1. Introduction
Autism spectrum disorders (ASD) is a group of complex, heterogeneous, neurodevelopmental conditions. The International Statistical Classification of Diseases and Related Health Problems (the 10th revision, ICD-10) list by the World Health Organization (WHO) distinguishes a group of pervasive developmental disorders characterized by qualitative abnormalities in reciprocal social interactions and in patterns of communication and by a restricted, stereotyped, repetitive repertoire of interests and activities. That group includes childhood autism; atypical autism; Rett syndrome, another childhood disintegrative disorder; hyperkinetic disorder with associated mental retardation and stereotyped movements; Asperger’s syndrome, another global development disorder; and comprehensive developmental disorder, unspecified. Common features of all these disorders are problems in communication and understanding of social phenomena [
1].
ASD is characterized by impairment of social behavior, social interactions, communication, learning, and the presence of restricted and repetitive patterns of behavior and activities [
2,
3]. ASD affects more children than cancer, diabetes, and AIDS combined, which makes it the fastest-growing neurodevelopmental disability, with a higher prevalence among males than females [
4,
5]. According to literature data, the prevalence of ASD in the world is about 1 percent of the entire population of individual countries. For 2017, the prevalence was, respectively, 0.74% for the United States, 0.94% for Canada, 0.64% for Germany and Australia, and 0.47% for Poland. Detailed analyses based on the DALY (Disability Adjusted Years of Life) for ASD measured per 100,000 people showed that this rate is highest for Canada at 129.54 and then the United States at 101.57, while for European countries, it ranges from limits 93–62 DALY’s per 100,000 people. The DALY index is used to measure the overall burden of disease (both years lost and years lived with disability), and 1 DALY is understood as one healthy life year lost [
6]. Based on the data from the Centers for Disease Control and Prevention (CDC), the prevalence of ASD increases year by year: at the beginning of 2000, it was 1 in 150 people over eight years, while in 2016, it was 1 in 54 people [
7]. Similar trends are observed in many European countries, including Poland, while in the years 2010–2019, the percentage of disabled children diagnosed with ASD was 20.87%, and detailed data on age showed that the largest percentage was constituted by school children and adolescents 8–16 years old (46.09%) (
Figure 1) [
8]. Because ASD is a lifelong condition, the management of ASD is associated with huge health-economic costs [
5,
9] The lifetime social cost for an individual with an ASD in the U.S. was estimated at
$3.6 million. For all of the individuals with ASD identified in the three decades from 1990–2019, the lifetime social cost for the U.S. is estimated to be more than
$7 trillion in 2019 dollars [
10].
Apart from being heterogeneous in nature, ASD is believed to be multifactorial in origin. However, the pathogenesis of ASD remains poorly understood, and there is no consensus among investigators regarding the exact etiology. It is suggested that genetic, biological, and environmental factors altogether contribute to the development of ASD. ASD is known to be highly heritable (~90%), and some related genes have been reported [
11,
12,
13]. Despite that, a genetic component cannot fully explain ASD as a single gene, and chromosomal defects only account for a minority of ASD cases (10–20%) [
14,
15]. More and more studies raise the importance of environmental factors in the development of ASD. This applies to contamination and/or exposure of the developing organism to many metals, such as lead, aluminum, or cadmium, as well as to disturbances in the homeostasis of microelements, such as manganese or zinc, the presence of which is necessary for the proper functioning of the organism [
16]. Manganese is one of the most common metals found on Earth and thus is a source of metal used in many industrial products, including leather, textile, battery production, glass, as well as cosmetics, paints, and fertilizers. This means that it is present in almost every sphere of human life, constituting not only a micronutrient necessary for proper functioning but also a potential source of danger. Estimated literature data indicate that the content of Mn in soils in the United States varies from 40 to 900 mg/kg, which directly affects its presence in plants (500 µg/g is toxic to plants) as well as in the meat of farm animals that we eat. There are several ways for Mn to enter the human body, including alimentary (diet, water, food), inhalation (air), or skin contact [
