
Ten Sessions of 30 Min tDCS over 5 Days to Achieve Remission in Depression: A Randomized Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
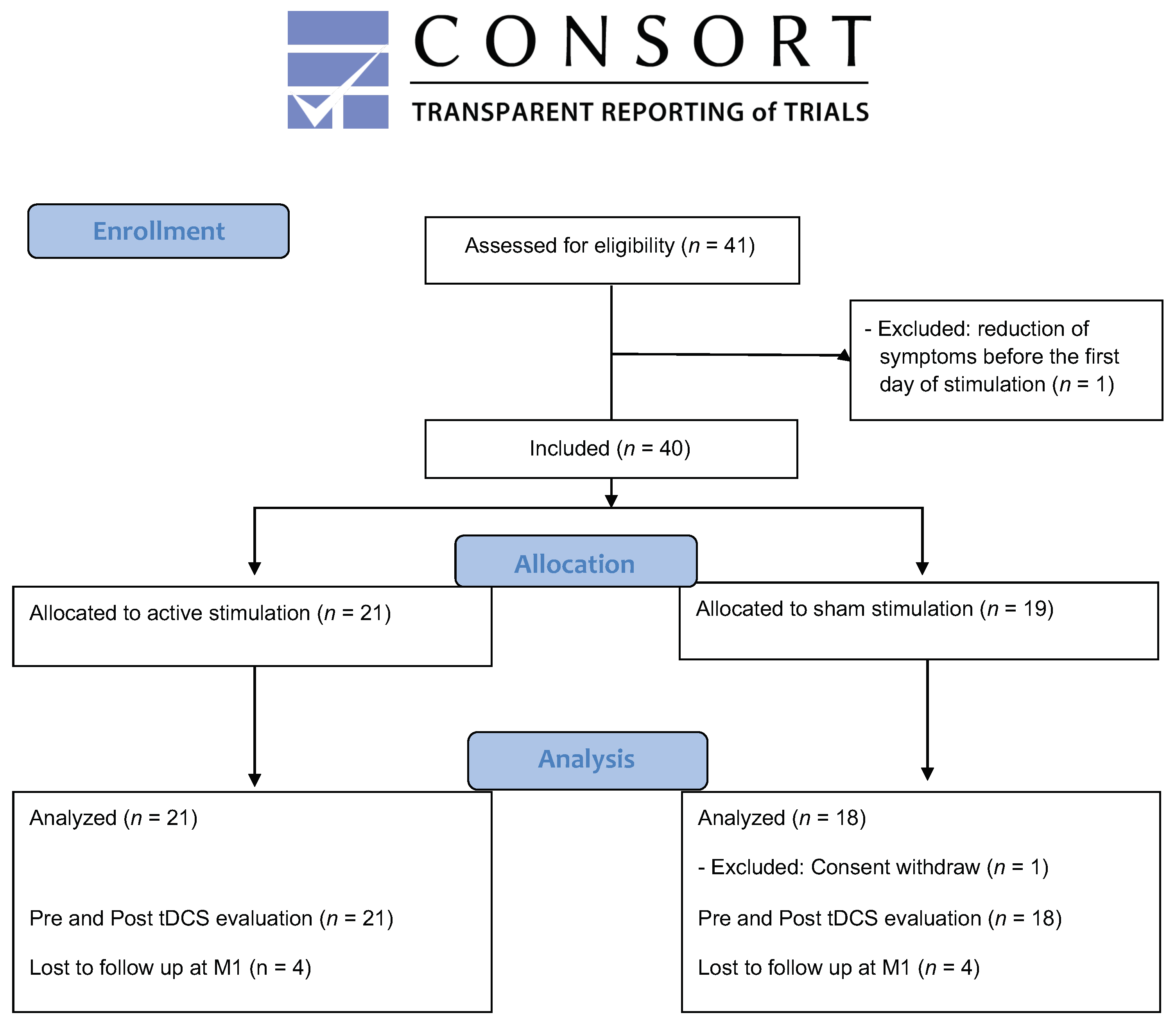
2.1. Sample
2.2. Stimulation Procedure
2.3. Statistical Analysis
3. Results
3.1. Primary Outcome Analysis
3.2. Secondary Outcome Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Statistics 2017: Monitoring Health for the SDGs, Sustainable Development Goals. 2017. Available online: https://apps.who.int/iris/handle/10665/255336 (accessed on 2 September 2021).
