
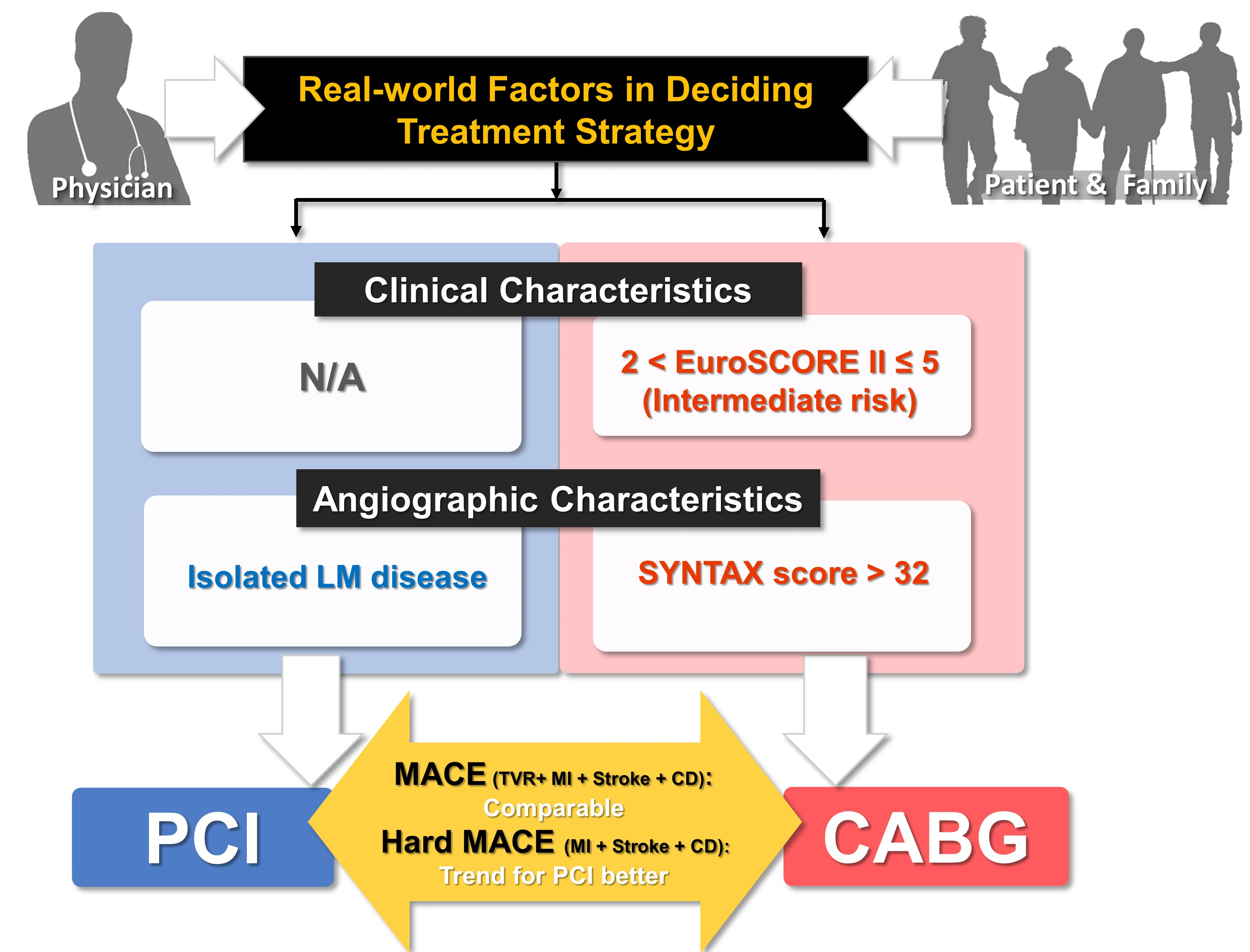
Real-World Treatment Selection Factors and 7-Year Clinical Outcomes between Percutaneous Coronary Intervention and Coronary Artery Bypass Graft Surgery in Left Main Disease

 ,
,  , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Definition of Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Angiographic and Procedural Characteristics
3.3. Factors for the Selection of PCI or CABG
3.4. Long Term Clinical Outcomes: Unadjusted Survival Analysis
3.5. Long Term Clinical Outcomes: Multivariate-Adjusted Survival Analysis and PSM
3.6. Predictors for Composite Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, D.W.; Ahn, J.M.; Park, H.; Yun, S.C.; Kang, D.Y.; Lee, P.H.; Kim, Y.H.; Lim, D.S.; Rha, S.W.; Park, G.M.; et al. Ten-Year Outcomes After Drug-Eluting Stents Versus Coronary Artery Bypass Grafting for Left Main Coronary Disease: Extended Follow-Up of the PRECOMBAT Trial. Circulation 2020, 141, 1437–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, N.R.; Makikallio, T.; Lindsay, M.M.; Spence, M.S.; Erglis, A.; Menown, I.B.A.; Trovik, T.; Kellerth, T.; Kalinauskas, G.; Mogensen, L.J.H.; et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in the treatment of unprotected left main stenosis: Updated 5-year outcomes from the randomised, non-inferiority NOBLE trial. Lancet 2020, 395, 191–199. [Google Scholar] [CrossRef]
- Thuijs, D.; Kappetein, A.P.; Serruys, P.W.; Mohr, F.W.; Morice, M.C.; Mack, M.J.; Holmes, D.R., Jr.; Curzen, N.; Davierwala, P.; Noack, T.; et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet 2019, 394, 1325–1334. [Google Scholar] [CrossRef]
- Stone, G.W.; Kappetein, A.P.; Sabik, J.F.; Pocock, S.J.; Morice, M.C.; Puskas, J.; Kandzari, D.E.; Karmpaliotis, D.; Brown, W.M., 3rd; Lembo, N.J.; et al. Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease. N. Engl. J. Med. 2019, 381, 1820–1830. [Google Scholar] [CrossRef] [PubMed]
- Hanger, H.C.; Fogarty, B.; Wilkinson, T.J.; Sainsbury, R. Stroke patients’ views on stroke outcomes: Death versus disability. Clin. Rehabil. 2000, 14, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Averitt, A.J.; Weng, C.; Ryan, P.; Perotte, A. Translating evidence into practice: Eligibility criteria fail to eliminate clinically significant differences between real-world and study populations. NPJ Digital Med. 2020, 3, 67. [Google Scholar] [CrossRef] [PubMed]