17,
18,
19]. Although an exposure to excess levels of manganese has many negative effects, including neurological disorders (tremors, difficulty walking, muscle and facial spasms), impaired cognitive effects (problems with concentration, memory, decreased scientific performance), and neurobehavioral disorders (hyperactivity, increased behavior opposition), it should not be fully eradicated from the diet, as it also has many health-promoting functions [
16,
17,
20]. Such functions include the protection of brain cells against oxidative stress or the influence on the release of neurotransmitters. It should also be mentioned that Mn deficiency in the body can lead to growth impairment, poor bone formation, and skeletal defects as well as reduced fertility, birth defects in children, and metabolic changes (impaired glucose tolerance, reduced lipid and carbohydrate metabolism) [
16,
17,
18,
19,
20]. The homeostasis of Mn ions in the body is maintained and regulated by a number of mechanisms of uptake, storage, and release by individual cells. About 3–5% of ingested Mn is absorbed from the gastrointestinal tract. It is thought that under homeostatic conditions, Mn enters the portal circulation through either passive diffusion or active transport involving divalent metal transporter 1 (DMT1). Mn is distributed throughout the body, including bones, kidneys, pancreas, liver, and brain, which accumulate the highest contents of Mn [
21].
Inhaled Mn is very often transported directly to the brain before it is metabolized by the liver. This is clearly visible in the MRI pictures, where the excess of this element is accumulated in the CNS in basal ganglia, which in humans plays important functions in the processes of body movement control, cognitive processes, emotional control, and learning [
18,
19].
In addition to Mn, the second most significant metal influencing the functioning of the human body is cadmium, belonging to mutagenic and teratogenic elements. Like other heavy metals, Cd is present in the environment as a result of many anthropogenic activities, including use in industry as a corrosive reagent, as a PVC stabilizer, in batteries, in accumulators, from smelting and refining copper and nickel, from burning fossil fuels, and even from the use of fertilizers phosphate. Due to the ubiquitous presence of this metal in the environment, there are three ways for Cd to enter the body: mainly through the respiratory tract, through the gastrointestinal tract, and less often through the skin [
22]. Upon entering the body, Cd is transported by erythrocytes and albumin and accumulates in the kidneys, liver, and intestines. The presence of this element in the body causes a number of adverse health effects, such as kidney and adrenal dysfunction, liver disorders, pulmonary edema, damage to the genital organs, and disorders of the hematopoietic system. Cd is also a common carcinogen involved in the development of breast, lung, prostate, bladder, nasopharyngeal, and pancreatic cancers [
22,
23].
Thyroid hormones are essential for the proper functioning of the human body due to the maintenance of balance in almost all metabolic processes. Triiodothyronine (T3) and thyroxine (T4) in the early stages of development ensure normal growth as well as the functioning of the nervous and cardiovascular systems. Their level varies depending on many factors, e.g., in elderly people, it drops from 10 to 50% compared to children, but their impact on many metabolic processes and circulation, functioning of the digestive tract, muscles, nerves, and mental functions remains unchanged [
24]. The thyroid-stimulating hormone (TSH) produced by the pituitary gland in order to stimulate the secretion of T3 and T4 by the thyroid gland is also involved in the proper functioning of the thyroid gland. The thyroid gland is often exposed to many endocrine toxic elements, such as cadmium or manganese, causing disorders of proper functioning [
18]. Mn ions can directly and indirectly interfere with the binding, transport, and activity of thyroid hormones at the tissue level. The first pathway concerns the dysfunction of deiodinase enzymes (which are responsible for the activation and deactivation of thyroid hormones) involved in the metabolic, signaling, and regulatory processes of the formation and conversion of thyroid hormones, whereas the second pathway concerns the binding of Mn ions to dopaminergic receptors. Dopamine exerts a suppressive effect on TSH secretion and thereby affects the level of thyroid hormones (damage to dopaminergic receptors may cause non-developmental deficits) [
18,
19].
