
Carisoprodol Single and Multiple Dose PK-PD. Part II: Pharmacodynamics Evaluation Method for Central Muscle Relaxants. Double-Blind Placebo-Controlled Clinical Trial in Healthy Volunteers


Abstract
:1. Introduction
2. Materials and Methods
2.1. PD Endpoints (Activity)
2.1.1. Muscle Relaxation
Electromyogram
Dynamometry
2.1.2. Central Activity: Sleepiness Tests
2.2. Tolerability: Psychomotor Impairment, Withdrawal Symptoms, and Adverse Events
2.2.1. Psychomotor Impairment
2.2.2. Adverse Events (AE)
2.2.3. Withdrawal Symptoms
2.3. Statistical Analysis
3. Results
3.1. Muscle relaxation
3.1.1. Electromyogram (EMG)
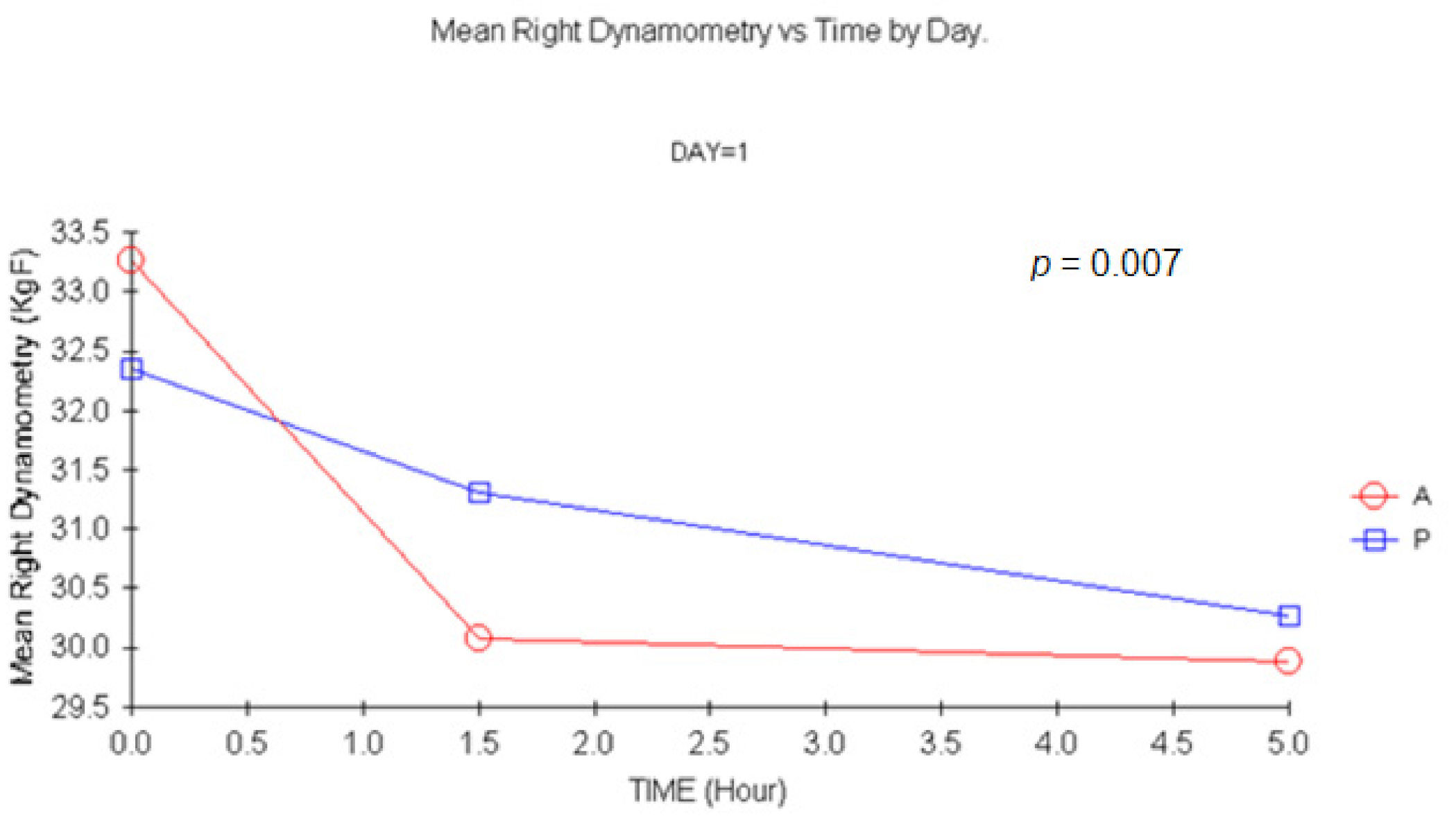
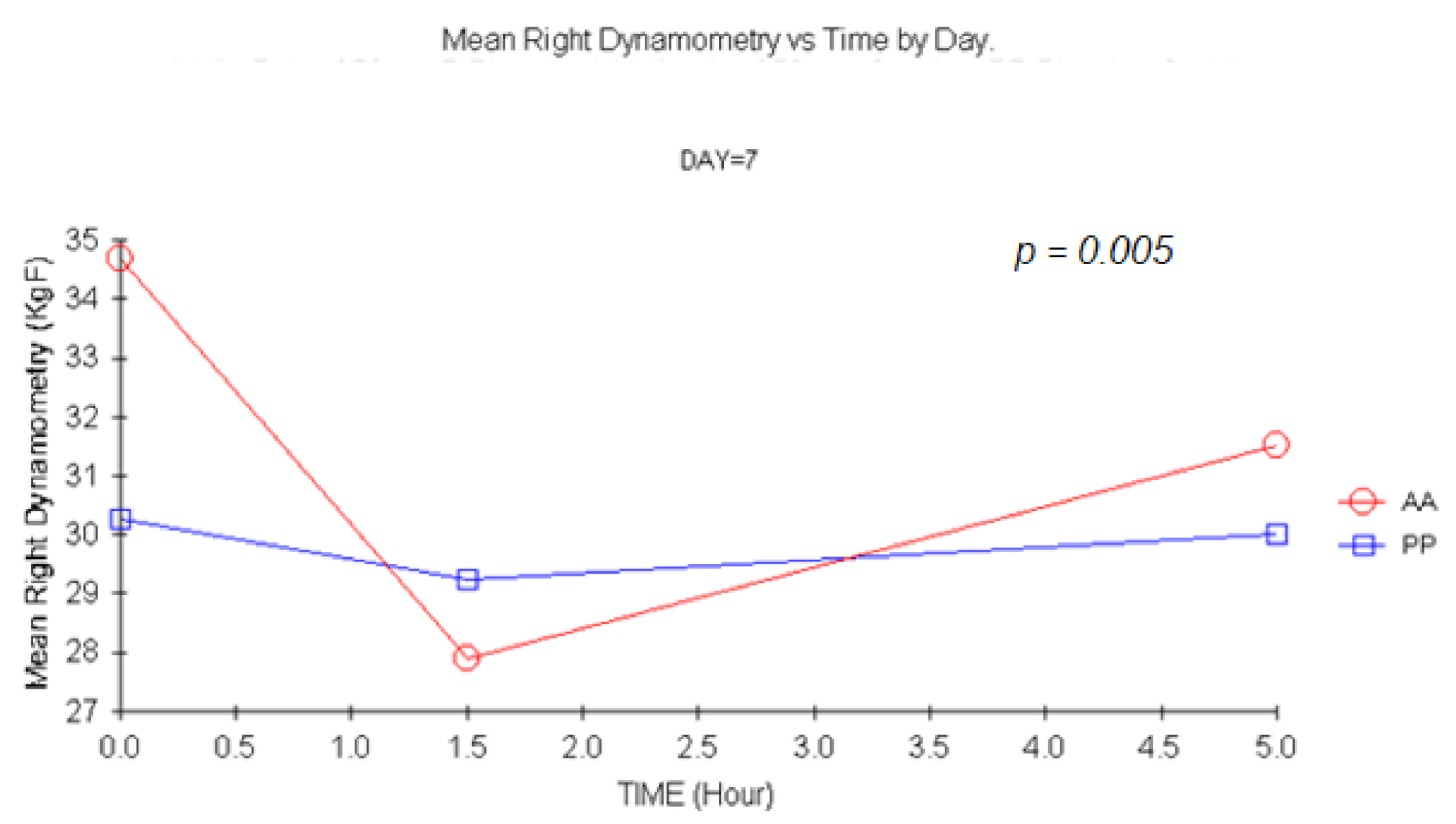
3.1.2. Dynamometry
3.2. Central Activity: Sleepiness Tests
3.2.1. Subject’s and Investigator’s Perceived Somnolence VAS
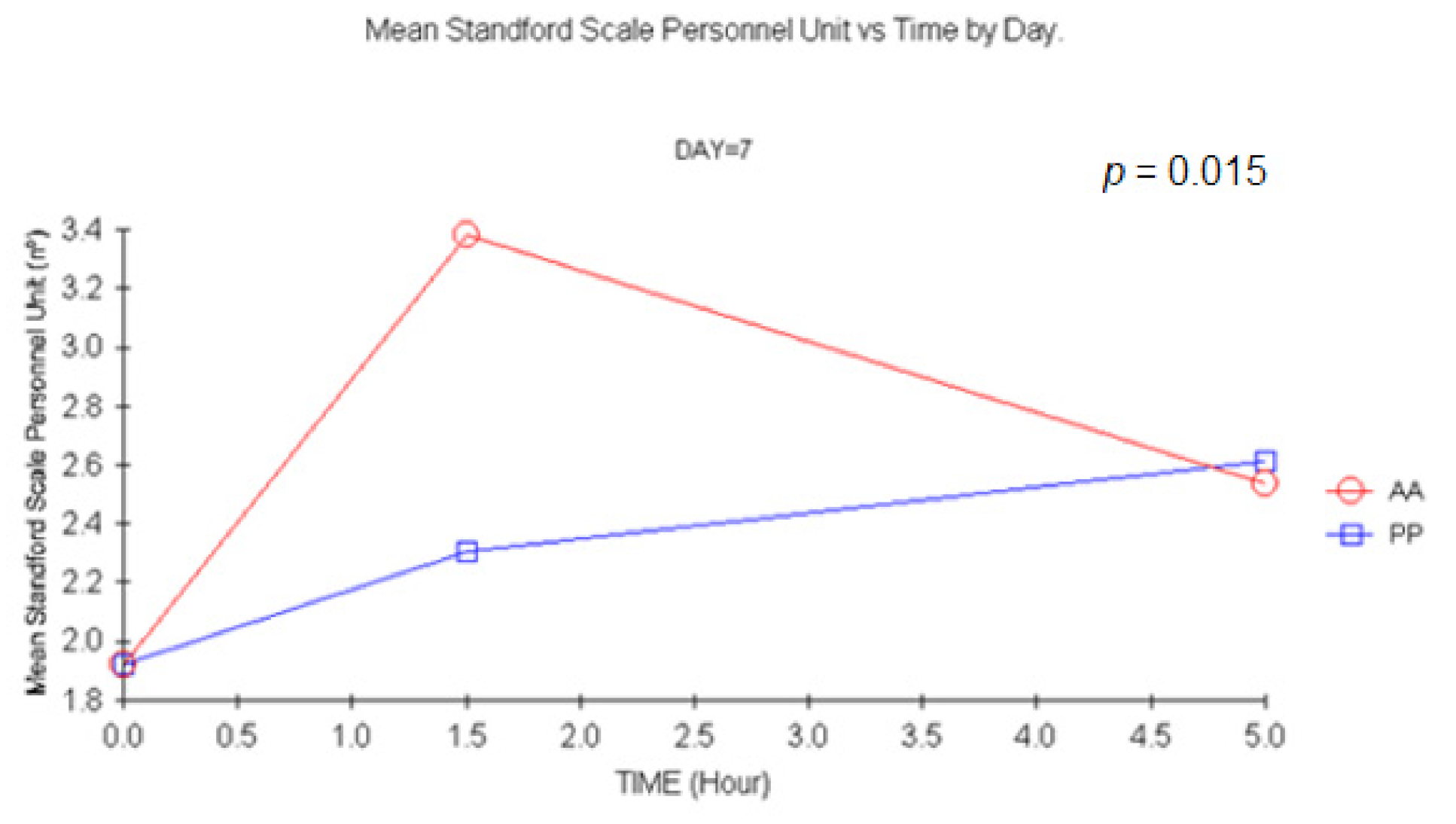
3.2.2. Subject’s and Investigator’s Stanford Sleepiness Scale (SSS)
4. Tolerability
4.1. Psychomotor Impairment
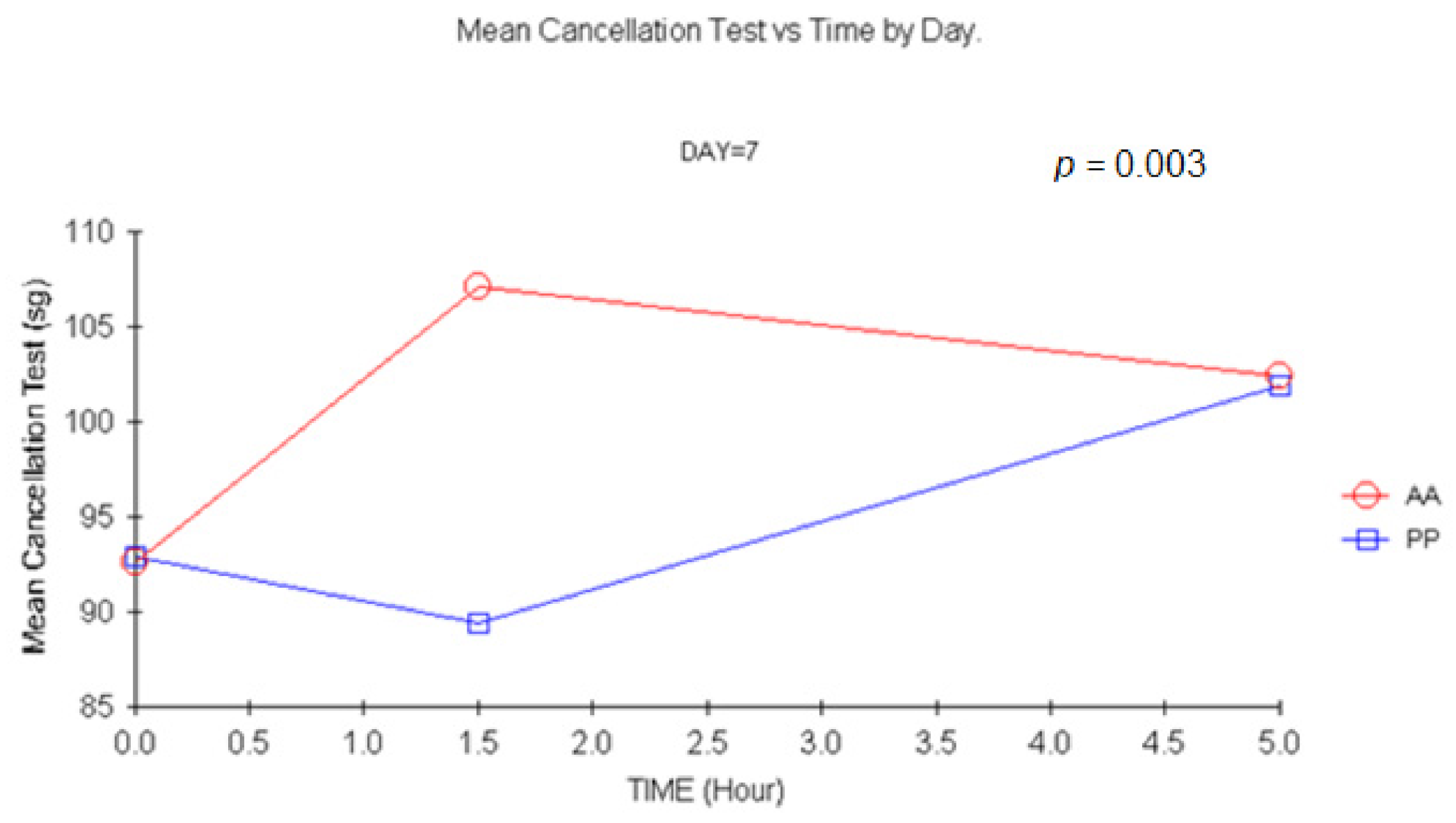
4.1.1. Cancellation Test (CT)
4.1.2. Digit Symbols Substitution Test (DSST or Numbers Key Test)
4.1.3. SVRT
4.2. Adverse Events
4.3. Abstinence Criteria—Withdrawal Symptoms
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Treatment Period | Fatigue (Dif %) Day 1 Difference Time 1.5 vs. 0 | Fatigue (Dif %) Day 1 Difference Time 5 vs. 0 | Fatigue (Dif %) Day 14 Difference Time 1.5 vs. 0 | Fatigue (Dif %) Day 14 Difference Time 5 vs. 0 | Fatigue (Dif %) Day 7 Difference Time 1.5 vs. 0 | Fatigue (Dif %) Day 7 Difference Time 5 vs. 0 | |
|---|---|---|---|---|---|---|---|
| P | N | 13 | 13 | 6 | 6 | 7 | 7 |
| Mean | −7.6956 | −10.5613 | 0.8594 | 0.3353 | −1.3249 | 2.1674 | |
| SD | 15.48327 | 14.85825 | 3.27662 | 3.85995 | 9.21977 | 6.46668 | |
| Median | −5.0132 | −4.9771 | 1.9944 | 0.8764 | −0.2614 | 1.4006 | |
| A | N | 13 | 13 | 6 | 6 | 6 | 6 |
| Mean | −5.1272 | −7.0049 | 1.1844 | −1.3189 | 3.7781 | −4.3638 | |
| SD | 14.53944 | 14.73740 | 4.36398 | 5.00332 | 7.80195 | 3.10312 | |
| Median | −6.5292 | −4.0153 | 1.7131 | −1.1970 | .3377 | −4.9519 |
| Drug Treatment Period | Dynamometry Left Day 1 Difference 1.5 vs. 0 | Dynamometry Left Day 1 Difference 5 vs. 0 | Dynamometry Left Day 14 Difference 1.5 vs. 0 | Dynamometry Left Day 14 Difference 5 vs. 0 | Dynamometry Left Day 7 Difference 1.5 vs. 0 | Dynamometry Left Day 7 Difference 5 vs. 0 | |
|---|---|---|---|---|---|---|---|