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.; Vos, T.; Whiteford, H.A. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moffa, A.H.; Martin, D.; Alonzo, A.; Bennabi, D.; Blumberger, D.M.; Benseñor, I.M.; Daskalakis, Z.; Fregni, F.; Haffen, E.; Lisanby, S.H.; et al. Efficacy and acceptability of transcranial direct current stimulation (tDCS) for major depressive disorder: An individual patient data meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 99, 109836. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runoni, A.R.; Moffa, A.H.; Sampaio-Junior, B.; Borrione, L.; Moreno, M.L.; Fernandes, R.A.; Veronezi, B.P.; Nogueira, B.S.; Aparicio, L.V.; Razza, L.B.; et al. Trial of Electrical Direct-Current Therapy versus Escitalopram for Depression. N. Engl. J. Med. 2017, 376, 2523–2533. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; El-Hagrassy, M.M.; Pacheco-Barrios, K.; Carvalho, S.; Leite, J.; Simis, M.; Brunelin, J.; Nakamura-Palacios, E.M.; Marangolo, P.; Venkatasubramanian, G.; et al. Evidence-Based Guidelines and Secondary Meta-Analysis for the Use of Transcranial Direct Current Stimulation in Neurological and Psychiatric Disorders. Int. J. Neuropsychopharmacol. 2021, 24, 256–313. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Lam, C.L.; Peng, X.; Zhang, D.; Zhang, C.; Huang, R.; Lee, T.M. Efficacy and acceptability of transcranial direct current stimulation for treating depression: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 126, 481–490. [Google Scholar] [CrossRef]
- Palm, U.; Leitner, B.; Strube, W.; Hasan, A.; Padberg, F. Safety of Repeated Twice-daily 30 Minutes of 2 mA tDCS in Depressed Patients. Int. Neuropsychiatr. Dis. J. 2015, 4, 168–171. [Google Scholar] [CrossRef] [Green Version]
- Zanardi, R.; Poletti, S.; Prestifilippo, D.; Attanasio, F.; Barbini, B.; Colombo, C. Transcranial direct current stimulation: A novel approach in the treatment of vascular depression. Brain Stimul. 2020, 13, 1559–1565. [Google Scholar] [CrossRef]
- Zimmerman, M.; Posternak, M.A.; Chelminski, I. Defining remission on the Montgomery-Asberg depression rating scale. J. Clin. Psychiatry 2004, 65, 163–168. [Google Scholar] [CrossRef]
- De Smet, S.; Nikolin, S.; Moffa, A.; Suen, P.; Vanderhasselt, M.A.; Brunoni, A.R.; Razza, L.B. Determinants of sham response in tDCS depression trials: A systematic review and meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110261. [Google Scholar] [CrossRef] [PubMed]
- Fonteneau, C.; Mondino, M.; Arns, M.; Baeken, C.; Bikson, M.; Brunoni, A.R.; Burke, M.J.; Neuvonen, T.; Padberg, F.; Pascual-Leone, A.; et al. Sham tDCS: A hidden source of variability? Reflections for further blinded, controlled trials. Brain Stimul. 2019, 12, 668–673. [Google Scholar] [CrossRef]
- Li, M.S.; Du, H.D.; Chu, H.C.; Liao, Y.Y.; Pan, W.; Li, Z.; Hung, G.C.L. Delayed effect of bifrontal transcranial direct current stimulation in patients with treatment-resistant depression: A pilot study. BMC Psychiatry 2019, 19, 180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duprat, R.; Desmyter, S.; Rudi, D.R.; van Heeringen, K.; Abbeele, D.V.D.; Tandt, H.; Bakic, J.; Pourtois, G.; Dedoncker, J.; Vervaet, M.; et al. Accelerated intermittent theta burst stimulation treatment in medication-resistant major depression: A fast road to remission? J. Affect. Disord. 2016, 200, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Bation, R.; Magnin, C.; Poulet, E.; Mondino, M.; Brunelin, J. Intermittent theta burst stimulation for negative symptoms of schizophrenia—A double-blind, sham-controlled pilot study. NPJ Schizophr. 2021, 7, 10. [Google Scholar] [CrossRef]
- Maslej, M.M.; Furukawa, T.A.; Cipriani, A.; Andrews, P.W.; Sanches, M.; Tomlinson, A.; Volkmann, C.; McCutcheon, R.A.; Howes, O.; Guo, X.; et al. Individual Differences in Response to Antidepressants. JAMA Psychiatry 2021, 78, 490. [Google Scholar] [CrossRef]
- Rezaei, M.; Shariat Bagheri, M.M.; Ahmadi, M. Clinical and demographic predictors of response to anodal tDCS treatment in major depression disorder (MDD). J. Psychiatr. Res. 2021, 138, 68–74. [Google Scholar] [CrossRef]
- Mondino, M.; Fonteneau, C.; Simon, L.; Dondé, C.; Haesebaert, F.; Poulet, E.; Brunelin, J. Advancing clinical response characterization to frontotemporal transcranial direct current stimulation with electric field distribution in patients with schizophrenia and auditory hallucinations: A pilot study. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 85–92. [Google Scholar] [CrossRef]
