
Predictors of Mortality and Cardiovascular Outcome at 6 Months after Hospitalization for COVID-19

 , , , , , , , , , , , ,
, , , , , , , , , , , ,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
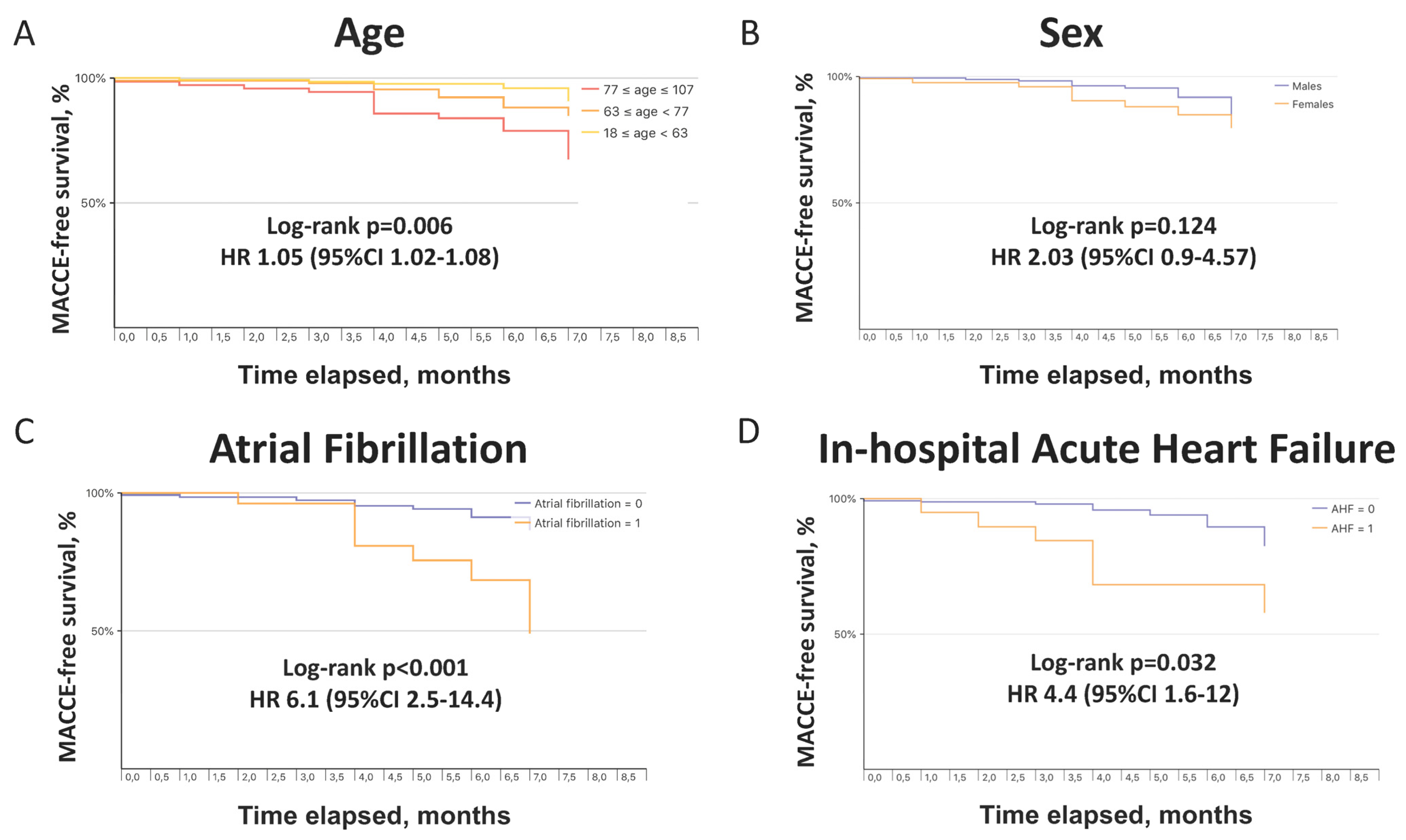
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Weekly Epidemiological Update. 6 April 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---6-april-2021 (accessed on 6 April 2021).