| P | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −1.8846 | −2.2308 | −0.5833 | 1.3750 | −2.8077 | −1.8077 | |
| SD | 4.37871 | 3.94554 | 2.89069 | 4.64232 | 5.13784 | 4.61221 | |
| Median | −1.0000 | −2.0000 | 0.0000 | 0.7500 | −2.0000 | − 2.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −2.7308 | −1.6538 | −1.6667 | −0.9583 | −6.8077 | −1.8077 | |
| SD | 5.95334 | 5.89980 | 5.34846 | 2.62383 | 5.47547 | 4.61221 | |
| Median | −2.5000 | −2.0000 | −0.7500 | −0.2500 | −7.5000 | −2.0000 | |
| Drug Treatment Period | Dynamometry Right Day 1 Difference 1.5 vs. 0 | Dynamometry Right Day 1 Difference 5 vs. 0 | Dynamometry Right Day 14 Difference 1.5 vs. 0 | Dynamometry Right Day 14 Difference 5 vs. 0 | Dynamometry Right Day 7 Difference 1.5 vs. 0 | Dynamometry Right Day 7 Difference 5 vs. 0 | |
| P | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −1.0385 | −2.0769 | −0.1538 | 1.3462 | − 3.2308 | −1.3077 | |
| SD | 4.1052 | 5.5896 | 3.8643 | 4.7626 | 6.0883 | 3.4250 | |
| Median | 0.0000 | −1.0000 | −1.0000 | 1.0000 | −2.0000 | − 2.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −3.1923 | −3.3846 | −3.2917 | −0.0417 | −4.6154 | −2.1538 | |
| SD | 5.78986 | 5.45112 | 8.5718 | 3.81062 | 4.49608 | 4.41298 | |
| Median | −4.5000 | −3.0000 | −1.0000 | −0.5000 | −2.0000 | −0.5000 |
| Drug Treatment Period | VAS (cm) Day 1 Difference 1.5 vs. 0 | VAS (cm) Day 1 Difference 5 vs. 0 | VAS (cm) Day 14 Difference 1.5 vs. 0 | VAS (cm) Day 14 Difference 5 vs. 0 | VAS (cm) Day 7 Difference 1.5 vs. 0 | VAS (cm) Day 7 Difference 5 vs. 0 | |
|---|---|---|---|---|---|---|---|
| Subject’s perceived somnolence | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −0.2692 | −0.4308 | −0.6538 | −0.8077 | 0.9769 | 0.6923 | |
| SD | 1.21955 | 2.46218 | 1.00715 | 1.75141 | 1.97448 | 2.69736 | |
| Median | 0.0000 | 0.0000 | −0.8000 | −1.1000 | 0.2000 | 0.3000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | 0.9615 | 0.2846 | 0.3833 | −0.6000 | 3.7308 | 0.7385 | |
| SD | 1.59767 | 1.60200 | 1.54027 | 1.29123 | 2.57403 | 2.16662 | |
| Median | 0.1000 | 0.0000 | 0.6500 | −0.2500 | 4.3000 | 0.4000 | |
| Investigator’s perceived somnolence | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −0.4769 | 0.0385 | −0.7154 | −0.6231 | 0.6077 | 0.8692 | |
| SD | 1.17200 | 1.43848 | 1.65068 | 1.80192 | 0.81595 | 1.08119 | |
| Median | −0.6000 | 0.3000 | −0.4000 | −0.4000 | 0.7000 | 0.9000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −0.1000 | 0.1615 | 0.2500 | −0.8417 | 2.5462 | 0.8538 | |
