1. Introduction
Migraine is a highly disabling headache disorder with an estimated global prevalence of around 15% of the world’s population [
1,
2,
3,
4]. Migraine is associated with a high individual burden and is considered a major socioeconomic problem with approximately
$36 billion in direct and indirect medical costs in the United States alone [
2,
5,
6].
For migraine with frequent attacks, severe accompanying symptoms, persistent aura, or insufficient effect of acute medication, migraine prophylaxis should be offered to the patient, according to the guidelines [
7,
8]. The pharmacological prophylaxis of migraine attacks is usually carried out with drugs originally intended for other indications, such as beta blockers, calcium channel blockers, anticonvulsants, or antidepressants, as these drugs have an “incidental” effect that reduces migraine frequency [
7,
9,
10]. However, most of these drugs may lead to numerous adverse events such as dizziness, diarrhea, fatigue, weight gain, or erectile dysfunction, which is believed to be the main reason that drug adherence is very low [
11,
12]. A relatively new—and first migraine specific—pharmacological strategy is the blockade of the neuropeptide calcitonin gene-related peptide (CGRP) or its receptor by antibodies [
13]. However, due to high costs, this approach is currently not routinely offered to all patients [
14,
15]. An accompanying non-pharmacological therapy and prophylaxis are frequently recommended and also mentioned in some clinical guidelines [
7]. For instance, these non-pharmacological approaches include, above all, stress-reducing measures such as muscle relaxation or biofeedback, acupuncture, neurostimulation, and nutritional supplements [
16]. However, non-pharmacological therapy is not yet part of standardized migraine therapy and is not accessible in all parts of the world. In addition, specific dietary interventions are not part of the current standard of care, although more than two-thirds of all migraine patients report their diet as a trigger on migraine activity, such as prolonged periods of fasting, alcohol, or distinct food [
17]. In particular, certain foods such as cheese, chocolate, or citrus fruits are frequently reported to induce migraine attacks [
18,
19]. However, there is currently no clear understanding of a possible relation and usually, provocation studies fail [
20]. Consequently, many authors recommend that clinicians should refrain from supporting an appreciation that avoidance of specific food items had a role in therapy as long as studies have not found sufficient supporting evidence [
10].
Potentially greater influence than food triggers may be body weight and obesity-related metabolism. In a recent meta-analysis including a total of 10 randomized studies, a positive effect of weight reduction could be demonstrated [
21]. However, the underlying mechanisms remain uncertain since the reduction in migraine activity was independent of the amount of body weight loss.
A potential pathological link between nutrition and migraine may be a disturbed glucose-insulin metabolism. Glucose has an essential role in the energy supply to the central nervous system and was hypothesized to be a potential pathophysiological correlate for migraine as early as 1935 [
22]. Recent data suggest that energy and particularly glucose-dependent mechanisms play a role in migraine pathology including cortical spreading depolarization and TRPA1-induced CGRP release [
23]. Supporting evidence for an important role of glucose-insulin metabolism comes from a recent dietary intervention trial demonstrating that a very low carbohydrate diet, which is known to reduce the overall glycemic load, significantly improved migraine symptoms in patients with drug-refractory chronic migraine [
24]. Moreover, Evcili et al. studied the effect of a low-glycemic index (GI) diet compared with migraine prophylaxis with either propranolol, flunarizine, or amitriptyline in a cohort of 348 migraineurs. Here, the effect of a low GI diet was non-inferior to pharmacological migraine prophylaxis [
25].
Personalized nutrition represents an evolution of low GI approaches. In 2015, a large prospective study with more than 800 participants demonstrated that postprandial glucose responses (PPGR) to identical test meals are highly variable across individuals and influenced by anthropometry and the individual composition of the intestinal microbiome [
26]. Berry et al. not only confirmed the strong interindividual effects of identical meals but additionally demonstrated that numerous other factors such as genetics, premeal physical activity, and sleep influence individual PPGR [
27]. Together, these studies led to a paradigm shift in nutritional medicine. Not the food itself is considered the main determinant of the biological effect of nutrition, but individual factors such as microbiome, genetics, or lifestyle.