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Mennuni, M.G.; Renda, G.; Grisafi, L.; Rognoni, A.; Colombo, C.; Lio, V.; Foglietta, M.; Petrilli, I.; Pirisi, M.; Spinoni, E.; et al. Clinical outcome with different doses of low-molecular-weight heparin in patients hospitalized for COVID-19. J. Thromb. Thrombolysis 2021, 52, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Navaratnam, A.V.; Gray, W.K.; Day, J.; Wendon, J.; Briggs, T.W.R. Patient factors and temporal trends associated with COVID-19 in-hospital mortality in England: An observational study using administrative data. Lancet Respir. Med. 2021, 9, 397–406. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated with In-Hospital Mortality in a US National Sample of Patients with COVID-19. JAMA Netw. Open 2020, 3, e2029058. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Baricich, A.; Borg, M.B.; Cuneo, D.; Cadario, E.; Azzolina, D.; Balbo, P.E.; Bellan, M.; Zeppegno, P.; Pirisi, M.; Cisari, C.; et al. Midterm functional sequelae and implications in rehabilitation after COVID19. A cross-sectional study. Eur. J. Phys. Rehabil. Med. 2021, 57, 199–207. [Google Scholar] [CrossRef]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae among Patients with COVID-19 Four Months after Hospital Discharge. JAMA Netw. Open 2021, 4, e2036142. [Google Scholar] [CrossRef]
- Carfi, A.; Bernabei, R.; Landi, F.; For the Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef] [PubMed]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiological Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Wang, X.Q.; Iwashyna, T.J.; Prescott, H.C. Readmission and Death after Initial Hospital Discharge among Patients with COVID-19 in a Large Multihospital System. JAMA 2021, 325, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-covid syndrome in individuals admitted to hospital with covid-19: Retrospective cohort study. BMJ 2021, 372, n693. [Google Scholar] [CrossRef] [PubMed]
- Günster, C.; Busse, R.; Spoden, M.; Rombey, T.; Schillinger, G.; Hoffmann, W.; Weber-Carstens, S.; Schuppert, A.; Karagiannidis, C. 6-month mortality and readmissions of hospitalized COVID-19 patients: A nationwide cohort study of 8679 patients in Germany. PLoS ONE 2021, 16, e0255427. [Google Scholar] [CrossRef]
- Estimates. 1950–2020: Annually Interpolated Demographic Indicators—Crude Death Rate (Deaths per 1000 Population). Available online: https://population.un.org/wpp2019/Download/Standard/Interpolated/ (accessed on 6 April 2021).
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and cardiac arrhythmias. Heart Rhythm 2020, 17, 1439–1444. [Google Scholar] [CrossRef] [PubMed]
- Spinoni, E.G.; Mennuni, M.; Rognoni, A.; Grisafi, L.; Colombo, C.; Lio, V.; Renda, G.; Foglietta, M.; Petrilli, I.; D’Ardes, D.; et al. Contribution of Atrial Fibrillation to In-Hospital Mortality in Patients with COVID-19. Circ. Arrhythm. Electrophysiol. 2021, 14, e009375. [Google Scholar] [CrossRef]