| SD | 1.53025 | 1.96661 | 0.95964 | 0.98761 | 1.84915 | 1.85590 | |
| Median | −0.3000 | −0.2000 | 0.0500 | −1.0500 | 2.1000 | 0.4000 | |
| Drug Treatment Period | Stanford Scale Day 1 Difference Time 1.5 vs. 0 | Stanford Scale Day 1 Difference Time 5 vs. 0 | Stanford Scale Day 14 Difference Time 1.5 vs. 0 | Stanford Scale Day 14 Difference Time 5 vs. 0 | Stanford Scale Day 7 Difference Time 1.5 vs. 0 | Stanford Scale Day 7 Difference Time 5 vs. 0 | |
|---|---|---|---|---|---|---|---|
| Subject’s Stanford Sleepiness Scale | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −0.3846 | −0.2308 | −0.5385 | −0.4615 | 0.6923 | 0.6923 | |
| SD | 0.76795 | 1.23517 | 0.87706 | 1.45002 | 1.10940 | 1.65250 | |
| Median | 0.0000 | 0.0000 | −1.0000 | −1.0000 | 0.0000 | 1.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | 0.3846 | 0.0000 | 0.4167 | −0.2500 | 2.4615 | 0.3077 | |
| SD | 0.96077 | 0.70711 | 0.90034 | 0.75378 | 1.61325 | 1.31559 | |
| Median | 0.0000 | 0.0000 | 1.0000 | 0.0000 | 3.0000 | 0.0000 | |
| Investigator’s Stanford Sleepiness Scale | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −0.4615 | −0.2308 | −0.5385 | −0.4615 | 0.3846 | 0.6923 | |
| SD | 0.87706 | 0.83205 | 0.87706 | 1.45002 | 0.86972 | 1.10940 | |
| Median | −1.0000 | 0.0000 | −1.0000 | −1.0000 | 0.0000 | 1.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −0.1538 | 0.0000 | 0.4167 | −0.2500 | 1.4615 | 0.6154 | |
| SD | 0.98710 | 1.22474 | 0.90034 | 0.75378 | 1.05003 | 1.55662 | |
| Median | 0.0000 | 0.0000 | 1.0000 | 0.0000 | 1.0000 | 0.0000 | |
| Drug Treatment Period | Day 1 Difference 1.5 vs. 0 | Day 1 Difference 5 vs. 0 | Day 14 Difference 1.5 vs. 0 | Day 14 Difference 5 vs. 0 | Day 7 Difference 1.5 vs. 0 | Day 7 Difference 5 vs. 0 | |
|---|---|---|---|---|---|---|---|
| Cancellation Test | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −5.3077 | −14.7692 | −8.6923 | −15.5385 | −3.4615 | 9.0769 | |
| SD | 7.37546 | 8.44742 | 8.99430 | 11.55145 | 5.48658 | 11.47070 | |
| Median | −5.0000 | −15.0000 | −7.0000 | −16.0000 | −4.0000 | 7.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −1.8462 | −10.6923 | −2.5000 | −12.2500 | 14.4615 | 9.7692 | |
| SD | 9.08154 | 7.26160 | 5.16104 | 10.04648 | 16.57114 | 17.27789 | |
| Median | −3.0000 | −12.0000 | −3.0000 | −12.0000 | 14.0000 | 7.0000 | |
| Digit Symbol Substitution Test (Numbers Key) | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | 2.6923 | 1.9167 | .3077 | 7.6667 | −3.4615 | 1.6923 | |