- Kurzeck, A.K.; Dechantsreiter, E.; Wilkening, A.; Kumpf, U.; Nenov-Matt, T.; Padberg, F.; Palm, U. Transcranial Direct Current Stimulation (tDCS) for Depression during Pregnancy: Results from an Open-Label Pilot Study. Brain Sci. 2021, 11, 947. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Ferrucci, R.; Bortolomasi, M.; Vergari, M.; Tadini, L.; Boggio, P.S.; Giacopuzzi, M.; Barbieri, S.; Priori, A. Transcranial direct current stimulation (tDCS) in unipolar vs. bipolar depressive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 96–101. [Google Scholar] [CrossRef]
- Brunelin, J.; Mondino, M.; Gassab, L.; Haesebaert, F.; Gaha, L.; Suaud-Chagny, M.F.; Saoud, M.; Mechri, A.; Poulet, E. Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Am. J. Psychiatry 2012, 169, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Bennabi, D.; Nicolier, M.; Monnin, J.; Tio, G.; Pazart, L.; Vandel, P.; Haffen, E. Pilot study of feasibility of the effect of treatment with tDCS in patients suffering from treatment-resistant depression treated with escitalopram. Clin. Neurophysiol. 2015, 126, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S.; et al. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monte-Silva, K.; Kuo, M.F.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Shaping the optimal repetition interval for cathodal transcranial direct current stimulation (tDCS). J. Neurophysiol. 2010, 103, 1735–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monte-Silva, K.; Kuo, M.F.; Hessenthaler, S.; Fresnoza, S.; Liebetanz, D.; Paulus, W.; Nitsche, M.A. Induction of late LTP-like plasticity in the human motor cortex by repeated non-invasive brain stimulation. Brain Stimul. 2013, 6, 424–432. [Google Scholar] [CrossRef]
- Mondino, M.; Poulet, E.; Brunelin, J. Moving to accelerated protocols of tDCS in schizophrenia: A case report. Brain Stimul. 2021, 14, 822–824. [Google Scholar] [CrossRef]
- Kim, J.; Iwata, Y.; Plitman, E.; Caravaggio, F.; Chung, J.K.; Shah, P.; Blumberger, D.M.; Pollock, B.G.; Remington, G.; Graff-Guerrero, A.; et al. A meta-analysis of transcranial direct current stimulation for schizophrenia: “Is more better?”. J. Psychiatr. Res. 2019, 110, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Moffa, A.H.; Fregni, F.; Palm, U.; Padberg, F.; Blumberger, D.M.; Daskalakis, Z.J.; Bennabi, D.; Haffen, E.; Alonzo, A.; et al. Transcranial direct current stimulation for acute major depressive episodes: Meta-analysis of individual patient data. Br. J. Psychiatry 2016, 208, 522–531. [Google Scholar] [CrossRef] [Green Version]
- Cole, E.J.; Phillips, A.L.; Bentzley, B.S.; Stimpson, K.H.; Nejad, R.; Barmak, F.; Veerapal, C.; Khan, N.; Cherian, K.; Felber, E.; et al. Stanford Neuromodulation Therapy (SNT): A Double-Blind Randomized Controlled Trial. Am. J. Psychiatry 2021, 179, 132–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sham tDCS | Active tDCS | p | |
|---|---|---|---|
| n | 18 | 21 | |
| Age (years) | 51.5 (9.7) | 48.1 (9.3) | 0.272 |
| Education | 15.0 (3.1) | 13.5 (2.8) | 0.129 |
| Sex (F/M) | 12/6 | 12/9 | 0.542 |
| Episode duration (months) | 15.86 (14.7) | 21.43 (14.8) | 0.138 |
| Illness duration (years) | 22.5 (13.7) | 21.8 (12.0) | 0.878 |
| MADRS10 | 26.8 (5.1) | 27.0 (4.9) | 0.918 |
| Maudsley | 6.5 (3.5) | 7.7 (2.5) | 0.243 |
| Antidepressant medication | |||
| SSRIs | 11 | 13 | 1.000 |
| SNRIs | 5 | 8 | 0.734 |
| TCAs | 6 | 5 | 0.723 |
| MAOIs | 1 | 1 | 1.000 |
| Other medication | |||
| BZD | 5 | 4 | 0.706 |
| Antipsychotics | 2 | 4 | 0.667 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moirand, R.; Imbert, L.; Haesebaert, F.; Chesnoy, G.; Bediou, B.; Poulet, E.; Brunelin, J. Ten Sessions of 30 Min tDCS over 5 Days to Achieve Remission in Depression: A Randomized Pilot Study. J. Clin. Med. 2022, 11, 782. https://doi.org/10.3390/jcm11030782
Moirand R, Imbert L, Haesebaert F, Chesnoy G, Bediou B, Poulet E, Brunelin J. Ten Sessions of 30 Min tDCS over 5 Days to Achieve Remission in Depression: A Randomized Pilot Study. Journal of Clinical Medicine. 2022; 11(3):782. https://doi.org/10.3390/jcm11030782
Chicago/Turabian StyleMoirand, Rémi, Laetitia Imbert, Frédéric Haesebaert, Gabrielle Chesnoy, Benoit Bediou, Emmanuel Poulet, and Jérôme Brunelin. 2022. "Ten Sessions of 30 Min tDCS over 5 Days to Achieve Remission in Depression: A Randomized Pilot Study" Journal of Clinical Medicine 11, no. 3: 782. https://doi.org/10.3390/jcm11030782