- Stone, E.; Kiat, H.; McLachlan, C.S. Atrial fibrillation in COVID-19: A review of possible mechanisms. FASEB J. 2020, 34, 11347–11354. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 296) | Deceased during Follow-Up (n = 14) | Survivors (n = 282) | p Value | MACCE during Follow-Up (n = 21) | No MACCE (n = 275) | p Value | |
|---|---|---|---|---|---|---|---|
| Baseline characteristics | |||||||
| Age—year, mean ± SD | 64 ± 16 | 77 ± 14 | 64 ± 16 | 0.002 | 75 ± 17 | 63 ± 16 | 0.002 |
| Male sex, n (%) | 172 (58) | 7 (50) | 165 (59) | 0.585 | 8 (38) | 161 (59) | 0.107 |
| Caucasian, n (%) | 246 (93) | 12 (86) | 234 (83) | 0.568 | 18 (86) | 224 (81) | 0.776 |
| Weight—kg, mean ± SD | 76 ± 14 | 68 ± 12 | 77 ± 14 | 0.126 | 72 ± 10 | 77 ± 14 | 0.219 |
| BMI, mean ± SD | 27 ± 4 | 24 ± 3 | 27 ± 4 | 0.244 | 27 ± 4 | 27 ± 4 | 0.999 |
| Arterial hypertension, n (%) | 149 (50) | 9 (64) | 140 (50) | 0.413 | 10 (48) | 137 (50) | 0.999 |
| Dyslipidemia, n (%) | 59 (20) | 1(7) | 58 (21) | 0.316 | 6 (29) | 53 (19) | 0.392 |
| Diabetes mellitus, n (%) | 53 (18) | 4 (29) | 49 (17) | 0.287 | 3 (14) | 51 (18) | 0.776 |
| Current smoking, n (%) | 25 (8) | 2 (14) | 23 (8) | 0.335 | 4 (19) | 25 (9) | 0.137 |
| Cardiomyopathy, n (%) | 51 (17) | 5 (36) | 46 (16) | 0.073 | 6 (29) | 45 (16) | 0.224 |
| Previous PCI, n (%) | 24 (8) | 1 (7) | 23 (8) | 0.999 | 3 (14) | 22 (8) | 0.402 |
| Previous CABG, n (%) | 4 (1) | 0 (0) | 4 (1) | 0.823 | 0 (0) | 5 (2) | 0.999 |
| AF, n (%) | 18 (6) | 3 (21) | 15 (5) | 0.045 | 4 (19) | 14 (5) | 0.030 |
| PAD, n (%) | 30 (10) | 4 (29) | 26 (9) | 0.042 | 6 (28) | 27 (10) | 0.019 |
| COPD, n (%) | 24 (8) | 0 (0) | 24 (8) | 0.613 | 5 (24) | 25 (9) | 0.048 |
| OSAS, n (%) | 5 (2) | 0 (0) | 5 (2) | 0.999 | 0 (0) | 6 (2) | 0.999 |
| ILD during index hospitalization, n (%) | 5 (2) | 0 (0) | 5 (2) | 0.999 | 1 (5) | 5 (2) | 0.359 |
| CKD, n (%) | 32 (11) | 3 (21) | 29 (10) | 0.183 | 8 (38) | 31 (11) | 0.002 |
| History of cancer, n (%) | 43 (14) | 6 (43) | 37 (13) | 0.183 | 5 (24) | 38 (14) | 0.205 |
| Chronic liver disease, n (%) | 7 (2) | 1 (7) | 6 (2) | 0.290 | 1 (5) | 9 (3) | 0.527 |
| Autoimmune disease, n (%) | 11 (4) | 0 (0) | 11 (4) | 0.999 | 1 (5) | 13 (5) | 0.999 |
| Pevious organ transplant, n (%) | 4 (1) | 0 (0) | 4 (1) | 0.999 | 0 (0) | 5 (2) | 0.999 |
| Cognitive impairment, n (%) | 29 (10) | 3 (21) | 26 (9) | 0.147 | 2 (10) | 33 (12) | 0.999 |
| Signs upon admission for COVID-19 | |||||||
| Temperature—°C, mean ± SD | 37.5 ± 1.1 | 37.2 ± 1.2 | 37.5 ± 1.1 | 0.301 | 37.0 ± 1.0 | 37.5 ± 1.0 | 0.037 |
| Systolic blood pressure—mmHg, mean ± SD | 127 ± 20 | 129 ± 26 | 127 ± 20 | 0.730 | 129 ± 29 | 127 ± 19 | 0.517 |