In the case of Cd, literature data indicate structural and functional damage to the follicle and the endocrine apparatus of the thyroid gland. This is indicated by histological changes (flattening of follicular cells, growth of interstitial fibrous tissue between the follicles) and metabolic changes in the functioning of the thyroid gland. A positive correlation has also been demonstrated between the concentration of Cd in the blood and its accumulation in the thyroid gland. It was reported that the thyroid gland of people exposed to cadmium accumulates three times more cadmium compared to that of unexposed people [
25]. Studies in an animal model have shown that Cd reduces the secretory granules of thyroglobulin in the cytoplasm, which also causes a decrease in serum T3 and T4 levels [
22,
23,
26].
It has been shown that thyroid dysfunction is associated with neurological and psychiatric disorders, including neurodevelopmental disorders, such as ASD [
27,
28,
29,
30,
31,
32]. However, the exact relationship is far from being fully understood. It has been shown that a family history of autoimmune thyroid disease was associated with ASD with developmental regression [
33], and it was suggested that maternal hypothyroidism is associated with ASD in children [
34]. Another study showed no differences between thyroid hormone levels measured in children already diagnosed with ASD compared with typically developing controls [
35]. One study found that very low thyroxine (T4) levels (3rd percentile) in children were associated with higher ASD risk [
31], while the other study found no association between neonatal T4 levels and ASD or any other neurological condition [
36]. Furthermore, several toxic metals, including arsenic (As), lead (Pb), aluminum (Al), cadmium (Cd), and mercury (Hg), which are widely present in the environment, have been classified as neurotoxins [
37,
38,
39]. Yasuda et al. [
40] indicated that Cd highly accumulates in infants and children. Later, the same authors demonstrated high burdens of Cd in infantile patients diagnosed with autism [
41].
Rossignol et al. [
42] reported in a meta-analysis on toxicants and ASD that almost three-quarters of research found significant differences between neurotypical individuals and individuals with ASD. On the other hand, some studies revealed that children with ASD are characterized by lower values of toxic elements (e.g., As and Pb) in hair [
43].
Both effects of thyroid dysfunction [
32,
44] and exposure to toxic metals [
45] in ASD have already been discussed in literature. Our study aimed to assess the relationship between the level of hormones influencing the proper functioning of the thyroid in the serum: thyroid-stimulating hormone (TSH), free triiodothyronine (fT3), free thyroxine (fT4), and the concentration of cadmium (U-Cd) and manganese (U-Mn)) in urine of patients with ASD. We hoped that our research results would allow us to enrich the literature data and allow us to shed new light on the process of ASD pathogenesis in adolescents.
In the light of the existing inconsistencies regarding study designs and findings, and the lack of precisely known mechanisms underlying the effects of heavy metals as endocrine disruptors conducting this type of research is justified.
4. Discussion
Heavy metals in the environment can have a significant impact on the health and development of the human body. Prenatal exposure to toxic metals or changes in maternal essential elements during pregnancy may be a risk factor for neurodevelopmental disorders, such as attention deficit hyperactivity disorder (ADHD) and ASD, in offspring [
57,
58,
59,
60,
61,
62]. In studies by Skogheim et al. [
63], it was checked whether maternal levels of toxic metals and essential elements measured at mid-pregnancy, both individually and as mixtures, were associated with the diagnosis of ADHD or ASD in childhood. The results obtained by the researchers indicate that there is a positive correlation between the levels of metals and toxic elements during pregnancy and the prevalence of ASD and ADHD in children. The most important were arsenic, cadmium, copper, mercury, manganese, magnesium, and lead. Researchers suggest that the levels of these elements may have a negative effect on the development of the nervous system [
58,
59]. However, throughout his or her life, a person is exposed to contamination and accumulation of heavy metals in the body due to anthropogenic human activity and the presence of these elements in almost every sphere of life. It has been suggested that children with autistic spectrum may have poor heavy-metal-detoxifying mechanisms [
59].
