
Ablation of Left Atrial Tachycardia following Catheter Ablation of Atrial Fibrillation: 12-Month Success Rates

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Catheter Ablation Approaches
2.3. Further Ablation Strategies and Reinduction
2.4. Study Endpoints and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Investigated Mechanisms of the Tachycardia
3.3. Primary Endpoint
3.4. Secondary Endpoints
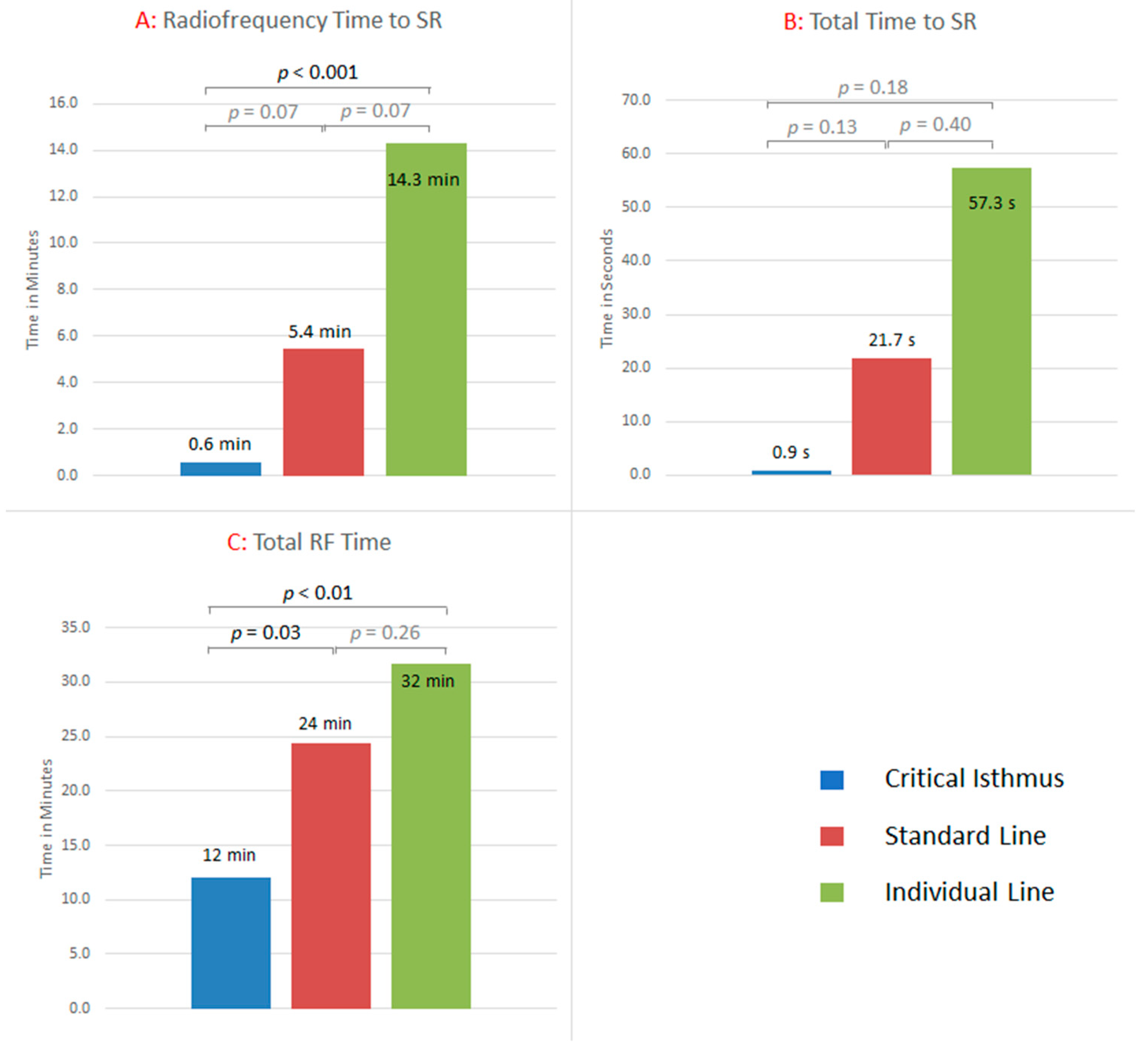
3.4.1. Termination into SR during CA
3.4.2. Time to Termination
3.4.3. Non-Inducibility of Any Type of Arrhythmia
3.4.4. Learning Curve
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Granada, J.; Uribe, W.; Chyou, P.-H.; Maassen, K.; Vierkant, R.; Smith, P.N.; Hayes, J.; Eaker, E.; Vidaillet, H. Incidence and predictors of atrial flutter in the general population. J. Am. Coll. Cardiol. 2000, 36, 2242–2246. [Google Scholar] [CrossRef] [Green Version]
- Elesber, A.A.; Rosales, A.G.; Herges, R.M.; Shen, W.-K.; Moon, B.S.; Malouf, J.F.; Ammash, N.M.; Somers, V.; Hodge, D.O.; Gersh, B.J.; et al. Relapse and mortality following cardioversion of new-onset vs. recurrent atrial fibrillation and atrial flutter in the elderly. Eur. Hear. J. 2006, 27, 854–860. [Google Scholar] [CrossRef] [Green Version]
- Gerstenfeld, E.P.; Callans, D.J.; Dixit, S.; Russo, A.M.; Nayak, H.; Lin, D.; Pulliam, W.; Siddique, S.; Marchlinski, F. Mechanisms of Organized Left Atrial Tachycardias Occurring After Pulmonary Vein Isolation. Circulation 2004, 110, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Gucuk Ipek, E.; Marine, J.E.; Habibi, M.; Chrispin, J.; Lima, J.; Rickard, J.; Spragg, D.; Zimmerman, S.L.; Zipunnikov, V.; Berger, R.; et al. Association of left atrial function with incident atypical atrial flutter after atrial fibrillation ablation. Heart Rhythm. 2016, 13, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chugh, A.; Oral, H.; Lemola, K.; Hall, B.; Cheung, P.; Good, E.; Tamirisa, K.; Han, J.; Bogun, F.; Pelosi, F.; et al. Prevalence, mechanisms, and clinical significance of macroreentrant atrial tachycardia during and following left atrial ablation for atrial fibrillation. Hear. Rhythm 2005, 2, 464–471. [Google Scholar] [CrossRef]
- Page, R.L.; Joglar, J.A.; Caldwell, M.A.; Calkins, H.; Conti, J.B.; Deal, B.J.; Estes, N.A.M.; Field, M.E.; Goldberger, Z.D.; Hammill, S.C.; et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2016, 133, e506–e574. [Google Scholar] [CrossRef]
- Ferrero de Loma-Osorio, Á.; Díaz-Infante, E.; Macías Gallego, A. Spanish Catheter Ablation Registry. 12th Official Report of the Spanish Society of Cardiology Working Group on Electrophysiology and Arrhythmias (2012). Revista Española Cardiología 2013, 66, 983–992. [Google Scholar] [CrossRef]
