
Associated Risk Factors with Low Back Pain in White-Collar Workers—A Cross-Sectional Study


Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Protocol
2.3. Statistics
3. Results
3.1. Demographic and Descriptive Statistics
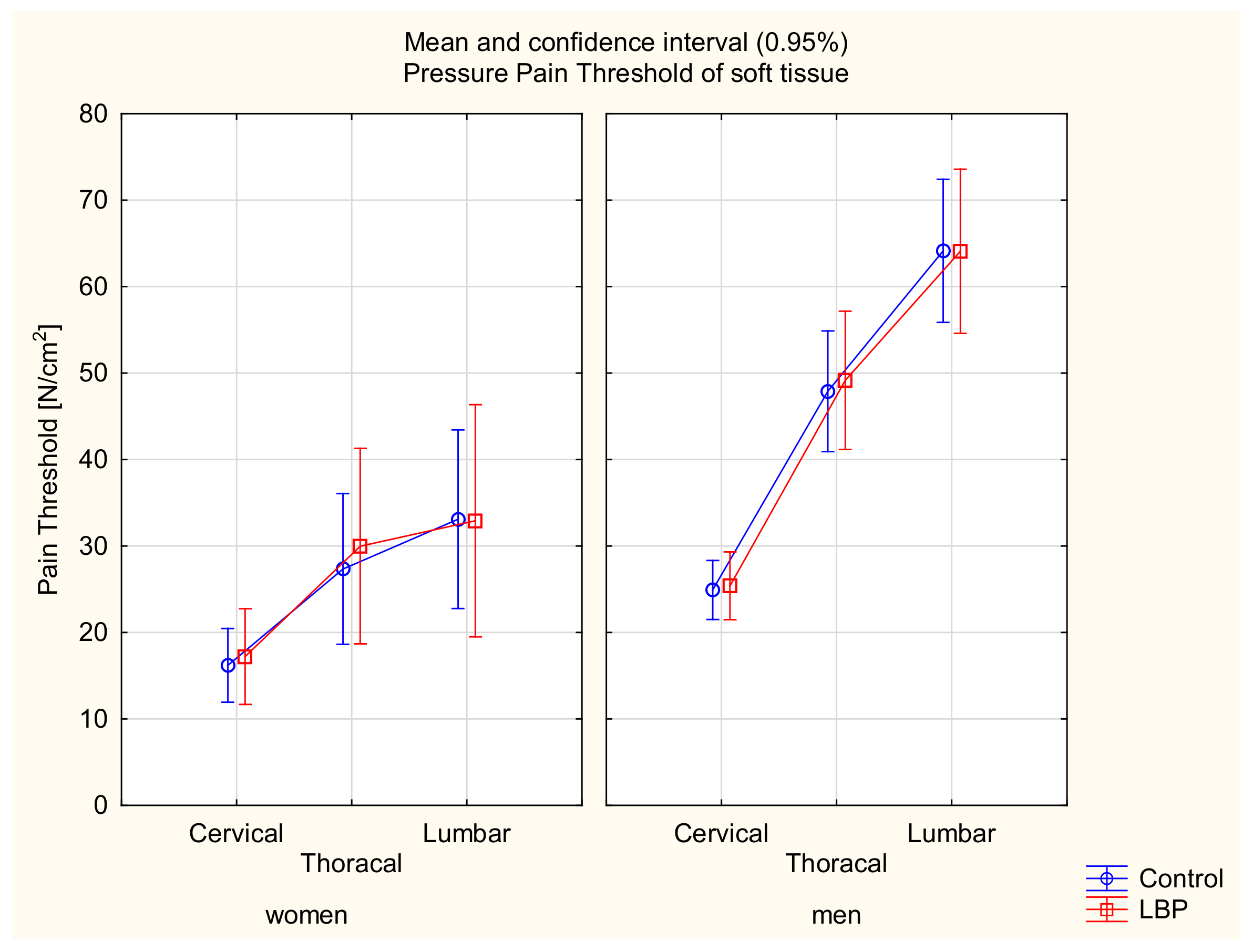
3.2. Pressure Pain Threshold
3.3. Angular Parameters of the Spine Curvatures
3.3.1. ALPHA Angle of the Lumbosacral Spine
3.3.2. BETA Angle of the Thoracolumbar Spine
3.3.3. GAMMA Angle of the Upper Thoracic Spine
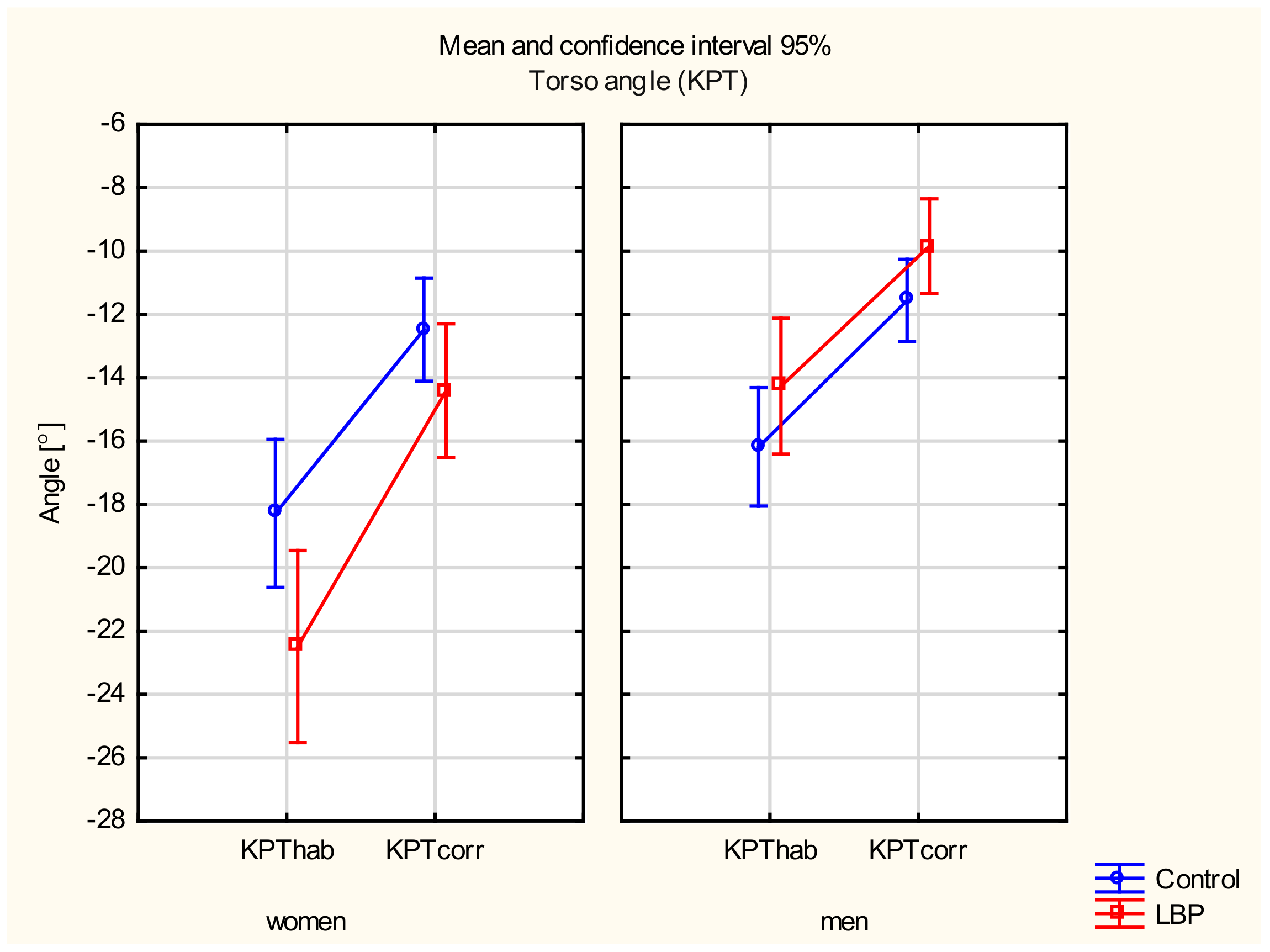
3.3.4. Torso Angle
3.4. The Logistic Regression Model
4. Discussion
4.1. The Pressure Pain Threshold
4.2. Angular Parameters of Spine Curvature
4.3. The Logistic Regression Model
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Garg, A.; Hegmann, K.T.; Moore, J.S.; Kapellusch, J.; Thiese, M.S.; Boda, S.; Bhoyr, P.; Bloswick, D.; Merryweather, A.; Sesek, R.; et al. Study protocol title: A prospective cohort study of low back pain. BMC Musculoskelet. Disorders 2013, 14, 84. [Google Scholar] [CrossRef] [Green Version]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheumatol. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Nicol, A.L.; Adams, M.C.B.; Gordon, D.B.; Mirza, S.; Dickerson, D.; Mackey, S.; Edwards, D.; Hurley, R.W. AAAPT Diagnostic Criteria for Acute Low Back Pain with and Without Lower Extremity Pain. Pain Med. 2020, 21, 2661–2675. [Google Scholar] [CrossRef] [PubMed]
- Notarnicola, A.; Maccagnano, G.; Gallone, M.F.; Mastromauro, L.; Rifino, F.; Pesce, V.; Covelli, I.; Moretti, B. Extracorporeal shockwave therapy versus exercise program in patients with low back pain: Short-term results of a randomised controlled trial. J. Biol. Regul. Homeost. Agents 2018, 32, 385–389. [Google Scholar]