Research in recent years has shown that dysregulation of micronutrient homeostasis and increased body contamination with heavy metals, such as lead or mercury, can significantly affect the development of ASD. Therefore, scientists are increasingly eager to focus on researching new elements that may be involved in the development of these diseases, and manganese and cadmium are of particular importance. These metals show higher toxicity in children than in adults, which affects the developing body and may predispose to increased incidence of certain diseases. Due to the ubiquitous presence of manganese in human life and its pro-health aspects, which we mentioned earlier, in the literature, one can find numerous studies measuring its level in various body fluids, such as blood (in the range of 4–15 µg/L), red blood cells, serum (in the range 0.4–0.85 µg/L), urine (in the range 1–8 µg/L), tooth enamel, and hair, in both healthy and ASD children [
60].
In literature data regarding excretion of the studied elements, both Cd and Mn may be considered as contradictory. Several studies reported higher urinary excretion levels of Cd in healthy children than in ASD group [
58,
59]. On the other hand, according to Akyuzlu et al., of findings U-Cd were higher in individuals with ASD [
61], which is consistent with our results. The opposite results were achieved for U-Mn, which was lower in cited studies and higher in those with ASD in comparison with the healthy group. This is may be due not only to methodological differences or different research material but also to etiological or geographical differences. Each region of the world will be characterized by completely different contamination of soil, air, or water with these elements, which in turn will also translate into a variable diet in these people (cultural diversity and availability of certain foods and their amount and degree of contamination). In addition, the excretion of some metals varies with age and gender (see
Table 1).
At the core of Mn-induced neurotoxicity is the inactivation of the mitochondria, resulting in an increase in reactive oxygen species in brain regions affected by contamination and oxidative stress induction. The exact molecular mechanisms influencing the homeostasis of Mn ions in the human body still remain in the area of intense research. Currently, several transporters responsible for this process are known, including ferroportin, ZIP8/14, glutamate receptor, manganese citrate transporter, DMT1, and CA2 + channels as well as SCL3A10 and SCL39A14, which have a direct impact on the control of manganese levels in the blood, manifesting from not only the presence of these transporters but also the effect on maintaining homeostasis. One should also take into account genetic differences, including the phenomenon of polymorphism, which will condition the proper functioning of these structures [