- Baker, B.M.; Lindsay, B.D.; Bromberg, B.I.; Frazier, D.W.; Cain, M.E.; Smith, J.M. Catheter ablation of clinical intraatrial reentrant tachycardias resulting from previous atrial surgery: Localizing and transecting the critical isthmus. J. Am. Coll. Cardiol. 1996, 28, 411–417. [Google Scholar] [CrossRef]
- Triedman, J.K.; Bergau, D.M.; Saul, J.; Epstein, M.R.; Walsh, E.P. Efficacy of Radiofrequency Ablation for Control of Intraatrial Reentrant Tachycardia in Patients With Congenital Heart Disease. J. Am. Coll. Cardiol. 1997, 30, 1032–1038. [Google Scholar] [CrossRef] [Green Version]
- Chan, D.P.; Van Hare, G.F.; Mackall, J.A.; Carlson, M.D.; Waldo, A.L. Importance of Atrial Flutter Isthmus in Postoperative Intra-Atrial Reentrant Tachycardia. Circulation 2000, 102, 1283–1289. [Google Scholar] [CrossRef] [Green Version]
- Jaïs, P.; Shah, D.C.; Haïssaguerre, M.; Hocini, M.; Tian Peng, J.; Takahashi, A.; Garrigue, S.; le Métayer, P.; Clémenty, J. Mapping and Ablation of Left Atrial Flutters. Circulation 2000, 101, 2928–2934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akar, J.G.; Kok, L.C.; Haines, D.E.; DiMarco, J.P.; Mounsey, J. Coexistence of type I atrial flutter and intra-atrial re-entrant tachycardia in patients with surgically corrected congenital heart disease. J. Am. Coll. Cardiol. 2001, 38, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, H.; Shah, N.; Matsudaira, K.; Overholt, E.; Chandrasekaran, K.; Beckman, K.J.; Spector, P.; Calame, J.D.; Rao, A.; Otomo, K.; et al. Characterization of Reentrant Circuit in Macroreentrant Right Atrial Tachycardia After Surgical Repair of Congenital Heart Disease Isolated Channels Between Scars Allow “Focal” Ablation. Circulation 2001, 103, 699–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffey, J.O.; D’avila, A.; Dukkipati, S.; Danik, S.B.; Gangireddy, S.R.; Koruth, J.S.; Miller, M.A.; Sager, S.J.; Eggert, C.A.; Reddy, V.Y. Catheter ablation of scar-related atypical atrial flutter. Europace 2013, 15, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, I.H.; Kistler, P.M.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Morton, J.B.; Kalman, J.M. Scar-related right atrial macroreentrant tachycardia in patients without prioratrial surgery: Electroanatomic characterization and ablation outcome. Heart Rhythm 2005, 2, 594–601. [Google Scholar] [CrossRef]
- Winkle, R.A.; Moskovitz, R.; Mead, R.H.; Engel, G.; Kong, M.H.; Fleming, W.; Patrawala, R.A. Ablation of atypical atrial flutters using ultra high density-activation sequence mapping. J. Interv. Card. Electrophysiol. 2017, 48, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Jaïs, P.; Hocini, M.; Weerasoryia, R.; Macle, L.; Scavee, C.; Raybaud, F.; Shah, D.C.; Clémenty, J.; Haïssaguerre, M. Atypical left atrial flutters. Kluwer Acad. Publ. 2002, 6, 371–377. [Google Scholar] [CrossRef]