| SD | 5.29756 | 5.66422 | 4.17102 | 6.59660 | 5.54700 | 4.66163 | |
| Median | 4.0000 | 2.5000 | 1.0000 | 10.5000 | −2.0000 | 3.0000 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | −1.6154 | 3.6923 | −2.8333 | 6.6667 | −14.8462 | −3.6923 | |
| SD | 4.97558 | 3.17240 | 5.55687 | 6.51339 | 7.89352 | 12.65164 | |
| Median | −3.0000 | 2.0000 | −2.0000 | 7.0000 | −12.0000 | −1.0000 | |
| Simple visual reaction time (SVRT) | |||||||
| P | N | 13 | 13 | 13 | 13 | 13 | 13 |
| Mean | −0.012892 | −0.018185 | 0.007608 | 0.010754 | 0.0058 | −0.0034 | |
| SD | 0.0230643 | 0.0238022 | 0.0366391 | 0.0413096 | 0.05896 | 0.03816 | |
| Median | −0.007000 | −0.019100 | 0.005900 | 0.000000 | −0.0029 | 0.0008 | |
| A | N | 13 | 13 | 12 | 12 | 13 | 13 |
| Mean | 0.011115 | 0.008192 | 0.008883 | 0.016058 | 0.0921 | 0.0128 | |
| SD | 0.0543668 | 0.0379932 | 0.0294313 | 0.0837221 | 0.07610 | 0.04407 | |
| Median | −0.001000 | −0.009500 | −0.000900 | −0.006750 | 0.0530 | −0.0025 | |
References
- Waldman, H. Centrally acting skeletal muscle relaxants and associated drugs. J. Pain Symptom Manag. 1994, 9, 434–441. [Google Scholar] [CrossRef]
- Bramness, J.G.; Skurtveit, S.; Gulliksen, M.; Breilid, H.; Steen, V.M.; Morland, J. The CYP2C19 genotype and the use of oral contraceptives influence the pharmacokinetics of Carisoprodol in healthy human subjects. Eur. J. Clin. Pharmacol. 2005, 61, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Sweetman, S. Martindale: The Complete Drug Reference, 34th ed.; The Pharmaceutical Press: London, UK, 2005. [Google Scholar]
- Boothby, L.; Doering, P.; Hatton, R. Carisoprodol: A marginally effective skeletal muscle relaxant with serious abuse potential. Hosp. Pharm. 2003, 38, 337–345. [Google Scholar] [CrossRef]
- Littrell, R.; Hayes, L.; Stillner, V. Carisoprodol (Soma): A new and cautious perspective on an old agent. South. Med. J. 1993, 86, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Elenbaas, J.K. Centrally acting oral skeletal muscle relaxants. Am. J. Hosp. Pharm. 1980, 37, 1313–1323. [Google Scholar] [CrossRef]
- Bramness, J.G.; Skurtveit, S.; Morland, J. Impairment due to intake of Carisoprodol. Drug Alcohol Depend. 2004, 74, 311–318. [Google Scholar] [CrossRef]
- Sikdar, S.; Basu, D.; Malhotra, A.K.; Varma, V.K.; Mattoo, S.K. Carisoprodol abuse: A report from India. Acta Psychiatr. Scand. 1993, 88, 302–303. [Google Scholar] [CrossRef]