19,
64].
In addition, many scientific studies argue that the pathomechanism of diseases caused by manganese contamination in humans is closely correlated with the functioning of the thyroid gland. SCL3A10 and SCL39A14 transporters are responsible for the uptake and release of manganese ions in the body, the mutations of which result in the loss of their functions, which in turn translates into hereditary toxicity of manganese. It manifests itself not only in increased levels of manganese in the blood and brain but also in the thyroid gland and liver, which contributes to the development of neurotoxicity. Studies by Liu and colleagues have shown that the transport activities of these proteins are essential for the proper excretion of manganese by the liver [
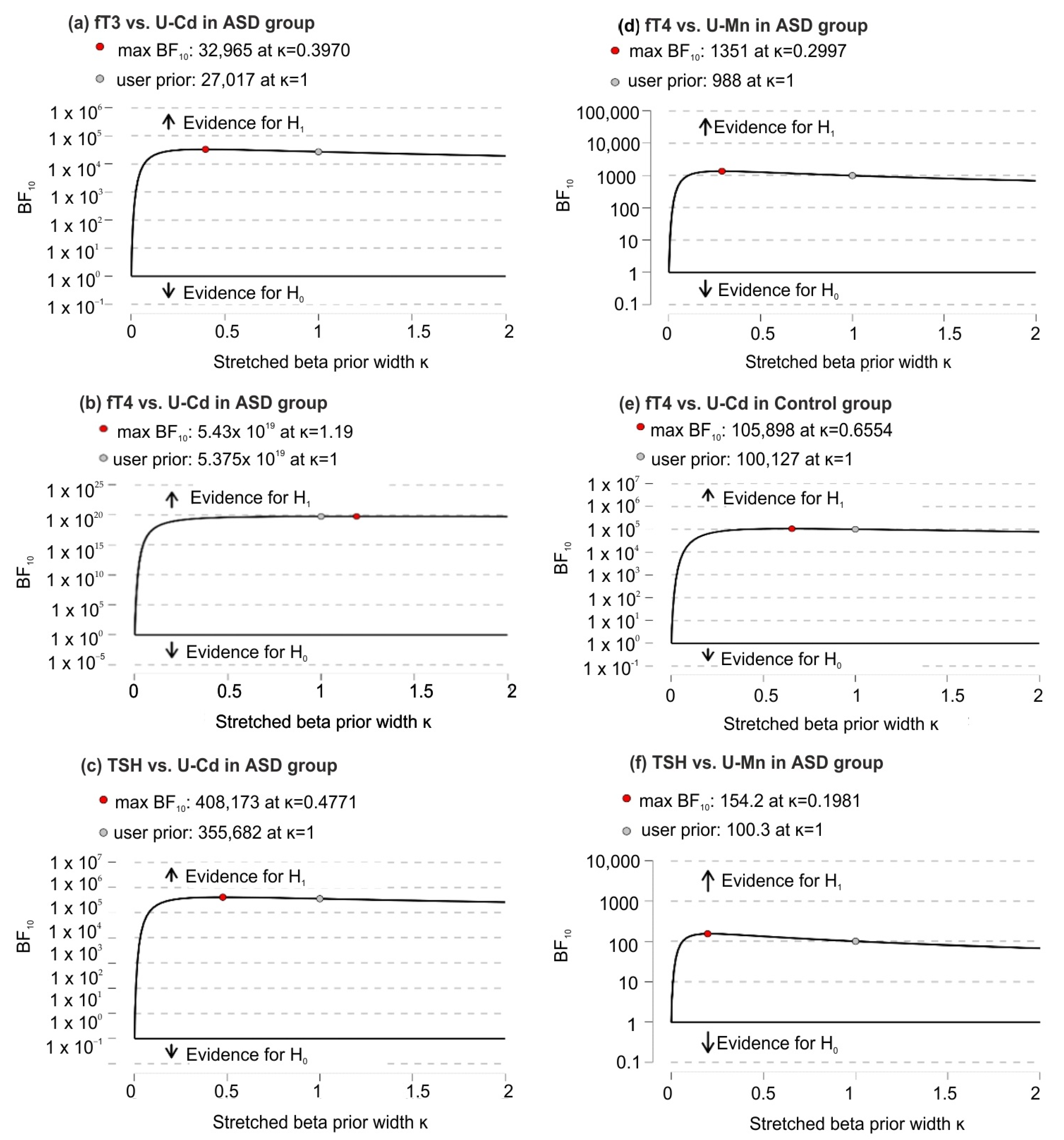
64]. Changes in SLC3A10 resulted in increased amounts of manganese in the thyroid compared to the SLC39A14 knock-out and knock-out of both transporters, which showed lower levels of manganese and normal thyroid activity. In addition, it was shown that intrathyroid levels of thyroxine with a single SLC30A10 knockout were higher than in the control group, meaning that the hypothyroid phenotype induced by these changes is induced by high levels of manganese in the thyroid, which blocks the production of thyroxine. In our studies, we showed that there is a negative correlation between U-Mn and serum fT4 levels among ASD patients, which was not found in the control group [
19]. Accumulation of manganese in patients with specific ASD features as measured by the Autism Diagnostic Observation Schedule (ADOS) was the subject of a study by Fiore et al. [
65]. They showed that the level of manganese in the hair was inversely correlated with the cognitive level (full IQ) of people with ASD. These studies confirm the significant influence of manganese in neuronal development. Additionally, another study related to the analysis of primary incisors in children six to nine years of age showed significant differences in the concentration of metals in the tooth samples of children with ASD and typically developing children. The content of manganese was three times higher in the teeth of children with ASD compared to children from the control group [
66]. In the light of the above varied data obtained in studies by various teams and taking into account the potential environmental differences related to exposure to heavy metals, it is difficult to indicate the unequivocal effect of manganese on human health. Moreover, reference values for Mn of the 24-h urine measurement have not been established for patients <18 years of age.