- Bun, S.-S.; Latcu, D.G.; Marchlinski, F.; Saoudi, N. Atrial flutter: More than just one of a kind. Eur. Heart J. 2015, 36, 2356–2363. [Google Scholar] [CrossRef] [Green Version]
- Pedrinazzi, C.; Durin, O.; Mascioli, G.; Curnis, A.; Raddino, R.; Inama, G.; Cas, L.D. Atrial Flutter: From ECG to Electroanatomical 3D Mapping. Heart Int. 2006, 2. [Google Scholar] [CrossRef]
- Sundaram, S.; Choe, W.; Jordan, J.R.; Mullins, N.; Boorman, C.; Kessler, E.J.; Nath, S. Catheter ablation of atypical atrial flutter: A novel 3D anatomic mapping approach to quickly localize and terminate atypical atrial flutter. J. Interv. Card. Electrophysiol. 2017, 49, 307–318. [Google Scholar] [CrossRef]
- Patel, A.M.; d’Avila, A.; Neuzil, P.; Kim, S.J.; Mela, T.; Singh, J.P.; Ruskin, J.N.; Reddy, V.Y. Atrial tachycardia after ablation of persistent atrial fibrillation: Identification of the critical isthmus with a combination of multielectrode activation mapping and targeted entrainment mapping. Circ. Arrhythmia Electrophysiol. 2008, 1, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, W.; Yang, B.; Chen, H.; Zhang, F.; Gu, K.; Yu, J.; Li, M.; Yang, G.; Cao, K.; Chen, M. Mapping of focal atrial tachycardia with an uninterpretable activation map after extensive atrial ablation: Tricks and tips. Circ. Arrhythmia Electrophysiol. 2014, 7, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, B.; Stevenson, W.G. Entrainment mapping: Theoretical considerations and practical implementation. J. Cardiovasc. Electrophysiol. 2017, 29, 204–213. [Google Scholar] [CrossRef] [Green Version]
- Takigawa, M.; Derval, N.; Frontera, A.; Martin, R.; Yamashita, S.; Cheniti, G.; Vlachos, K.; Thompson, N.; Kitamura, T.; Wolf, M.; et al. Revisiting anatomic macroreentrant tachycardia after atrial fibrillation ablation using ultrahigh-resolution mapping: Implications for ablation. Heart Rhythm. 2018, 15, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Laţcu, D.G.; Bun, S.-S.; Viera, F.; Delassi, T.; El Jamili, M.; Al Amoura, A.; Saoudi, N. Selection of Critical Isthmus in Scar-Related Atrial Tachycardia Using a New Automated Ultrahigh Resolution Mapping System. Circ. Arrhythmia Electrophysiol. 2017, 10, e004510. [Google Scholar] [CrossRef] [PubMed]
- De Ponti, R.; Verlato, R.; Bertaglia, E.; Del Greco, M.; Fusco, A.; Bottoni, N.; Drago, F.; Sciarra, L.; Ometto, R.; Mantovan, R.; et al. Treatment of macro-re-entrant atrial tachycardia based on electroanatomic mapping: Identification and ablation of the mid-diastolic isthmus. Europace 2007, 9, 449–457. [Google Scholar] [CrossRef]
- Kuck, K.; Böcker, D.; Chun, J.; Deneke, T.; Hindricks, G.; Hoffmann, E.; Piorkowski, C.; Willems, S. Qualitätskriterien zur Durchführung der Katheterablation von Vorhofflimmern. Kardiologe 2017, 11, 161–182. [Google Scholar] [CrossRef]