| Diastolic blood pressure—mmHg, mean ± SD | 74 ± 11 | 74 ± 9 | 74 ± 12 | 0.928 | 72 ± 13 | 73 ± 12 | 0.720 |
| Heart Rate—bpm, mean ± SD | 85 ± 16 | 83 ± 21 | 86 ± 16 | 0.466 | 81 ± 17 | 87 ± 16 | 0.133 |
| Respiratory rate—bpm, mean ± SD | 20 ± 5 | 19 ± 3 | 21 ± 5 | 0.241 | 21 ± 4 | 20 ± 5 | 0.862 |
| Oxygen saturation—%, mean ± SD | 95 ± 4 | 94 ± 4 | 95 ± 4 | 0.526 | 93 ± 6 | 92 ± 6 | 0.644 |
| Laboratory data upon admission for COVID-19 | |||||||
| WBC—n/mm3, mean ± SD | 7091 ± 3371 | 7723 ± 3772 | 7057 ± 3353 | 0.489 | 7320 ± 2592 | 7118 ± 3455 | 0.799 |
| Neutrophil—%, mean ± SD | 70 ± 12 | 72 ± 11 | 70 ± 12 | 0.620 | 69 ± 12 | 71 ± 11 | 0.544 |
| Lymphocites—%, mean ± SD | 21 ± 10 | 17 ± 11 | 21 ± 9 | 0.205 | 19 ± 9 | 20 ± 10 | 0.638 |
| NLR, mean ± SD | 4.5 ± 5.6 | 10.7 ± 18.9 | 4.1 ± 3.6 | <0.001 | 7.8 ± 16 | 4 ± 4 | 0.017 |
| Hemoglobin—g/dL, mean ± SD | 13.4 ± 1.7 | 13.0 ± 1.0 | 13.4 ± 1.7 | 0.490 | 13 ± 2 | 13 ± 2 | 0.162 |
| Platelets—n/mm3, mean ± SD | 211 ± 76 | 213 ± 79 | 211 ± 77 | 0.888 | 219 ± 72 | 212 ± 79 | 0.695 |
| CRP—mg/L, mean ± SD | 21 ± 42 | 21 ± 33 | 21 ± 42 | 0.972 | 28 ± 39 | 23 ± 45 | 0.657 |
| Creatinine—mg/dL, mean ± SD | 0.9 ± 0.6 | 1.0 ± 0.4 | 0.9 ± 0.6 | 0.588 | 1.4 ± 2.2 | 1 ± 0.7 | 0.056 |
| eGFR—mL/min, mean ± SD | 81 ± 28 | 58 ± 24 | 82 ± 27 | 0.025 | 67 ± 27 | 80 ± 29 | 0.059 |
| ABG upon admission for COVID-19 | |||||||
| pH, mean ± SD | 7.45 ± 0.06 | 7.46 ± 0.047 | 7.46 ± 0.06 | 0.663 | 7.44 ± 0.07 | 7.40 ± 0.64 | 0.754 |
| PaCO2—mmHg, mean ± SD | 35 ± 6 | 35 ± 4 | 35 ± 7 | 0.920 | 38 ± 13 | 35 ± 7 | 0.045 |
| PaO2—mmHg, mean ± SD | 68 ± 19 | 66 ± 17 | 68 ± 19 | 0.812 | 72 ± 19 | 67 ± 18 | 0.271 |
| HCO3—mEq/L, mean ± SD | 25 ± 4 | 26 ± 4 | 25 ± 4 | 0.945 | 27 ± 8 | 25 ± 4 | 0.137 |
| SaO2—%, mean ± SD | 91 ± 11 | 92 ± 7 | 91 ± 11 | 0.960 | 93 ± 6 | 91 ± 11 | 0.575 |
| Lactate—mmol/L, mean ± SD | 1.2 ± 0.9 | 1.2 ± 0.5 | 1.2 ± 0.9 | 0.918 | 1.5 ± 1.1 | 1.2 ± 0.9 | 0.189 |
| PaO2/FiO2 ratio, mean ± SD | 299 ± 82 | 300 ± 62 | 299 ± 83 | 0.975 | 332 ± 92 | 294 ± 83 | 0.050 |
| ECG upon admission for COVID-19 | |||||||
| QRS duration—ms, mean ± SD | 25 ± 22 | 118 ± 45 | 94 ± 20 | <0.001 | 97 ± 20 | 95 ± 20 | 0.648 |
| QTc interval—ms, mean ± SD | 436 ± 32 | 443 ± 51 | 436 ± 32 | 0.409 | 445 ± 27 | 436 ± 32 | 0.214 |
| LBBB, n (%) | 18 (6) | 4 (28) | 14 (5) | 0.007 | 2 (10) | 17 (6) | 0.634 |
| RBBB, n (%) | 15 (5) | 0 (0) | 15 (5) | 0.999 | 1 (5) | 14 (5) | 0.999 |
| Therapy | |||||||
| Beta-blockers, n (%) | 82 (28) | 10 (71) | 72 (26) | <0.001 | 10 (48) | 69 (25) | 0.038 |
| CCBs, n (%) | 59 (20) | 2 (14) | 57 (20) | 0.744 | 5 (24) | 53 (19) | 0.575 |
| Oral diuretic drugs, n (%) | 68 (23) | 7 (50) | 61 (22) | 0.008 | 9 (43) | 56 (20) | 0.026 |
| Intravenous diuretic drugs, n (%) | 24 (8) | 4 (29) | 20 (7) | 0.019 | 3 (14) | 19 (2) | 0.197 |