As regards the second analyzed element, which was cadmium (Cd), we also observed significant correlations that may affect the development of ASD in adolescents. Cadmium alone has multiple effects on cells; therefore, it can directly or indirectly interfere with the development of the brain. It disrupts the progress of the cell cycle, proliferation, differentiation, and the induction of apoptosis. The excess of this heavy metal (as much as 50% of cadmium absorbed by the body) accumulates in the liver and kidneys, where its half-life in the body is 6–38 years and 4–19 years, respectively [
17]. It has also been shown that this element can accumulate in bones and the entire skeletal system as well as in the brain, as is the case with zebrafish [
67]. The problem of the influence of cadmium on the human body is still a subject of intense research by many scientists. Similar to the data on manganese concentrations in the human body, the concentration of Cd among ASD patients reported in the literature is also extremely varied, and the reference values for Cd of the 24-h urine measurement have not been established for patients <18 years of age as well. The largest amount of data concerns the presence of this element in the hair, which, depending on the researcher, is 0.021 µg/g [
68], 0.0277 µg/g [
43], or even 0.62 mg/kg [
58].
In the case of autism-related research, the hypothesis we adopted was the effect of metals on thyroid function. Indications that Cd may affect thyroid function were found by the team of Chen et al. [
68], who analyzed National Health and Nutrition Examination Survey (NHANES) data for 2007–2008 obtained from the general U.S. population with higher levels of environmental exposure. Analyses showed that higher levels of thyroid hormones and thyroglobulin (Tg) in adults correlated with increased levels of urinary Cd, i.e., greater exposure to Cd. However, in terms of TSH level itself, it was no longer associated with exposure to Cd. Consequently, this raises questions about the effects of this metal on the thyroid gland [
69]. Another analysis of NHANES data from 2007–2008 confirmed that urinary Cd levels also correlated with increased T3 and T4 levels. In addition, studies have shown elevated blood Cd levels were associated with decreased TSH levels, suggesting that this inverse relationship between Cd and TSH is indicative of overt thyroid disease caused by exposure to Cd. Another aspect of the observation was that the presence of blood Cd correlated with lower TSH levels and unchanged levels of T3 and T4, indicating the presence of subclinical primary hyperthyroidism in this case. On the other hand, urinary Cd levels are associated with higher T3 and T4 levels, but TSH levels remained unchanged, indicating secondary hyperthyroidism. Additionally, the data obtained from NHANES were used to analyze the correlation between the presence of Cd in urine and the concentration of thyroid hormones [
68]. The presence of Cd is different both in human blood and urine and may indicate different levels of contamination in the whole organism. Research suggests that urinary Cd excretion is a function of total body content of Cd, nephron numbers, tubular reabsorption capacity, and the presence of other disease, and other conditions, such as hypertension [
70]. These findings led to the hypothesis that thyroid hormone levels are strongly related to the total body burden on Cd, while the observed changes in TSH levels alone may reflect the relatively recent exposure to this metal. Currently, researchers are trying to consider the effects of interactions between various trace and toxic metals. One publication found positive statistically significant correlations between Cd and fT3 levels and Cd and Tg levels but only for men, indicating gender differences in thyroid function response to Cd exposure. The evidence for a link between Cd and thyroid dysfunction remains inconclusive, and more research is needed to clarify the problem and better understand the effects of Cd on the thyroid gland [
71,
72,
73].
Some studies cited in the introduction suggest that lower production of thyroid hormones at birth may influence neurodevelopmental impairment (subsequently diagnosis of ASD) that persists even though the hormone levels return later to normal ranges (it is worth noting that this is a fairly broad range: TSH from 0.45–5.0 mIU/L under 14 y and from 0.4 to 4.0 mIU/L above 14 y [
52]) [
31]. Frye at al. emphasized the impact of folate receptor autoantibodies, which may contribute to the higher TSH levels in children with autism [
32].
However, all the studies conducted, including ours, did not test the interaction of the environment with the genetic predispositions and conditions of the studied children and adolescents. Therefore, as researchers around the world argue, analyzing and comparing the presented data without taking into account the gene–environment interaction is incomplete and cannot be interpreted as unrelated.