- Toth, P.P.; Urtis, J. Commonly used muscle relaxant therapies for acute low back pain: A review of Carisoprodol, cyclobenzaprine hydrochloride, and metaxalone. Clin. Ther. 2004, 26, 1355–1367. [Google Scholar] [CrossRef]
- Reeves, R.R.; Beddingfield, J.J.; Mack, J.E. Carisoprodol withdrawal syndrome. Pharmacotherapy 2004, 24, 1804–1806. [Google Scholar] [CrossRef]
- Calvo, A.; Alonso, S.; Prieto, E.; Ascaso-del-Rio, A.; Ortuño, J.; Fernandez, N.; Portolés, A. Single and Multiple Dose PK-PD Characterization for Carisoprodol. Part I: Pharmacokinetics, Metabolites and 2C19 Phenotype Influence. Double-Blind, Placebo-Controlled Clinical Trial in Healthy Volunteers. J. Clin. Med. 2022, 11, 858. [Google Scholar] [CrossRef]
- Nevins, M.E.; Nash, S.A.; Beardsley, P.M. Quantitative grip strength assessment as a means of evaluating muscle relaxation in mice. Psychopharmacology 1993, 110, 92–96. [Google Scholar] [CrossRef]
- Simiand, J.; Keane, P.E.; Biziere, K.; Soubrie, P. Comparative study in mice of tetrazepam and other centrally active skeletal muscle relaxants. Arch. Int. Pharmacodyn. Ther. 1989, 297, 272–285. [Google Scholar]
- Maurissen, J.P.; Marable, B.R.; Andrus, A.K.; Stebbins, K.E. Factors affecting grip strength testing. Neurotoxicol. Teratol. 2003, 25, 543–553. [Google Scholar] [CrossRef]
- Hillman, T.E.; Nunes, Q.M.; Hornby, S.T.; Stanga, Z.; Neal, K.R.; Rowlands, B.J. A practical posture for hand grip dynamometry in the clinical setting. Clin. Nutr. 2005, 24, 224–228. [Google Scholar] [CrossRef]
- Arnedt, J.T.; Owens, J.; Crouch, M.; Stahl, J.; Carskadon, M.A. Neurobehavioral performance of residents after heavy night call vs. after alcohol ingestion. JAMA 2005, 294, 1025–1033. [Google Scholar] [CrossRef]
- Lucchesi, L.M.; Braga, N.I.; Manzano, G.M.; Pompeia, S.; Tufik, S. Acute neurophysiological effects of the hypnotic zolpidem in healthy volunteers. Prog. Neuropsychopharmacol. Biol. Psychiatry 2005, 29, 557–564. [Google Scholar] [CrossRef]
- Richardson, G.S.; Roehrs, T.A.; Rosenthal, L.; Koshorek, G.; Roth, T. Tolerance to daytime sedative effects of H1 antihistamines. J. Clin. Psychopharmacol. 2002, 22, 511–515. [Google Scholar] [CrossRef]