- Munk, N.E.; Knudsen, J.S.; Pottegård, A.; Witte, D.R.; Thomsen, R.W. Differences Between Randomized Clinical Trial Participants and Real-World Empagliflozin Users and the Changes in Their Glycated Hemoglobin Levels. JAMA Netw. Open 2020, 3, e1920949. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology; American College of Cardiology; American Heart Association; et al. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Caggegi, A.; Miano, M.; Cincotta, G.; Dipasqua, F.; Giacchi, G.; Capranzano, P.; Ussia, G.; Di Salvo, M.E.; La Manna, A.; et al. Global risk classification and clinical SYNTAX (synergy between percutaneous coronary intervention with TAXUS and cardiac surgery) score in patients undergoing percutaneous or surgical left main revascularization. JACC Cardiovasc. Interv. 2011, 4, 287–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, 2574–2609. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Morice, M.C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Stahle, E.; Feldman, T.E.; van den Brand, M.; Bass, E.J.; et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 360, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Bakal, J.A.; Westerhout, C.M.; Cantor, W.J.; Fernandez-Aviles, F.; Welsh, R.C.; Fitchett, D.; Goodman, S.G.; Armstrong, P.W. Evaluation of early percutaneous coronary intervention vs. standard therapy after fibrinolysis for ST-segment elevation myocardial infarction: Contribution of weighting the composite endpoint. Eur. Heart J. 2013, 34, 903–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.A.; Andrew, M.J.; Schrader, G.; Knight, J.L. Preoperative depression and mortality in coronary artery bypass surgery: Preliminary findings. ANZ J. Surg. 2001, 71, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E.; Cannon, C.P.; McCabe, C.H. An approach to evaluating thrombolytic therapy in acute myocardial infarction. The ‘unsatisfactory outcome’ end point. Circulation 1992, 86, 683–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolker, J.M.; Spertus, J.A.; Cohen, D.J.; Jones, P.G.; Jain, K.K.; Bamberger, E.; Lonergan, B.B.; Chan, P.S. Rethinking composite end points in clinical trials: Insights from patients and trialists. Circulation 2014, 130, 1254–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 230) | PCI (n = 118) | CABG (n = 112) | p | |
