
Morphological Relation of Peripheral Nerve Sheath Tumors and Nerve Fascicles: Prospective Study and Classification

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
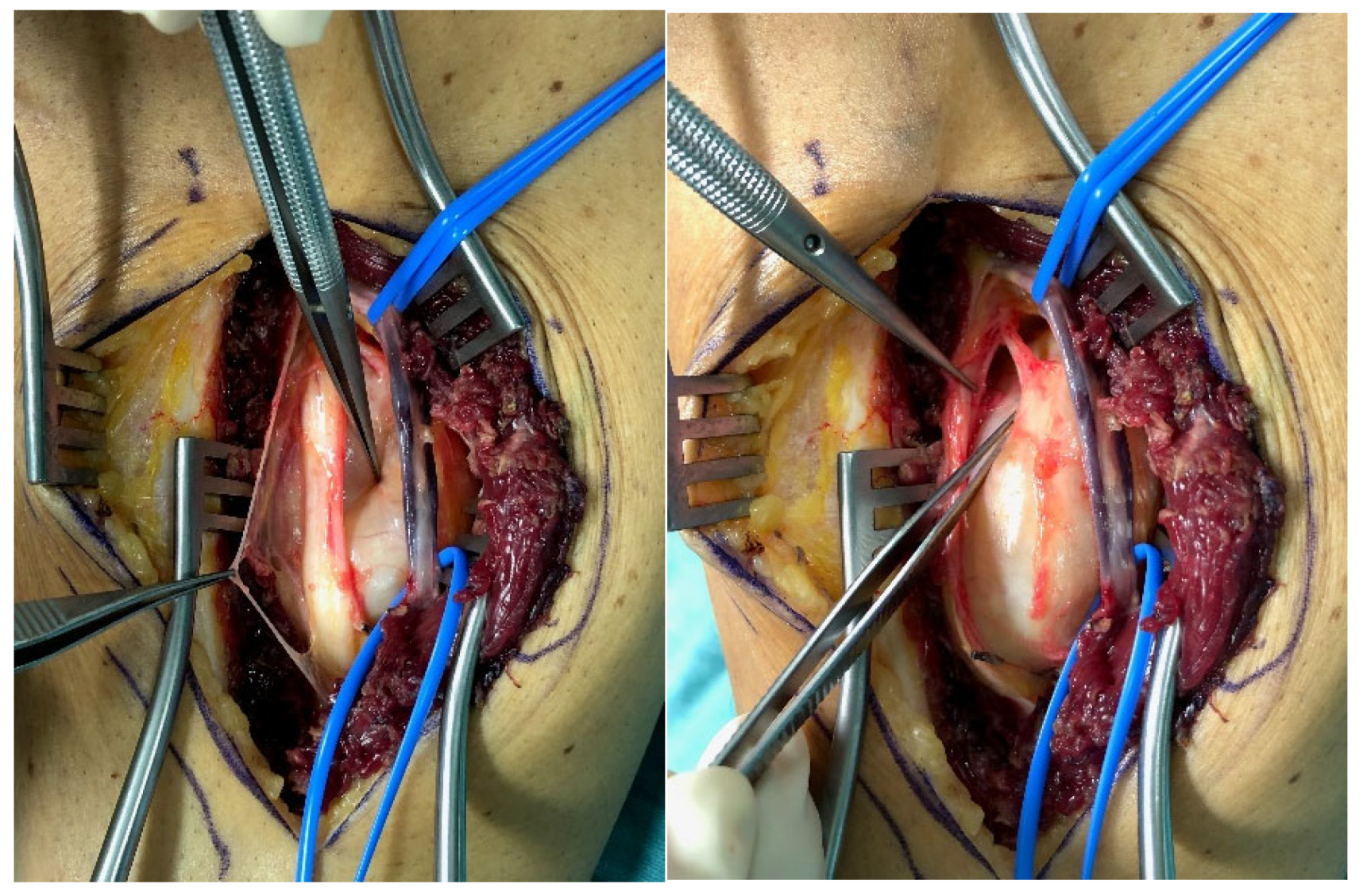
2.1. Surgical Technique
2.2. Assessment
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyer, A.; Billings, S.D. What’s new in nerve sheath tumors. Virchows Arch. 2020, 476, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Levi, A.D.; Ross, A.L.; Cuartas, E.; Qadir, R.; Temple, H.T. The surgical management of symptomatic peripheral nerve sheath tumors. Neurosurgery 2010, 66, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, F.J.; Folpe, A.L.; Giannini, C.; Perry, A. Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathol. 2012, 123, 295–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanouda, S.; Kaya, G. Benign Cutaneous Peripheral Nerve Sheath Tumor with Hybrid Features: Report of Two Cases with Schwannoma/Perineurioma and Schwannoma/Neurofibroma Components. Dermatopathology 2017, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ronellenfitsch, M.W.; Harter, P.N.; Kirchner, M.; Heining, C.; Hutter, B.; Gieldon, L.; Schittenhelm, J.; Schuhmann, M.U.; Tatagiba, M.; Marquardt, G.; et al. Targetable ERBB2 mutations identified in neurofibroma/schwannoma hybrid nerve sheath tumors. J. Clin. Investig. 2020, 130, 2488–2495. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Tamura, R. Current Understanding of Neurofibromatosis Type 1, 2, and Schwannomatosis. Int. J. Mol. Sci. 2021, 22, 5850. [Google Scholar] [CrossRef]
- Powers, C.J.; Friedman, A.H. A brief history of surgery for peripheral nerve sheath tumors. Neurosurg. Focus 2007, 22, E1. [Google Scholar] [CrossRef] [Green Version]
- Gosk, J.; Zimmer, K.; Rutowski, R. Peripheral nerve tumours—Diagnostic and therapeutical basics. Folia Neuropathol. 2004, 42, 31–35. [Google Scholar]
- Knight, D.M.A.; Birch, R.; Pringle, J. Benign solitary schwannomas: A review of 234 cases. J. Bone Jt. Surgery. Br. Vol. 2007, 89, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Murovic, J.A.; Tiel, R.L.; Moes, G.; Kline, D.G. A series of 397 peripheral neural sheath tumors: 30-year experience at Louisiana State University Health Sciences Center. J. Neurosurg. 2005, 102, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.M. Preserve the nerve: Microsurgical resection of peripheral nerve sheath tumors. Neurosurgery 2007, 61, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Furniss, D.; Swan, M.C.; Morritt, D.G.; Lim, J.; Khanna, T.; Way, B.L.M.; Athanasou, N.A.; Giele, H.; Critchley, P. A 10-year review of benign and malignant peripheral nerve sheath tumors in a single center: Clinical and radiographic features can help to differentiate benign from malignant lesions. Plast. Reconstr. Surg. 2008, 121, 529–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, J.; Sandberg, K.; Søe Nielsen, N.; Dahlin, L.B. Magnetic resonance imaging of peripheral nerve tumours in the upper extremity. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2009, 43, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Kasprian, G.; Amann, G.; Duscher, D.; Aszmann, O.C. Diffusion tensor tractography for the surgical management of peripheral nerve sheath tumors. Neurosurg. Focus 2015, 39, E17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedro, M.T.; Antoniadis, G.; Scheuerle, A.; Pham, M.; Wirtz, C.R.; Koenig, R.W. Intraoperative high-resolution ultrasound and contrast-enhanced ultrasound of peripheral nerve tumors and tumorlike lesions. Neurosurg. Focus 2015, 39, E5. [Google Scholar] [CrossRef] [Green Version]
- Abe, K.; Takeuchi, A.; Yamamoto, N.; Hayashi, K.; Tada, K.; Miwa, S.; Inatani, H.; Aoki, Y.; Higuchi, T.; Tsuchiya, H. Symptomatic small schwannoma is a risk factor for surgical complications and correlates with difficulty of enucleation. Springerplus 2015, 4, 751. [Google Scholar] [CrossRef] [Green Version]
- Syme, J. Lectures on clinical surgery: Lecture XXII Neuromata. Lancet 1855, 1, 551–553. [Google Scholar] [CrossRef] [Green Version]
- Harkin, J.C.; Reed, R.J. Tumors of the Peripheral Nervous System; Atlas of Tumor Pathology; American Registry of Pathology: Silver Spring, MD, USA, 1969. [Google Scholar]
- Stevens, J.; Davis, D.H.; MacCarty, C.S. A 32-year experience with the surgical treatment of selected brachial plexus lesions with emphasis on its reconstruction. Surg. Neurol. 1983, 19, 334–345. [Google Scholar] [CrossRef]
- Handler, S.D.; Canalis, R.F.; Jenkins, H.A.; Weiss, A.J. Management of brachial plexus tumors. Arch. Otolaryngol. 1977, 103, 653–657. [Google Scholar] [CrossRef]
- Donner, T.R.; Voorhies, R.M.; Kline, D.G. Neural sheath tumors of major nerves. J. Neurosurg. 1994, 81, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Kline, D.G.; Judice, D.J. Operative management of selected brachial plexus lesions. J. Neurosurg. 1983, 58, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Gosk, J.; Rutowski, R.; Zimmer, K.; Rabczyński, J. Brachial plexus tumours--own experience in diagnostics and surgical treatment. Folia Neuropathol. 2004, 42, 171–175. [Google Scholar] [PubMed]