In our study, we explored whether personalized nutrition targeting the PPGR may influence migraine disease severity. We surveyed 238 migraine patients, who took part in a digital nutrition program that generates personalized dietary recommendations based on the analysis of individual continuous glucose measurements. A total of 84 individuals completed the retrospective digital survey. Using retrospective analysis, we were able to obtain first data indicating that a digital health application allowing a personalized low-glycemic nutrition has a potential prophylactic effect on migraine.
4. Discussion
The objective of the present study was to produce the first proof-of-concept of whether a personalized low-glycemic nutritional intervention as a digital therapy can potentially exert clinically relevant effects in the prophylaxis of migraine attacks. Indeed, data from the present study indicate that an individually tailored low-glycemic dietary intervention may be effective in the prophylaxis of migraine.
A complete cohort of 84 patients who reported having a physician-confirmed migraine, was set up. The cohort was heterogeneous with respect to baseline migraine frequency (from a minimum of 1 migraine day per month to a maximum of 28 days per month) and related migraine symptoms. The cohort was mostly female, had concomitant tension-type headaches in 56%, frequently received antimigraine medical care in 57.1%, frequently used acute medication such as painkillers or triptans, and less frequently used prophylactic medications. A total of 29 patients (34.5%) reported having one migraine day per month at baseline classified as “rare” migraine in order to distinguish it from the remaining 55 patients with “regular” migraine. Of these, three subjects reported more than 14 migraine days per month at baseline and could be suspected to have chronic migraine. However, due to the lack of data collected in a headache diary and the retrospective nature, this issue was not further considered for the analyses performed. Taken together, the complete cohort can be considered representative for patients with migraine. However, future research should collect data with more detailed information about the clear characteristics of the reported headaches.
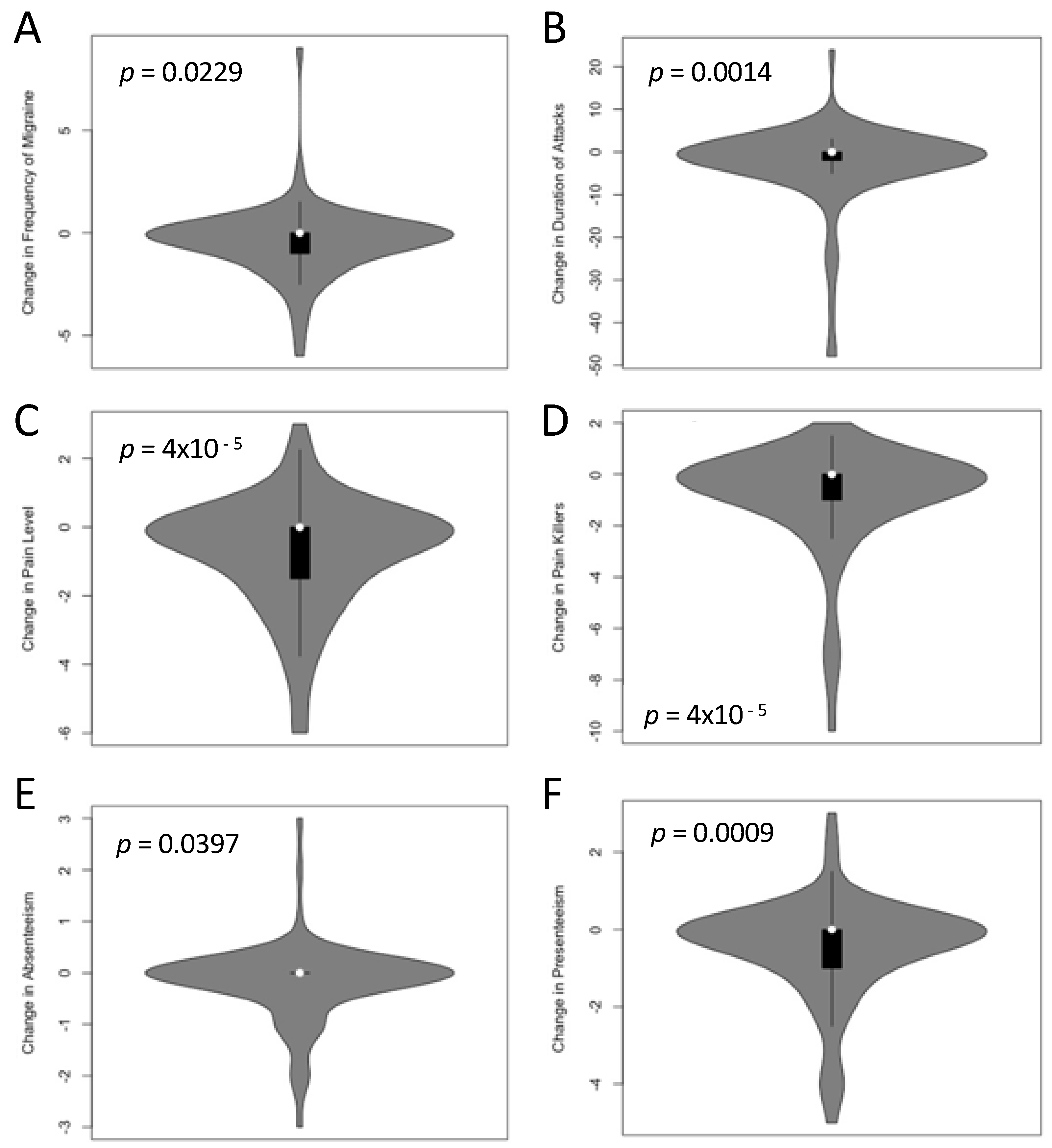