- Beattie, P.F. Current understanding of lumbar intervertebral disc degeneration: A review with emphasis upon etiology, pathophysiology, and lumbar magnetic resonance imaging findings. J. Orthop. Sports Phys. Ther. 2008, 38, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Womersley, L.; May, S. Sitting posture of subjects with postural backache. J. Manip. Physiol. Ther. 2006, 29, 213–218. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Pesce, V.; Tafuri, S.; Leo, N.; Moretti, B. Is the Zumba fitness responsible for low back pain? Musculoskelet. Surg. 2015, 99, 211–216. [Google Scholar] [CrossRef]
- Heneweer, H.; Vanhees, L.; Picavet JS, H. Physical activity and low back pain: A U-shaped relation? Pain 2009, 143, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- D’Amico, M.; Kinel, E.; Roncoletta, P. 3D Quantitative Evaluation of Spine Proprioceptive Percep-tion/Motor Control through Instinctive Self-Correction Maneuver in Healthy Young Subjects’ Posture: An Observational Study. Eur. J. Phys. Rehabil. Med. 2018, 54, 428–439. [Google Scholar] [PubMed]
- Kinel, E.; Roncoletta, P.; Pietrangelo, T.; D’Amico, M. 3D Stereophotogrammetric Quantitative Evalua-tion of Posture and Spine Proprioception in Subacute and Chronic Nonspecific Low Back. Pain. J. Clin. Med. 2022, 11, 546. [Google Scholar] [CrossRef]
- Pinto, S.M.; Cheung, J.P.Y.; Samartzis, D.; Karppinen, J.; Zheng, Y.; Pang, M.Y.C.; Wong, A.Y.L. Dif-ferences in Proprioception Between Young and Middle-Aged Adults With and Without Chronic Low Back Pain. Front. Neurol. 2020, 11, 605787. [Google Scholar] [CrossRef] [PubMed]
- Lis, A.; Black, K.; Korn, H.; Nordin, M. Association between sitting and occupational LBP. Eur. Spine J. 2007, 16, 238–298. [Google Scholar] [CrossRef] [Green Version]
- Mork, P.; Westgaard, R. Back posture and low back muscle activity in female computer workers: A field study. Clin. Biomech. 2009, 24, 169–175. [Google Scholar] [CrossRef]
- Caneiro, J.; O’Sullivan, P.; Burnett, A.; Barach, A.; O’Neil, D.; Tveit, O.; Olafsdottir, K. The influence of different sitting postures on head/neck posture and muscle activity. Man. Ther. 2010, 15, 54–60. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, D.E.; Soave, D.; Ross, K.; Callaghan, J.P. Lumbar spine and pelvic posture between standing and sitting: A radiologic investigation including reliability and repeatability of the lumbar lordosis measure. J. Manip. Physiol. Ther. 2010, 33, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Eguchi, A.; Kobara, K.; Ishida, H. Influence of trunk muscle cocontraction on spinal curvature during sitting for desk work. Electromyogr. Clin. Neurophysiol. 2007, 47, 273–278. [Google Scholar]
- Brink, Y.; Crous, L.C.; Louw, Q.A.; Grimmer-Somers, K.; Schreve, K. The association between postural alignment and psychosocial factors to upper quadrant pain in high school students: A prospective study. Man. Ther. 2009, 14, 647–653. [Google Scholar] [CrossRef]
- Claus, A.; Hides, J.; Moseley, G.; Hodges, P. Is “ideal” sitting real?: Measurement of spinal curves in four sitting postures. Man. Ther. 2009, 14, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Scannell, J.P.; McGill, S.M. Lumbar posture—Should it, and can it, be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Phys. Ther. 2003, 83, 907–917. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D. The International Association for the Study of Pain definition of pain: As valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018, 3, e643. [Google Scholar] [CrossRef] [PubMed]
- Jones, D. Test and retest reliability of pressure pain threshold measurements of the upper limb and torso in young healthy women. J. Pain 2007, 8, 650e6. [Google Scholar] [CrossRef]
- Waller, R.; Smith, A.; O’Sullivan, P.; Slater, H.; Sterling, M.; McVeigh, J.; Straker, L. Pressure and cold pain threshold reference values in a large, young adult, pain-free population. Scand. J. Pain 2016, 13, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Sipko, T.; Kuczyński, M. Intensity of chronic pain modifies postural control in low back patients. Eur. J. Pain 2013, 17, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Neziri, A.; Scaramozzino, P.; Andersen, O.; Dickenson, A.; Arendt-Nielsen, L.; Curatolo, M. Reference values of mechanical and thermal pain tests in a pain-free population. Eur. J. Pain 2011, 15, 376–383. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P.; Waller, R.; Wright, A.; Gardner, J.; Johnston, R.; Payne, C.; Shannon, A.; Ware, B.; Smith, A. Sensory characteristics of chronic non-specific low back pain: A subgroup investigation. Man Ther. 2014, 19, 311–318. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.; Brinch Larsen, J.; Nim, C.; Arendt-Nielsen, L. Topographic mapping of pain sensitivity of the lower back—A comparison of healthy controls and patients with chronic non-specific low back pain. Scand. J. Pain. 2019, 19, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Balaguier, R.; Madeleine, P.; Vuillerme, N. Is One Trial Sufficient to Obtain Excellent Pressure Pain Threshold Reliability in the Low Back of Asymptomatic Individuals? A Test-Retest Study. PLoS ONE 2016, 11, e0160866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiarotto, A.; Boers, M.; Deyo, R.A.; Buchbinder, R.; Corbin, T.P.; Costa, L.O.P.; Foster, N.E.; Grotle, M.; Koes, B.W.; Kovacs, F.M.; et al. Core outcome measurement instruments for clinical trials in nonspecific low back pain. Pain 2018, 159, 481–495. [Google Scholar] [CrossRef]
- Lee, P.; Macfarlane, D.; Lam, T.; Stewart, S. Validity of the international physical activity questionnaire short form [IPAQ-SF]: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Biernat, E.; Stupnicki, R.; Gajewski, A. Międzynarodowy Kwestionariusz Aktywności Fizycznej [IPQA]-wersja polska. Wychowanie Fizyczne i Sport 2007, 51, 47–54. [Google Scholar]
- Barczyk-Pawelec, K.; Sipko, T. Active self-correction of spinal posture in pain-free women in response to the command “Straighten Your Back”. Women Health 2017, 57, 1098–1114. [Google Scholar] [CrossRef] [PubMed]
- American Society for Photogrammetry and Remote Sensing (ASPRS). What Is ASPRS? American Society for Photogrammetry and Remote Sensing: Bethesda, MD, USA, 2007; Available online: https://www.asprs.org/a/society/about.html (accessed on 4 January 2022).