- Jaïs, P.; Matsuo, S.; Knecht, S.; Weerasooriya, R.; Hocini, M.; Sacher, F.; Wright, M.; Nault, I.; Lellouche, N.; Klein, G.; et al. A Deductive Mapping Strategy for Atrial Tachycardia Following Atrial Fibrillation Ablation: Importance of Localized Reentry. J. Cardiovasc. Electrophysiol. 2009, 20, 480–491. [Google Scholar] [CrossRef]
- Sanders, P.; Hocini, M.; Jaïs, P.; Hsu, L.-F.; Takahashi, Y.; Rotter, M.; Scavée, C.; Pasquié, J.-L.; Sacher, F.; Rostock, T.; et al. Characterization of Focal Atrial Tachycardia Using High-Density Mapping. J. Am. Coll. Cardiol. 2005, 46, 2088–2099. [Google Scholar] [CrossRef]
- Saoudi, N.; Cosio, F.; Waldo, A.E.A.; Chen, S.A.; Iesaka, Y.; Lesh, M.; Saksena, S.; Salerno, J.; Schoels, W. Classification of Atrial Flutter and Regular Atrial Tachycardia According to Electrophysiologic Mechanism and Anatomic Bases. J. Cardiovasc. Electrophysiol. 2001, 12, 852–866. [Google Scholar] [CrossRef]
- Rostock, T.; Drewitz, I.; Steven, D.; Hoffmann, B.A.; Salukhe, T.V.; Bock, K.; Servatius, H.; Aydin, M.A.; Meinertz, T.; Willems, S. Characterization, Mapping, and Catheter Ablation of Recurrent Atrial Tachycardias After Stepwise Ablation of Long-Lasting Persistent Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2010, 3, 160–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narayan, S.M.; Krummen, D.E. Targeting Stable Rotors to Treat Atrial Fibrillation. Arrhythm. Electrophysiol. Rev. 2012, 1, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaïs, P.; Hocini, M.; Hsu, L.-F.; Sanders, P.; Scavee, C.; Weerasooriya, R.; Macle, L.; Raybaud, F.; Garrigue, S.; Shah, D.C.; et al. Technique and Results of Linear Ablation at the Mitral Isthmus. Circulation 2004, 110, 2996–3002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzeis, S.; Luik, A.; Jilek, C.; Schmitt, C.; Estner, H.L.; Wu, J.; Reents, T.; Fichtner, S.; Kolb, C.; Karch, M.R.; et al. The Modified Anterior Line: An Alternative Linear Lesion in Perimitral Flutter. J. Cardiovasc. Electrophysiol. 2010, 21, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Ammar, S.; Luik, A.; Hessling, G.; Bruhm, A.; Reents, T.; Semmler, V.; Buiatti, A.; Kathan, S.; Hofmann, M.; Kolb, C.; et al. Ablation of perimitral flutter: Acute and long-term success of the modified anterior line. Europace 2015, 17, 447–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, M.; Luik, A.; Shepherd, E.; Sulkin, M.; Laughner, J.; Duffy, E.; Oesterlein, T.; Meyer, C.; Jais, P.; Duchateau, J.; et al. Local catheter impedance drop during pulmonary vein isolation predicts conduction block in patients with paroxysmal atrial fibrillation: Initial results of the LOCALIZE clinical trial. Europace 2020, 22, euaa162.249. Available online: https://academic.oup.com/europace/article/22/Supplement_1/euaa162.249/5858672 (accessed on 18 October 2021). [CrossRef]