An analysis of reported clinically relevant symptoms before and after receiving the PLGN report, such as attack frequency, pain level, duration of attacks, the need for painkiller intake, and days with absenteeism or presenteeism, were significantly lower after taking part in this nutritional program as compared with the situation before. This highlights the potential therapeutic effect of this nutritional approach in migraine prophylaxis. However, these data need confirmation with a prospective data collection and additional measures addressing potential confounding factors.
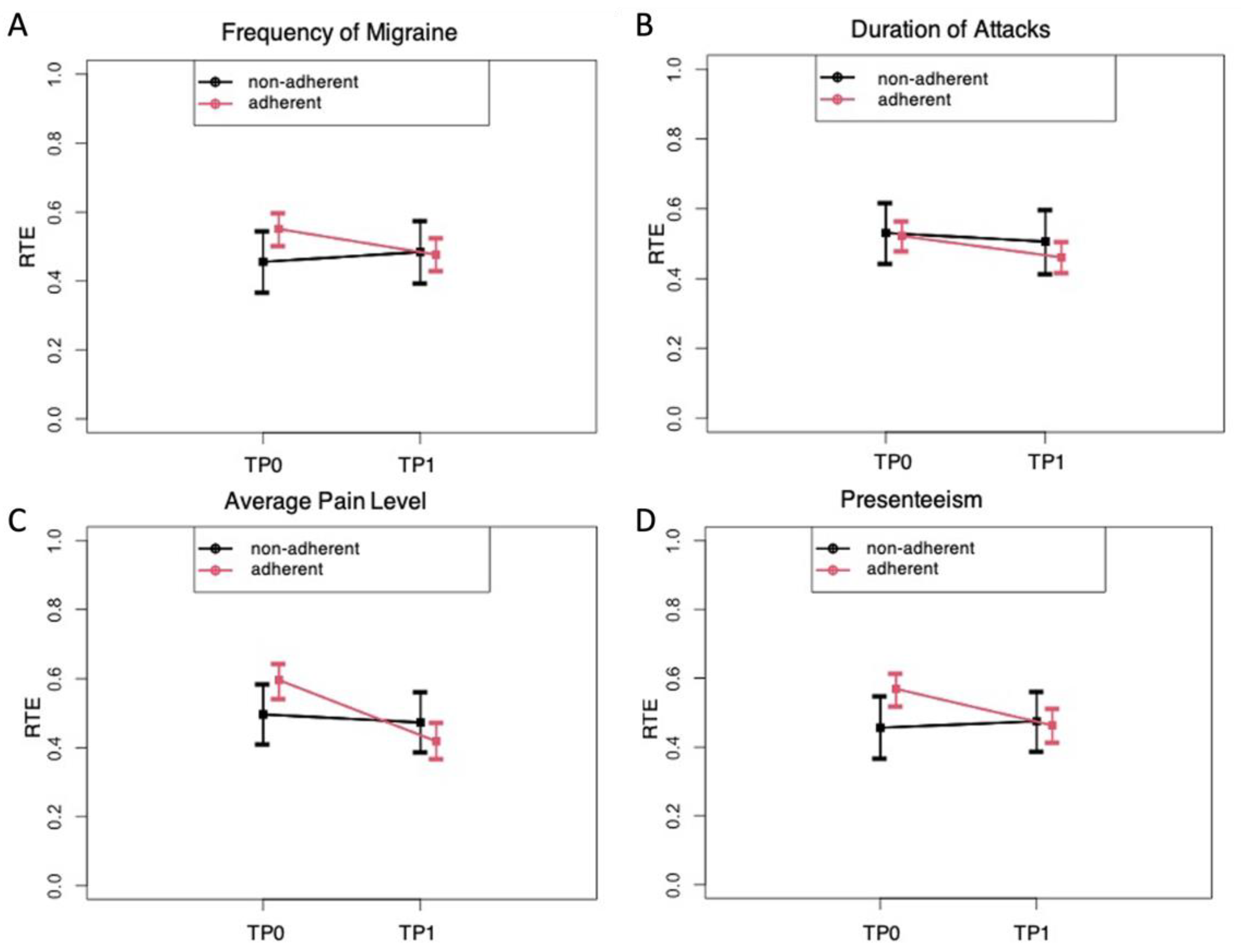
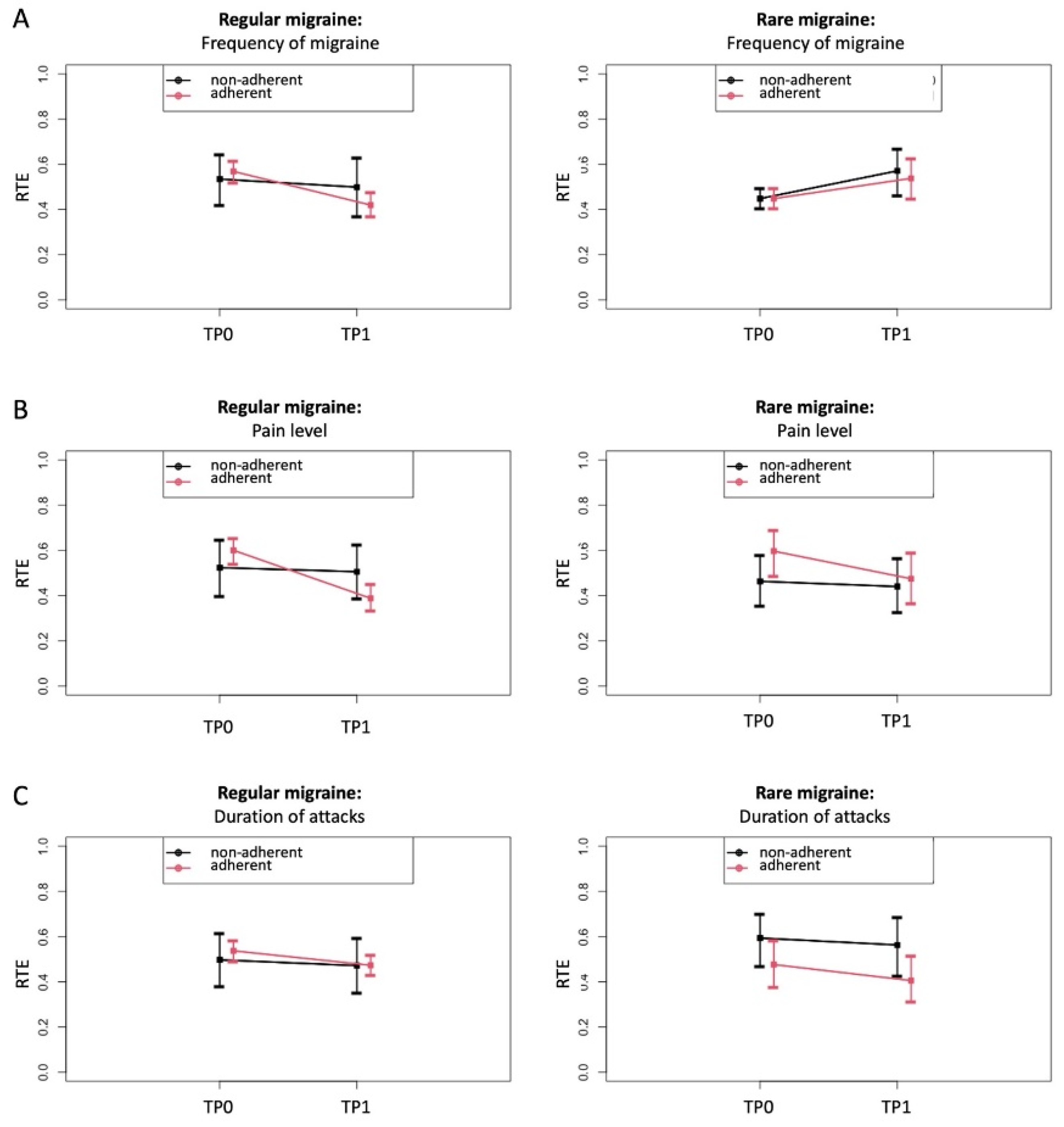
To further evaluate whether these changes may depend on the fact that 58 patients reported to daily follow the personalized nutrition recommendation (“adherent subgroup”) and 26 reported following the recommendation less than once a day (“non-adherent subgroup”), we separately analyzed the changes for adherent and non-adherent patients. In fact, the changes were clearly predominant in the adherent subgroup. Specifically, our non-parametric analysis of variance indicated that the intraindividual changes were more prominent in the adherent group. In further subgroup analyses of patients with regular migraine, those who were adherent to the personalized recommendations reported a mean reduction in migraine frequency of 33%. According to expert assessment, this alone can be classified as clinically relevant [
39]. In 38% of patients with regular migraines, the frequency of migraines even improved by at least 50% (i.e., response rate). Placebo-controlled studies on the effect of the new migraine-specific CGRP antibodies in migraine prophylaxis showed a 36% to 43% response rate [
40,
41,
42,
43]. This indicates the potential effectiveness of the PLGN report in the range of drug effects. In addition, this finding is in line with previous reports about the positive impact of diets that stabilize glycemic reactions on migraine symptoms [
24,
25,
29].
It has to be appreciated that both factors, adherence to the recommendations and change in migraine severity, were assessed in a retrospect manner; so it cannot be ruled out that both observations may interact. Accordingly, this analysis does not allow for confirmatory conclusions about the causative role of the nutrition intervention; however, it can be considered as the first proof-of-concept data that following personalized low-glycemic nutritional recommendation has the potential to reduce migraine severity.