- Saad, K.R.; Colombo, A.S.; Ribeiro, A.P.; Joao, S.M.A. Reliability of photogrammetry in the evaluation of the postural aspects of individuals with structural scoliosis. J. Bodyw. Mov. Ther. 2012, 16, 210–216. [Google Scholar] [CrossRef]
- Chesterton, L.; Barlas, P.; Foster, N.; Baxter, G.; Wright, C. Gender differences in pressure pain threshold in healthy humans. Pain 2003, 101, 259–266. [Google Scholar] [CrossRef]
- Özdolap, S.; Sarikaya, S.; Köktürk, F. Evaluation of Pain Pressure Threshold and Widespread Pain in Chronic Low Back Pain. Turk. Soc. Phys. Med. Rehabil. 2014, 60, 32–36. [Google Scholar] [CrossRef]
- Vialle, R.; Levassor, N.; Rillardon, L.; Templier, A.; Skalli, W.; Guigui, P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J. Bone Jt. Surg. 2005, 87, 260–267. [Google Scholar] [CrossRef]
- Endo, K.; Suzuki, H.; Nishimura, H.; Tanaka, H.; Shishido, T.; Yamamoto, K. Sagittal lumbar and pelvic alignment in the standing and sitting positions. J. Orthop. Sci. 2012, 17, 682–686. [Google Scholar] [CrossRef]
- Laird, R.; Gilbert, J.; Kent, P.; Keating, J. Comparing lumbo-pelvic kinematics in people with and without back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2014, 15, 229. [Google Scholar] [CrossRef] [PubMed]
- Kamel, E.; Abdelmajeed, S.; El Khozamy, H.; Hassan, K. Trunk and hip muscles activation patterns in subjects with and without chronic low back pain: A systematic review. Physiother. Q. 2021, 29, 79–88. [Google Scholar] [CrossRef]
- Chun, S.W.; Lim, C.Y.; Kim, K.; Hwang, J.; Chung, S. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J. 2017, 17, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, P.B.; Dankaerts, W.; Burnett, A.F.; Farrell, G.T.; Jefford, E.; Naylor, C.S.; O’Sullivan, K.J. Effect of different upright sitting postures on spinal-pelvic curvature and trunk muscle activation in a pain-free population. Spine 2006, 31, E707–E712. [Google Scholar] [CrossRef]
- Wong, A.; Chan, T.; Chau, A.; Tung Cheung, H.; Kwan, K.; Lam, A.; Wong, P.; De Carvalho, D. Do different sitting postures affect spinal biomechanics of asymptomatic individuals? Gait Posture 2019, 67, 230–235. [Google Scholar] [CrossRef]
- Korakakis, V.; O’Sullivan, K.; O’Sullivan, P.; Evagelinou, V.; Sotiralis, Y.; Sideris, A.; Sakellariou, K.; Karanasios, S.; Giakas, G. Physiotherapist perceptions of optimal sitting and standing posture. Musculoskelet. Sci. Pract. 2019, 39, 24–31. [Google Scholar] [CrossRef]