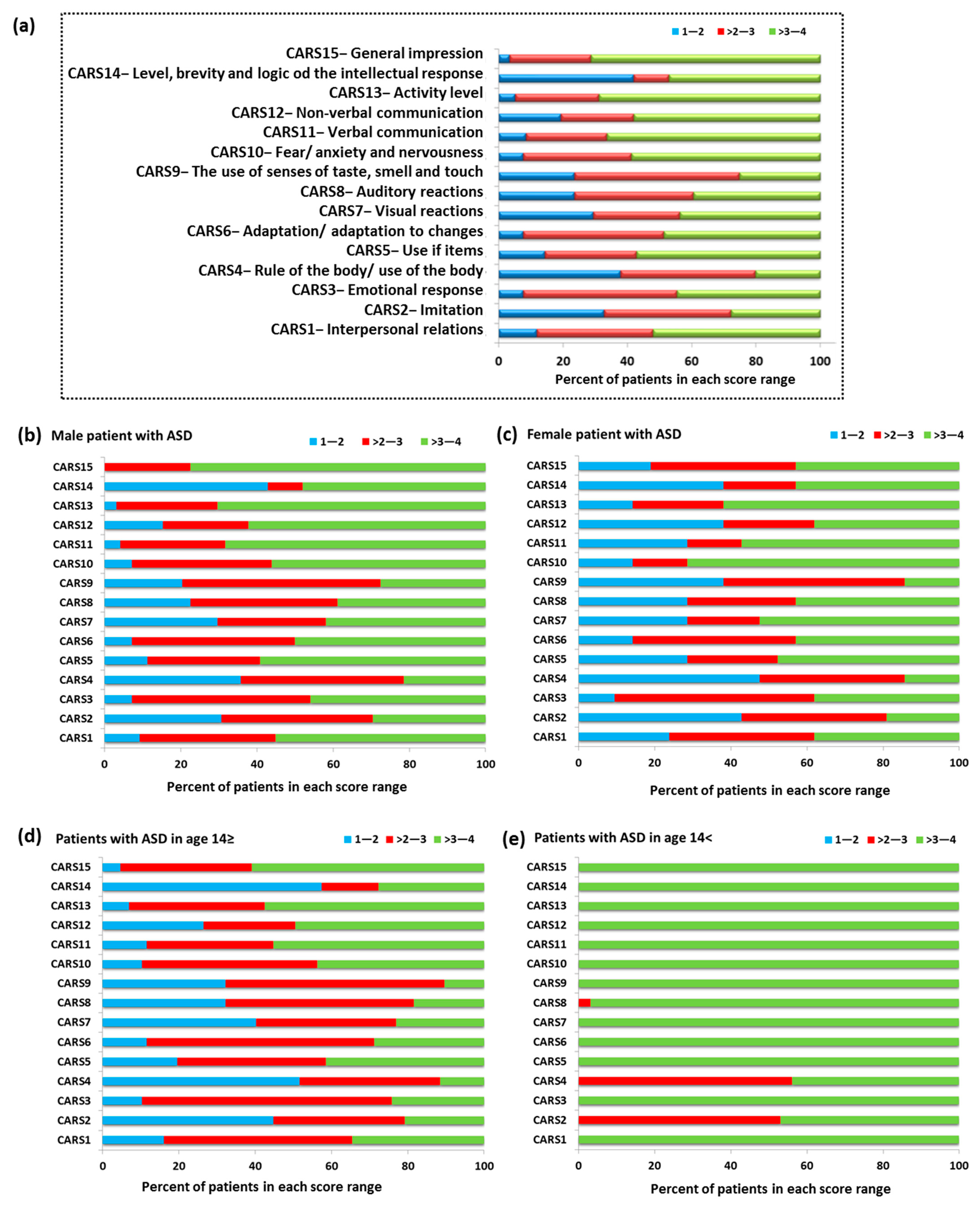
Results of correlation analysis of U-Mn, U-Cd, and biochemical variables with CARS scores in group of patients based on their sex (
Table 7) revealed a link with visual responsiveness. There is growing evidence for disruption of the auditory and visual processing pathways in autism [
74]. Individuals with autism tend to manifest significant disturbances in perception and processing of sensual stimuli from the environment as well as from their own body. Both over- and under-sensitivity is characteristic for the described neurodevelopmental disorder. A marked arousal when exposed to strong visual stimuli is usually observed, and response depends on the type of visual information [
74]. Both autism and visual problems can cause an avoidance of eye contact or problems with visual attention, etc. Hypersensitivity to light and other visual stimuli is a very common problem in ASD.