- Micallef, J.; Soubrouillard, C.; Guet, F.; Le Guern, M.E.; Alquier, C.; Bruguerolle, B. A double blind parallel group placebo controlled comparison of sedative and mnesic effects of etifoxine and lorazepam in healthy subjects. Fundam. Clin. Pharmacol. 2001, 15, 209–216. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, W.M.; Hanks, G.W.; Simpson, P.; Fallon, M.T.; Jenkins, E.; Wesnes, K. The cognitive and psychomotor effects of morphine in healthy subjects: A randomized controlled trial of repeated (four) oral doses of dextropropoxyphene, morphine, lorazepam and placebo. Pain 2000, 85, 209–215. [Google Scholar] [CrossRef]
- Frattola, L.; Maggioni, M.; Cesana, B.; Priore, P. Double blind comparison of zolpidem 20 mg versus flunitrazepam 2 mg in insomniac in-patients. Fármacos. Exp. Clin. Res. 1990, 16, 371–376. [Google Scholar]
- Lucchesi, L.M.; Pompeia, S.; Manzano, G.M.; Kohn, A.F.; Galduroz, J.C.; Bueno, O.F.; Tufik, S. Flunitrazepam-induced changes in neurophysiological, behavioral, and subjective measures used to assess sedation. Prog. Neuropsychopharmacol. Biol. Psychiatry 2003, 27, 525–533. [Google Scholar] [CrossRef]
- Girre, C.; Bertaux, L.; Dussaucy, E.; Palombo, S.; Crouzette, J.; Fournier, P.E. Comparative effects on psychomotor performance of the muscle relaxant afloqualone, alone and with ethanol. Fundam. Clin. Pharmacol. 1991, 5, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Girre, C.; Hirschhorn, M.; Bertaux, L.; Palombo, S.; Dellatolas, F.; Ngo, R. Enhancement of propoxyphene bioavailability by ethanol. Relation to psychomotor and cognitive function in healthy volunteers. Eur. J. Clin. Pharmacol. 1991, 41, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Wetherell, A. Cognitive and psychomotor performance tests and experiment design in multiple chemical sensitivity. Environ. Health Perspect. 1997, 105, 495–503. [Google Scholar]
- Roache, J.D.; Griffiths, R.R. Lorazepam and meprobamate dose effects in humans: Behavioral effects and abuse liability. J. Pharmacol. Exp. Ther. 1987, 243, 978–988. [Google Scholar]
- Zammit, G.K.; McNabb, L.J.; Caron, J.; Amato, D.A.; Roth, T. Efficacy and safety of eszopiclone across 6-weeks of treatment for primary insomnia. Curr. Med. Res. Opin. 2004, 20, 1979–1991. [Google Scholar] [CrossRef]
- Erman, M.K.; Loewy, D.; Scharf, M.B. Comparison of temazepam 7.5 mg with temazepam 15 mg for the treatment of transient insomnia. Curr. Med. Res. Opin. 2004, 20, 441–449. [Google Scholar] [CrossRef]
- Zacny, J.P.; Gutierrez, S. Characterizing the subjective, psychomotor, and physiological effects of oral oxycodone in non-drug-abusing volunteers. Psychopharmacology 2003, 170, 242–254. [Google Scholar] [CrossRef]