| Nitrates, n (%) | 9 (3) | 2 (14) | 7 (2) | 0.062 | 0 (0) | 6 (2) | 0.999 |
| Anti-arrhythmics, n (%) | 17 (6) | 1 (7) | 16 (6) | 0.571 | 0 (0) | 9 (3) | 0.999 |
| ASA, n (%) | 51 (17) | 2 (14) | 49 (17) | 0.999 | 4 (19) | 51 (18) | 0.999 |
| P2Y12 inhibitors, n (%) | 9 (3) | 0 (0) | 9 (3) | 0.999 | 1 (5) | 12 (4) | 0.999 |
| OAC, n (%) | 17 (6) | 3 (21) | 14 (5) | 0.039 | 7 (33) | 15 (6) | <0.001 |
| ACE-inhibitors, n (%) | 43 (15) | 2 (14) | 41 (15) | 0.999 | 2 (10) | 48 (17) | 0.546 |
| ARBs, n (%) | 22 (7) | 1 (7) | 21 (7) | 0.999 | 1 (5) | 31 (11) | 0.712 |
| Insulin, n (%) | 36 (12) | 1 (7) | 35 (12) | 0.999 | 3 (14) | 11 (4) | 0.067 |
| Statins, n (%) | 24 (8) | 0 (0) | 24 (9) | 0.613 | 3 (14) | 46 (17) | 0.999 |
| Oral antidiabetic drugs, n (%) | 8 (3) | 0 (0) | 8 (3) | 0.999 | 1 (5) | 24 (9) | 0.999 |
| QTc modifying drugs, n (%) | 166 (56) | 10 (71) | 156 (55) | 0.280 | 1 (5) | 40 (15) | 0.328 |
| Hydroxycloroquine, n (%) | 240 (81) | 9 (64) | 231 (82) | 0.152 | 14 (67) | 223 (81) | 0.151 |
| Lopinavir, n (%) | 47 (16) | 1 (7) | 46 (16) | 0.705 | 3 (14) | 43 (14) | 0.999 |
| Remdesivir, n (%) | 4 (1) | 0 (0) | 4 (1) | 0.999 | 0 (0) | 4 (1) | 0.999 |
| Darunavir, n (%) | 115 (39) | 4 (29) | 111 (39) | 0.576 | 5 (24) | 109 (40) | 0.170 |
| Tocilizumab, n (%) | 8 (3) | 0 (0) | 8 (3) | 0.999 | 0 (0) | 8 (3) | 0.999 |
| LMWH, n (%) | 202 (68) | 9 (64) | 193 (68) | 0.772 | 17 (81) | 182 (66) | 0.228 |
| Azithromycine, n (%) | 64 (22) | 3 (21) | 61 (22) | 0.999 | 3 (14) | 61 (22) | 0.583 |
| Steroids, n (%) | 46 (16) | 0 (0) | 46 (16) | 0.137 | 4 (19) | 42 (15) | 0.548 |
| In-hospital events | |||||||
| Acute heart failure, n (%) | 20 (7) | 4 (29) | 16 (6) | 0.001 | 4 (19) | 20 (7) | 0.078 |
| ALI, n (%) | 103 (35) | 3 (21) | 100 (35) | 0.393 | 11 (52) | 101 (37) | 0.167 |
| ARDS, n (%) | 50 (17) | 1 (7) | 49 (17) | 0.477 | 3 (14) | 53 (219) | 0.774 |
| AKI, n (%) | 13 (4) | 1 (7) | 12 (4) | 0.474 | 0 (0) | 20 (7) | 0.379 |
| CRRT, n (%) | 6 (2) | 0 (0) | 6 (2) | 0.999 | 1 (5) | 11 (4) | 0.593 |
| Secondary infection, n (%) | 35 (12) | 2 (14) | 33 (12) | 0.674 | 2 (10) | 42 (15) | 0.750 |
| Septic shock, n (%) | 1 (0) | 0 (0) | 1 (0) | 0.999 | 1 (5) | 3 (1) | 0.256 |
| Any thrombotic complication, n (%) | 13 (4) | 1 (7) | 12 (4) | 0.474 | 2 (10) | 14 (5) | 0.316 |
| ACS, n (%) | 2 (1) | 0 (0) | 2 (1) | 0.999 | 0 (0) | 5 (2) | 0.999 |
| Pulmonary embolism, n (%) | 8 (3) | 0 (0) | 8 (3) | 0.999 | 1 (5) | 7 (3) | 0.449 |
| Deep venous thrombosis, n (%) | 4 (1) | 0 (0) | 4 (1) | 0.999 | 2 (10) | 3 (1) | 0.042 |
| Ischemic stroke, n (%) | 1 (0) | 1 (7) | 0 (0) | 0.047 | 0 (0) | 1 (0.4) | 0.999 |
| Bilateral CT involvment, n (%) | 168 (57) | 6 (43) | 162 (57) | 0.408 | 12 (57) | 167 (61) | 0.818 |
| ICU admission, n (%) | 24 (8) | 1 (7) | 23 (8) | 0.999 | 0 (0) | 23 (8) | 0.388 |
