) | 0.823 | 1.0 | 1.0 | 1.0 |
| fdVD | 40.2 (39.2–42.9) | 44.3 (42–47.9) | 42.3 (37–48.9) | 0.004 | 0.009 | 0.073 | 1.0 |
| pdVD | 51.4 (48.6–54.8) | 50.1 (47.8–53) | 49.65 (47–55.4) | 0.476 | 1.0 | 0.869 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czeszyk, A.; Hautz, W.; Jaworski, M.; Bulsiewicz, D.; Czech-Kowalska, J. Morphology and Vessel Density of the Macula in Preterm Children Using Optical Coherence Tomography Angiography. J. Clin. Med. 2022, 11, 1337. https://doi.org/10.3390/jcm11051337
Czeszyk A, Hautz W, Jaworski M, Bulsiewicz D, Czech-Kowalska J. Morphology and Vessel Density of the Macula in Preterm Children Using Optical Coherence Tomography Angiography. Journal of Clinical Medicine. 2022; 11(5):1337. https://doi.org/10.3390/jcm11051337
Chicago/Turabian StyleCzeszyk, Agnieszka, Wojciech Hautz, Maciej Jaworski, Dorota Bulsiewicz, and Justyna Czech-Kowalska. 2022. "Morphology and Vessel Density of the Macula in Preterm Children Using Optical Coherence Tomography Angiography" Journal of Clinical Medicine 11, no. 5: 1337. https://doi.org/10.3390/jcm11051337