- Munro, J.; Shen, W.-K.; Ru-Xing, W. A practical approach to atypical atrial flutter. J. Pract. Electrophysiol. 2015, 24, 229–244. [Google Scholar]
- Ghannam, M.; Chugh, A. Utility of the Electrocardiogram in Mapping of Atrial Tachycardia Post-Atrial Fibrillation Ablation: Back to the Basics. JACC Clin. Electrophysiol. 2018, 4, 46–48. [Google Scholar] [CrossRef]
- Van Marion, D.M.S.; Lanters, E.A.H.; Wiersma, M.; Allessie, M.A.; Brundel, B.B.J.J.M.; de Groot, N.M.S. Diagnosis and Therapy of Atrial Fibrillation: The Past, the Present and the Future. J. Atrial Fibrillation 2015, 8, 51–60. [Google Scholar]
- Schaeffer, B.; Hoffmann, B.A.; Meyer, C.; Akbulak, R.; Moser, J.; Jularic, M.; Eickholt, C.; Nührich, J.M.; Kuklik, P.; Willems, S. Characterization, Mapping, and Ablation of Complex Atrial Tachycardia: Initial Experience With a Novel Method of Ultra High-Density 3D Mapping. J. Cardiovasc. Electrophysiol. 2016, 27, 1139–1150. [Google Scholar] [CrossRef]
- Jungen, C.; Akbulak, R.; Kahle, A.; Eickholt, C.; Schaeffer, B.; Scherschel, K.; Dinshaw, L.; Muenkler, P.; Schleberger, R.; Nies, M.; et al. Outcome after tailored catheter ablation of atrial tachycardia using ultra-high-density mapping. J. Cardiovasc. Electrophysiol. 2020, 31, 2645–2652. [Google Scholar] [CrossRef] [PubMed]
- Derval, N.; Takigawa, M.; Frontera, A.; Mahida, S.; Konstantinos, V.; Denis, A.; Duchateau, J.; Pillois, X.; Yamashita, S.; Berte, B.; et al. Characterization of Complex Atrial Tachycardia in Patients With Previous Atrial Interventions Using High-Resolution Mapping. JACC Clin. Electrophysiol. 2020, 6, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Ng, F.S.; Guerrero, F.; Luther, V.; Sikkel, M.; Lim, P.B. Microreentrant left atrial tachycardia circuit mapped with an ultra-high-density mapping system. Heart Rhythm Case Rep. 2017, 3, 224–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oesterlein, T.G.; Loewe, A.; Lenis, G.; Luik, A.; Schmitt, C.; Doessel, O. Automatic Identification of Reentry Mechanisms and Critical Sites During Atrial Tachycardia by Analyzing Areas of Activity. IEEE Trans. Biomed. Eng. 2018, 65, 2334–2344. [Google Scholar] [CrossRef]
- Loewe, A.; Poremba, E.; Oesterlein, T.; Luik, A.; Schmitt, C.; Seemann, G.; Dössel, O. Patient-Specific Identification of Atrial Flutter Vulnerability–A Computational Approach to Reveal Latent Reentry Pathways. Front. Physiol. 2019, 9, 1910. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics Index Procedure | Mean ± SD or Total (%) n = 35 |
|---|---|
| Age (years) | 65 ± 7 |
| Gender, female (n) | 12 (40%) |
| Hypertension (n) | 26 (87%) |
| CAD (n) | 8 (27%) |
| Diabetes mellitus (n) | 3 (10%) |
| LVEF < 50% | 7 (20%) |
| CHA2DS2-VASc | 2 ±1 |
| LA size (mm) | 43 ± 6 |
| LA area (cm2) | 23 ± 5 |
| AAD | |
| Betablocker (n) | 21 (60%) |
| Amiodarone (n) | 6 (17%) |