- Waterloo, K. The effect of Carisoprodol on Carisoprodol on performance on repeatedly administered neuropsychological Tests. Hum. Psychopharmacol. 1997, 12, 393–396. [Google Scholar] [CrossRef]
- Raffel, S.C.; Swink, R.; Lampton, T.D. The influence of chlorphenesin carbamate and Carisoprodol on psychological test scores. Curr. Ther. Res. Clin. Exp. 1969, 11, 553–560. [Google Scholar]
- Weschler, D. Administration and Scoring Guide. In WAIS-III, Weschler Adult Intelligence Scale, 3rd ed.; Harcourt Brace and Company: San Antonio, TX, USA, 1997. [Google Scholar]
- Bramness, J.G.; Furu, K.; Engeland, A.; Skurtveit, S. Carisoprodol use and abuse in Norway: A pharmacoepidemiological study. Br. J. Clin. Pharmacol. 2007, 64, 210–218. [Google Scholar] [CrossRef] [Green Version]
- Owens, C.; Pugmire, B.; Salness, T.; Culbertson, V.; Force, R.; Cady, P.; Steiner, J. Abuse potential of Carisoprodol: A retrospective review of Idaho Medicaid pharmacy and medical claims data. Clin. Ther. 2007, 29, 2222–2225. [Google Scholar] [CrossRef]
- Gregory, T.S.; Wheeler, W.J.; Sacks, H.J. Randomized, double-blind trial of carisoprodol 250 mg compared with placebo and carisoprodol 350 mg for the treatment of low back spasm. Curr. Med. Res. Opin. 2010, 26, 91–99. [Google Scholar]
- Bailey, D.N.; Briggs, J.R. Carisoprodol: An unrecognized drug of abuse. Am. J. Clin. Pathol. 2002, 117, 396–400. [Google Scholar] [CrossRef]
- Logan, B.K.; Case, G.A.; Gordon, A.M. Carisoprodol, meprobamate, and driving impairment. J. Forensic Sci. 2000, 45, 619–623. [Google Scholar] [CrossRef]
- Boakes, J.; Peach, J.P.; McGill, S.M. Does methocarbamol affect fatiga markers in the low-back electromyogram? J. Electromyogr. Kinesiol. 1998, 8, 423–427. [Google Scholar] [CrossRef]
- Ortiz-Gómez, J.R. Efecto directo de los inductores anestésicos sobre el registro electromiográfico del adductor pollicis. Rev. Esp. Anestesiol. Reanim. 2000, 47, 157–161. (In Spanish) [Google Scholar]
- Souri, E.; Sharifzadeh, M.; Farsam, H.; Gharavi, N. Muscle relaxant activity of methocarbamol enantiomers in mice. J. Pharm. Pharmacol. 1999, 51, 853–855. [Google Scholar] [CrossRef]
- Yang, S.I.; Park, H.Y.; Lee, S.H.; Lee, S.J.; Han, O.Y.; Lim, S.C. Transdermal eperisone elicits more potent and longer-lasting muscle relaxation than oral eperisone. Pharmacology 2004, 71, 150–156. [Google Scholar] [CrossRef]
- Bach-Rojecky, L.; Samarzija, I. Influence of ethanol on the myorelaxant effect of diazepam in rats. Acta Pharm. 2005, 55, 115–122. [Google Scholar]