| In-hospital LOS—days, mean ± SD | 14 ± 10 | 13 ± 9 | 14 ± 10 | 0.612 | 16 ± 9 | 13 ± 10 | 0.355 |
| Outcome | Number of Events | Crude Event Rate (%) | 95% CI |
|---|---|---|---|
| All-cause death | 14 | 4.730 | 2.252–7.207 |
| MACCE | 21 | 7.095 | 4.060–10.129 |
| Cardiovascular death | 6 | 2.027 | 0.405–3.649 |
| Myocardial infarction | 2 | 0.676 | 0.000–1.612 |
| Stroke | 4 | 1.351 | 0.027–2.676 |
| Pulmonary embolism | 1 | 0.338 | 0.000–1.000 |
| Acute heart failure | 6 | 2.027 | 0.405–3.649 |
| Hospitalization for cardiovascular causes | 14 | 4.730 | 2.252–7.207 |
| All-Cause Death | ||||||||
|---|---|---|---|---|---|---|---|---|
| Covariate | Univariate | Multivariate | ||||||
| HR | 95% CI | Z-Score | p Value | HR | 95% CI | Z-Score | p Value | |
| Age | 1.083 | 1.03–1.139 | 3.106 | 0.002 | 1.083 | 1.008–1.165 | 2.163 | 0.031 |
| Female sex | 1.507 | 0.475–4.781 | 0.696 | 0.487 | 1.683 | 0.393–7.198 | 0.702 | 0.483 |
| In-hospital acute heart failure | 5.414 | 1.399–20.948 | 2.447 | 0.014 | 2.003 | 0.437–9.193 | 0.894 | 0.371 |
| QRS duration | 1.031 | 1.011–1.052 | 3.031 | 0.002 | 1.015 | 0.999–1.042 | 1.183 | 0.237 |
| In-hospital beta-blockers use | 8.489 | 2.174–33.152 | 3.077 | 0.002 | 1.887 | 0.397–8.97 | 0.799 | 0.424 |
| MACCE | ||||||||
| Covariate | Univariate | Multivariate | ||||||
| HR | 95% CI | Z-Score | p Value | HR | 95% CI | Z-Score | pValue | |
| Age | 1.049 | 1.016–1.082 | 2.985 | 0.003 | 1.026 | 0.99–1.064 | 1.425 | 0.154 |
| Female sex | 2.029 | 0.9–4.571 | 1.707 | 0.088 | 2.612 | 1.047–6.518 | 2.058 | 0.040 |
| In-hospital acute heart failure | 4.39 | 1.604–12.012 | 2.88 | 0.004 | 3.454 | 1.193–9.999 | 2.286 | 0.022 |
| AF | 6.077 | 2.555–14.452 | 4.082 | <0.001 | 3.049 | 1.128–8.24 | 2.198 | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renda, G.; Ricci, F.; Spinoni, E.G.; Grisafi, L.; D’Ardes, D.; Mennuni, M.; Tana, C.; Rognoni, A.; Bellan, M.; Sainaghi, P.P.; et al. Predictors of Mortality and Cardiovascular Outcome at 6 Months after Hospitalization for COVID-19. J. Clin. Med. 2022, 11, 729. https://doi.org/10.3390/jcm11030729
Renda G, Ricci F, Spinoni EG, Grisafi L, D’Ardes D, Mennuni M, Tana C, Rognoni A, Bellan M, Sainaghi PP, et al. Predictors of Mortality and Cardiovascular Outcome at 6 Months after Hospitalization for COVID-19. Journal of Clinical Medicine. 2022; 11(3):729. https://doi.org/10.3390/jcm11030729
Chicago/Turabian StyleRenda, Giulia, Fabrizio Ricci, Enrico Guido Spinoni, Leonardo Grisafi, Damiano D’Ardes, Marco Mennuni, Claudio Tana, Andrea Rognoni, Mattia Bellan, Pier Paolo Sainaghi, and et al. 2022. "Predictors of Mortality and Cardiovascular Outcome at 6 Months after Hospitalization for COVID-19" Journal of Clinical Medicine 11, no. 3: 729. https://doi.org/10.3390/jcm11030729