- Gouteron, A.; Tabard-Fougère, A.; Bourredjem, A.; Casillas, J.-M.; Armand, S.; Genevay, S. The flexion relaxation phenomenon in nonspecific chronic low back pain: Prevalence, reproducibility and flexion-extension ratios. A systematic review and meta-analysis. Eur. Spine J. 2021, 31, 136–151. [Google Scholar] [CrossRef]
- Rosenberg, S.; Sipko, T. Wpływ sposobu utrzymywania pozycji siedzącej na próg bólu tkanek miękkich w okolicy piersiowej i lędźwiowej kręgosłupa u osób bez objawów bólowych. Ból 2016, 17, 17–24. [Google Scholar] [CrossRef]
- Gupta, A.; McBeth, J.; Macfarlane, G.J.; Morriss, R.; Dickens, C.; Ray, D.; Chiu, Y.H.; Silman, A.J. Pressure pain thresholds and tender point counts as predictors of new chronic widespread pain in somatising subjects. Ann. Rheum. Dis. 2007, 66, 517–521. [Google Scholar] [CrossRef]
- Swain, C.T.V.; Pan, F.; Owen, P.J.; Schmidt, H.; Belavy, D.L. No consensus on causality of spine postures or physical exposure and low back pain: A systematic review of systematic reviews. J. Biomech. 2020, 102, 109312. [Google Scholar] [CrossRef] [PubMed]
- Griffith, L.E.; Shannon, H.S.; Wells, R.P.; Walter, S.D.; Cole, D.C.; Cote, P.; Frank, J.; Hogg-Johnson, S.; Langlois, L.E. Individual participant data meta-analysis of mechanical workplace risk factors and low back pain. Am. J. Public Health 2012, 102, 309–318. [Google Scholar] [CrossRef]
- Sipko, T.; Glibowski, E.; Kuczyński, M. Acute effects of proprioceptive neuromuscular facilitation exercises on the postural strategy in patients with chronic low back pain. Complement. Ther. Clin. Pract. 2021, 44, 101439. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LBP (n = 57) | CONTROL (n = 82) | p-Value LBP/CON Females | p-Value LBP/CON Males | |||
|---|---|---|---|---|---|---|
| F (n = 19) Mean (SD) | M (n = 38) Mean (SD) | F (n = 32) Mean (SD) | M (n = 50) Mean (SD) | |||
| Age (years) | 29.00 (3.68) | 29.39 (3.16) | 29.59 (3.42) | 29.72 (3.00) | 0.56 | 0.63 |
| Mass (kg) | 64.42 (9.27) | 86.95 (13.67) | 59.31(7.75) | 83.20 (11.95) | 0.03 * | 0.17 |
| Height (m) | 1.67 (0.07) | 1.80 (0.06) | 1.66 (0.05) | 1.80 (0.06) | 0.64 | 0.87 |
| BMI | 23.11 (3.75) | 26.67 (4.0) | 21.39 (2.72) | 25.56 (3.27) | 0.06 | 0.15 |
| TY (years) | 5.47 (3.39) | 6.21 (2.87) | 6.03 (3.30) | 6.02 (3.08) | 0.56 | 0.77 |
| TD (hours) | 10.11(1.70) | 9.84 (1.94) | 9.44 (1.92) | 9.70 (1.96) | 0.21 | 0.73 |
| Insuff PA (n) | 3 | 6 | 5 | 8 | Chi2 = 0.06, p = 0.80 | |
| Suff PA (n) | 11 | 19 | 18 | 29 | Chi2 = 0.02, p = 0.88 | |
| High PA (n) | 5 | 13 | 9 | 13 | Chi2 = 0.75, p = 0.39 | |
| NRS | 1.95 (0.78) | 2.23 (0.79) | - | - | 0.19 | |