An example of animal-based research showed interesting effects of cadmium pollution on the vision of adult zebrafish Danio rerio [
75]. The results demonstrated that cadmium impairs functional responses, particularly through an increase in light sensitivity. At this point, however, it is difficult to prove that some kind of a photosensitivity in autistic individuals confirmed by the diagnostic tests is related to cadmium exposure and its effects on retina. In the light of some human studies that determined Cd accumulation in human retinal tissues, specifically the neural retina, retinal pigment epithelium, and choroid [
76], it seems to be justified to conduct studies on cadmium effects in the population with autism. Recently, studies have been undertaken on the effects of other toxic metals on the retina of donors without visual impairment and no significant retinal abnormalities [
77]. It was confirmed that toxic metals accumulate in the retina and may contribute to the pathogenesis of visual disturbances.
If an association between increased cadmium levels in individuals with ASD and its effects on increased photosensitivity could be proven, preventive measures could be taken early in the patients’ lives. Future larger studies should focus on confirming whether Cd is associated with disturbed visual responsiveness in ASD and on the explanation of why this relationship is evident in the older group and not in the younger group (
Table 6). Undoubtedly, our study confirms that elemental homeostasis and toxin exposure affect the severity of specific autistic symptoms.
A strong positive correlation between BMI and cadmium concentration, TSH, and once fT3/fT4 was found in our studies. These correlations show that the higher the BMI value, the higher the concentration of U-Cd and the concentration of thyroid hormones (
Table 2). The literature data show a relationship between U-Cd levels and obesity. Studies by Green et al. [
78] indicate that there is a relationship between the presence of cadmium in the blood of pregnant women and an increased risk of adolescent obesity in offspring obesity. Additionally, this trend was tested in an animal model (zebrafish), in which exposure to Cd was also associated with increased obesity [
79]. On the other hand, in the case of the influence of BMI on the thyroid gland, studies were also carried out on women, in which high maternal BMI coincides with the immature histological phenotype, affecting the thyroid gland of female fetuses [
80]. In turn, another study related to the Korean population showed that the risk of an underactive thyroid gland increased gradually with blood cadmium content in men, while no such correlation was observed in the case of women [
76].
Despite the above information, we have not encountered any studies that directly refer to the correlation between the concentration of U-Cd, thyroid hormones, and BMI.
Advantages and Limitations of the Study
A detailed analysis of individual subgroups of patients depending on age and sex allowed for a better and more complete picture of the studied patients and the relationships between the concentration of U-Cd and U-Mn and selected biochemical parameters of thyroid function.
The limitations of the present study refer to the missing information on the intake of micronutrients and, generally, on dietary factors that could affect relationships between both toxic and essential elements. As it is well known, chronic exposure to the toxic metals is particularly dangerous to the body. Since urine testing can only show recent exposure, consideration of other types of samples, such as blood, hair, or fingernails, would add to the knowledge on the discussed subject. However, in our study, the non-invasiveness of sampling was crucial for project participants. It is worth mentioning that hormone tests are usually done prophylactically, and metal analysis is not a routinely ordered test.
Although thyroid hormone levels were examined, and no serious pathology of this gland was found in either group of our study participants, additional imaging studies (e.g., ultrasonography) could bring further information about the location, size, and echostructure of the thyroid gland as well as its vascularity at the time of testing. Another limitation of this study is the inability to relate genetic interactions with the patients’ living environment.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}