| Other (n) | 0 (0%) |
| Number of prior left LA procedures (n) | 2 ± 1 |
| Time since last LA ablation (months) | 18 ± 23 |
| Prior LA-AT ablation (n) | 13 (37%) |
| Prior LA ablation approaches (n) | |
| PVI only (n) | 10 (29%) |
| PVI + CFAE(n) | 5 (14%) |
| PVI + LA-Lines (n) | 9 (26%) |
| PVI + CFAE + Lines (n) | 8 (23%) |
| PVI + Rotor (n) | 3 (9%) |
| Prior CTI ablation (n) | 15 (43%) |
| Procedural Data | n = 35 |
|---|---|
| Termination in SR (n) | 35 (100%) |
| Termination in SR upon 1st ablation strategy (n) | 32 (91%) |
| Total RF time (min) | 24 ± 16 |
| Total procedure time (min) | 193 ± 57 |
| Total fluoro time (min) | 12 ± 8 |
| Total fluoro dosage (cGycm2) | 621 ± 555 |
| Non-inducibility (n) | 30 (86%) |
| Follow-up time (months) | 30 ± 13 |
| Complications (n) | 2 (6%) |
| Minor | 2 (6%) |
| Major | 0 (0%) |
| Ablation strategy (n) | |
| Standard line | 7 (20%) |
| Individual line | 15 (43%) |
| Critical isthmus | 13 (37%) |
| Focal | 0 (0%) |
| Local area | 0 (0%) |
| Total time to SR (min) | 21 ± 57 |
| Standard line | 57 ± 100 |
| Individual line | 22 ± 49 |
| Critical isthmus | 1 ± 1 |
| RF time to SR (min) | 5 ± 9 |
| Standard line | 14 ± 12 |
| Individual line | 5 ± 9 |
| Critical isthmus | 1 ± 1 |
| Total RF applications to SR (n) | 6 ± 9 |
| Standard line | 16 ± 13 |
| Individual line | 6 ± 9 |
| Critical isthmus | 1 ± 1 |
| Mapping Data | n = 35 |
|---|---|
| AT cycle length (ms) | 297 ± 86 |
| P-wave duration in AT (ms) | 117 ± 32 |
| ATs mapped (n)/patient | 1 ± 1 |
| Points per map (n) | 20,773 ± 9748 |
| LA volume (mL) | 188 ± 48 |
| Mapping time (min) | 27 ± 10 |
| Dominant reentry defined (n) | 33 (94%) |
| Critical isthmus present (n) | 31 (89%) |
| Type of AT (n) | |
| Macro | 31 (88%) |
| Small area | 1 (3%) |
| Micro | 3 (9%) |
| Focal | 0 (0.0 %) |
| Rotor | 0 (0.0 %) |
| PV-reconnection (n) | 47 (33 %) |
| PV-reconnection per patient (n) | 1.6 ± 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luik, A.; Schmidt, K.; Haas, A.; Unger, L.; Tzamalis, P.; Brüggenjürgen, B. Ablation of Left Atrial Tachycardia following Catheter Ablation of Atrial Fibrillation: 12-Month Success Rates. J. Clin. Med. 2022, 11, 1047. https://doi.org/10.3390/jcm11041047
Luik A, Schmidt K, Haas A, Unger L, Tzamalis P, Brüggenjürgen B. Ablation of Left Atrial Tachycardia following Catheter Ablation of Atrial Fibrillation: 12-Month Success Rates. Journal of Clinical Medicine. 2022; 11(4):1047. https://doi.org/10.3390/jcm11041047
Chicago/Turabian StyleLuik, Armin, Kerstin Schmidt, Annika Haas, Laura Unger, Panagiotis Tzamalis, and Bernd Brüggenjürgen. 2022. "Ablation of Left Atrial Tachycardia following Catheter Ablation of Atrial Fibrillation: 12-Month Success Rates" Journal of Clinical Medicine 11, no. 4: 1047. https://doi.org/10.3390/jcm11041047