| ODI | 9.10 (5.95) | 7.07 (4.83) | - | - | 0.17 | |
| PPT cervical | 17.21 (5.25) | 25.4 (11.22) | 16.20 (6.10) | 24.92 (9.07) | 1.0 | 1.0 |
| PPT thoracic | 29.99 (7.66) | 49.16 (24.81) | 27.35 (9.92) | 47.90 (18.56) | 0.99 | 1.0 |
| PPT lumbar | 32.93 (7.14) | 64.09 (28.32) | 33.10 (11.79) | 64.15 (23.19) | 1.0 | 1.0 |
| Model Steps | Variables | Females (n = 51) | Males (n = 88) | ||
|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | ||
| Base model a | |||||
| BMI | 1.89 (0.3–13.64) | 0.51 | 1.8 (0.9–3.64) | 0.08 * | |
| PA | 1.56 (0.32–7.68) | 0.56 | 1.46 (0.67–3.16) | 0.32 | |
| TY | 0.90 (0.71–1.16) | 0.42 | 1.05 (0.88–1.24) | 0.56 | |
| TD | 0.96 (0.59–1.57) | 0.88 | 1.12 (0.86–1.46) | 0.36 | |
| Pressure pain threshold | |||||
| Cervical | 1.02 (0.88–1.16) | 0.80 | 0.99 (0.97–1.02) | 0.93 | |
| Thoracic | 1.1 (0.99–1.22) | 0.06 * | 1.00 (0.98–1.01) | 0.90 | |
| Lumbar | 0.90 (0.81–0.98) | 0.03 * | 1.10 (0.97–1.11) | 0.91 | |
| Habitual position | |||||
| ALFAhab | 0.99 (0.83–1.18) | 0.96 | 0.97 (0.88–1.07) | 0.65 | |
| BETAhab | 1.30 (0.91–1.85) | 0.13 * | 0.97 (0.83–1.13) | 0.72 | |
| GAMMAhab | 1.02 (0.68–1.54) | 0.89 | 0.96 (0.80–1.16) | 0.72 | |
| KPThab | 1.14 (5.3–2.40) | 7.25 | |||
| Corrected position | |||||
| ALFAcorr | 0.96 (0.82–1.13) | 0.66 | 1.06 (0.97–1.17) | 0.15 * | |
| BETAcorr | 0.86 (0.56–1.33) | 0.49 | 0.99 (0.83–1.17) | 0.93 | |
| GAMMAcorr | 1.03 (0.69–1.54) | 0.85 | 1.16 (0.95–1.42) | 0.13 * | |
| KPTcorr | 9.12 (4.41–1.88) | 7.97 | 1.36 (0.97–1.88) | 0.06 * | |
| Final modelb | |||||
| PPTTh | 1.10 (1.02–1.19) | 0.009 ** | - | - | |
| PPTL | 0.90 (0.83–0.98) | 0.01 ** | - | - | |
| BETAhab | 1.19 (1.05–1.34) | 0.002 ** | - | - | |
| BMI | - | - | 1.56 (0.84–2.90) | 0.14 | |
| KPTcorr | - | - | 1.14 (1.01–1.29) | 0.02 * | |
| ALFAcorr | - | - | 1.06 (0.98–1.15) | 0.10 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żywień, U.; Barczyk-Pawelec, K.; Sipko, T. Associated Risk Factors with Low Back Pain in White-Collar Workers—A Cross-Sectional Study. J. Clin. Med. 2022, 11, 1275. https://doi.org/10.3390/jcm11051275
Żywień U, Barczyk-Pawelec K, Sipko T. Associated Risk Factors with Low Back Pain in White-Collar Workers—A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(5):1275. https://doi.org/10.3390/jcm11051275
Chicago/Turabian StyleŻywień, Urszula, Katarzyna Barczyk-Pawelec, and Tomasz Sipko. 2022. "Associated Risk Factors with Low Back Pain in White-Collar Workers—A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 5: 1275. https://doi.org/10.3390/jcm11051275