- Alkhazrajy, W.; Khorasanee, A.D.; Russell, W.J. Muscle weakness after muscle relaxants: An audit of clinical practice. Anaesth. Intensive Care 2004, 32, 256–259. [Google Scholar] [CrossRef] [Green Version]
- United States Environmental Protection Agency. Guidelines for Neurotoxicity Risk Assessment. Available online: https://www.epa.gov/sites/default/files/2014-11/documents/neuro_tox.pdf (accessed on 14 December 2021).
- Zadrozniak, A.; Wojda, E.; Wlaź, A.; Łuszczki, J.J. Characterization of acute adverse-effect profiles of selected antiepileptic drugs in the grip-strength test in mice. Pharmacol. Rep. 2009, 61, 737–742. [Google Scholar] [CrossRef]










| Period A (Carisoprodol/Placebo) | Period B (Placebo/Carisoprodol) | |||||||
|---|---|---|---|---|---|---|---|---|
| D1 | D7 | D14 | Day 14 Period A +48, 120 and 168 h | D1 | D7 | D14 | Day 14 Period B +168–24 h | |
| PK | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| EMG | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Sedation scales | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Psychomotor activity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Dynamometry | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Adverse events | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Withdrawal symptoms | ✓ | ✓ | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo, A.; González-Hidalgo, M.; Terleira, A.; Fernández, N.; Portolés, A. Carisoprodol Single and Multiple Dose PK-PD. Part II: Pharmacodynamics Evaluation Method for Central Muscle Relaxants. Double-Blind Placebo-Controlled Clinical Trial in Healthy Volunteers. J. Clin. Med. 2022, 11, 1141. https://doi.org/10.3390/jcm11041141
Calvo A, González-Hidalgo M, Terleira A, Fernández N, Portolés A. Carisoprodol Single and Multiple Dose PK-PD. Part II: Pharmacodynamics Evaluation Method for Central Muscle Relaxants. Double-Blind Placebo-Controlled Clinical Trial in Healthy Volunteers. Journal of Clinical Medicine. 2022; 11(4):1141. https://doi.org/10.3390/jcm11041141
Chicago/Turabian StyleCalvo, Aitana, Mercedes González-Hidalgo, Ana Terleira, Nieves Fernández, and Antonio Portolés. 2022. "Carisoprodol Single and Multiple Dose PK-PD. Part II: Pharmacodynamics Evaluation Method for Central Muscle Relaxants. Double-Blind Placebo-Controlled Clinical Trial in Healthy Volunteers" Journal of Clinical Medicine 11, no. 4: 1141. https://doi.org/10.3390/jcm11041141