At this point, it remains uncertain by which exact mechanisms a personalized low-glycemic diet may reduce migraine symptoms. One possible mechanism may be via an increased insulin secretion that occurs in association with high PPGR. After ingestion of rapidly absorbable carbohydrates, blood glucose levels frequently drop to levels below pre-prandial blood glucose levels. This phenomenon is usually explained by excessive insulin secretion in the sense of a complex physiological counterregulatory response [
44]. Part of this compensatory response could be an increased CGRP secretion. CGRP has an effect on glucose levels and is capable of inducing relative hyperglycemia [
45]. Vice versa, CGRP levels are elevated in patients during a migraine attack [
46], which is discussed in the literature as a consequence of a presumed migraine-specific central nervous energy deficit after an excess energy usage before the attack, among other factors [
23]. However, it remains speculative if the hyperinsulinemia characteristically observed in migraine patients represents a counterregulatory response to chronic CGRP elevation [
47,
48] or might be even the origin of this phenomenon. The consequence of following a low-glycemic food is a reduction in PPGR and an improvement of systemic insulin sensitivity.
It is debated whether and how diabetes mellitus and migraine may be interrelated [
49]. Epidemiological data suggest that diabetes is less frequent in migraine patients and vice versa [
50]. A diverging regulation of CGRP is one approach to an explanation [
50]; however, underlying mechanisms are still elusive.
In addition, a low-glycemic diet potentially has an impact on the central nervous system [
48]. As an alternate hypothesis, a low-glycemic approach may favor economization of the central nervous energy supply, thereby counteracting the central nervous energy deficit suspected in migraine [
23]. Furthermore, a reduction in oxidative stress levels could also be an explaining mechanism [
51,
52,
53].
A low-glycemic approach may be beneficial in various diseases [
54,
55]; however, inconsistent effects are reported in the prevention and management of chronic diseases [
56,
57,
58]. This may be due to the high interindividual variance of the PPGR [
26,
27]. In fact, it is increasingly appreciated that effective personalization strategies are needed to tailor dietary recommendations to the individual’s metabolism. The obvious advantage over generalized low-glycemic recommendations is that personalized nutrition approaches based on objectively measured data—such as CGM data—take into account individual metabolism and consequently are more precise than general dietary recommendations [
27].
5. Limitations
Of note, the data should be interpreted cautiously since several limitations arise from the retrospective study design.
First, the patients were asked to recall their migraine symptoms from the time before participating in the program. The mean time since the receipt of the personalized, low-glycemic nutrition report was 56.4 months with a minimum of 5.7 months and a maximum of 118 months. This leads to a potential recall bias. However, it is described that, when recording migraine days retrospectively, patients can tend to underestimate baseline numbers of headaches in periods that are longer ago [
59]. Therefore, it can also be speculated that the frequency of migraine headaches was underestimated at the baseline rather than at the time of the survey and that the effect described could actually be even higher. However, no statistical relationship was detected between the individual observation time (time between baseline TP0 and survey TP1) and the specified baseline disease severity or the individual change in migraine days.
Second, the patients reported a physician-confirmed diagnosis, but no written confirmation was obtained, which could lead to a misclassification bias. In addition, the missing headache diary does not allow checking for ICHD criteria.
Third, no control measure for other migraine interventions such as other prophylactic drugs or non-pharmacological interventions was taken. In addition, the study does not involve a control group with a different or no treatment. This leads to uncertainty that the change in migraine severity could be induced by other factors than the nutritional intervention.
Forth, not all approached patients took part in the survey, the response rate was 45.8%. No data about the baseline disease severity of the course of the disease could be analyzed from the non-responding patients leading to a potential selection bias. In addition, patients responding to the survey request may have their own ideas about the involvement of nutrition and may tend to not objectively report their symptoms after the intervention (reporting bias).
Fifth, it is unknown why the patients took part in the nutrition program in the first place as it was not specifically advertised as a nutritional program for migraine prophylaxis. The reason for participation could also interfere with the study results. On the one hand, not knowing about a potential effect could reduce a confounding “placebo effect”, and on the other hand, the motivation to adhere or not adhere to the dietary recommendation could be influenced by factors unconnected to the disease.
More open questions arise from this study; e.g., the question remains whether the avoidance of an individually hyperglycemic postprandial glucose response is causally related to the observed effects or whether other factors, such as the sole use of a nutrition app, also have an influence on the frequency and severity of migraine patients. The fact that those participants who did not follow the dietary recommendations did not report improvement in clinical migraine symptoms supports the view of a causal relation.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}