- Stone, J.J.; Spinner, R.J. Go for the Gold: A “Plane” and Simple Technique for Resecting Benign Peripheral Nerve Sheath Tumors. Oper. Neurosurg. 2020, 18, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Tiel, R.; Kline, D. Peripheral nerve tumors: Surgical principles, approaches, and techniques. Neurosurg. Clin. N. Am. 2004, 15, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.; Slimp, J.; Born, D.; Goodkin, R.; Kliot, M. The evaluation and management of benign peripheral nerve tumors and masses. In Textbook of Neuro-Oncology; Berger, M.S., Prados, M.D., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2005; pp. 535–563. [Google Scholar]
- Montano, N.; D’Alessandris, Q.G.; D’Ercole, M.; Lauretti, L.; Pallini, R.; Di Bonaventura, R.; La Rocca, G.; Bianchi, F.; Fernandez, E. Tumors of the peripheral nervous system: Analysis of prognostic factors in a series with long-term follow-up and review of the literature. J. Neurosurg. 2016, 125, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Fujibuchi, T.; Miyawaki, J.; Kidani, T.; Miura, H. Risk factors for neurological complications after operative treatment for schwannomas. J. Clin. Neurosci. 2017, 46, 136–140. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n |
|---|---|
| Patients | 31 |
| Tumors | 34 |
| Age | 48 ± 18 |
| Sex (f/m) | 20/11 |
| Side (l/r) | 16/18 |
| Type | Description | Scheme |
|---|---|---|
| Type I | bPNST is located peripherally |  |
| Type II | bPNST splits the nerve into 2 main fascicles |  |
| Type III | bPNST totally splits up the nerve out of the nerve’s center |  |
| Type IV | bPNST encloses nerve fascicles without any detectable boundary layer |  |
| n | Schwannoma | Neurofibroma | Perineurioma | |
|---|---|---|---|---|
| Type I | 16 | 14 | 2 | - |
| Type II | 5 | 5 | - | - |
| Type III | 8 | 7 | - | 1 |
| Type IV | 5 | 2 | 3 | - |
| Σ | 34 | 28 | 5 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzbauer, M.; Aufschnaiter-Hießböck, K.; Zaussinger, M.; Aszmann, O.C.; Schmidt, M. Morphological Relation of Peripheral Nerve Sheath Tumors and Nerve Fascicles: Prospective Study and Classification. J. Clin. Med. 2022, 11, 552. https://doi.org/10.3390/jcm11030552
Holzbauer M, Aufschnaiter-Hießböck K, Zaussinger M, Aszmann OC, Schmidt M. Morphological Relation of Peripheral Nerve Sheath Tumors and Nerve Fascicles: Prospective Study and Classification. Journal of Clinical Medicine. 2022; 11(3):552. https://doi.org/10.3390/jcm11030552
Chicago/Turabian StyleHolzbauer, Matthias, Kathrin Aufschnaiter-Hießböck, Maximilian Zaussinger, Oskar C. Aszmann, and Manfred Schmidt. 2022. "Morphological Relation of Peripheral Nerve Sheath Tumors and Nerve Fascicles: Prospective Study and Classification" Journal of Clinical Medicine 11, no. 3: 552. https://doi.org/10.3390/jcm11030552