|---|---|---|---|---|
| Age (years) | 64.1 ± 9.5 | 64.0 ± 10.3 | 64.28 ± 8.6 | 0.85 |
| Male sex, n (%) | 166 (72) | 83 (75) | 83 (69) | 0.56 |
| HTN, n (%) | 136 (59) | 66 (56) | 70 (63) | 0.35 |
| DM, n (%) | 81 (35) | 37 (31) | 44 (39) | 0.22 |
| Dyslipidemia, n (%) | 53 (23) | 31 (38) | 22 (24) | 0.27 |
| Current smoker, n (%) | 55 (24) | 29 (25) | 26 (20) | 0.96 |
| LVEF | 58.8 ± 12.3 | 60.7 ± 11.1 | 56.8 ± 13.2 | 0.02 |
| ACS, n (%) | 155 (67) | 74 (11) | 79 (15.7) | 0.26 |
| PAD, n (%) | 7 (3) | 3 (3) | 4 (4) | 0.72 |
| CKD, n (%) | 15 (7) | 8 (7) | 7 (6) | 1.00 |
| Previous MI, n (%) | 9 (4) | 4 (3) | 5 (5) | 0.74 |
| History of CVA, n (%) | 14 (6) | 8 (7) | 6 (5) | 0.79 |
| History of PCI, n (%) | 30 (13) | 14 (12) | 16 (14) | 0.70 |
| EuroSCORE II | 1.65 ± 1.31 | 1.43 ± 1.35 | 1.90 ± 1.23 | 0.01 |
| Total (n = 230) | PCI (n = 118) | CABG (n = 112) | p | |
|---|---|---|---|---|
| Lesions characteristics | ||||
| Total SYNTAX score | 26.8 ± 11.2 | 20.7 ± 8.2 | 33.1 ± 10.4 | <0.01 |
| SYNTAX score of LM | 12.8 ± 2.6 | 12.4 ± 2.2 | 13.1 ± 3.0 | 0.03 |
| Low to intermediate SYNTAX score, n (%) | 155 (67) | 104 (88) | 51 (46) | <0.01 |
| Number of Lesions | 3.3 ± 1.5 | 2.6 ± 1.3 | 4.0 ± 1.4 | <0.01 |
| CTO lesions, n (%) | 62 (27) | 15 (13) | 47 (42) | <0.01 |
| Distal LM bifurcation disease, n (%) | 166 (72) | 83 (70) | 83 (74) | 0.56 |
| Extent of lesion | <0.01 | |||
| Isolated LM disease, n (%) | 21 (9) | 18 (15) | 3 (3) | |
| LM and 1-VD, n (%) | 42 (18) | 32 (27) | 10 (9) | |
| LM and 2-VD, n (%) | 59 (26) | 37 (31) | 42 (38) | |
| LM and 3-VD, n (%) | 88 (38) | 31 (26) | 57 (51) | |
| Procedural characteristics | ||||
| Single-stent technique | 93 (78.8) | |||
| Two-stent technique | 25 (21.2) | |||
| Main vessel stent diameter (mm) | - | 3.4 ± 0.4 | - | - |
| Main vessel stent length (mm) | - | 20.9 ± 8.5 | - | - |
| Side branch stent diameter (mm) | - | 3.1 ± 0.5 | - | - |
| Side branch stent length (mm) | - | 17.4 ± 4.0 | - | - |
| Number of grafts | - | 2.3 ± 0.5 | - | |
| Use of left internal mammary artery | 106 (94.6) | |||
| Off-pump surgery | 48 (42.9) | |||
| PCI, n (%) | CABG, n (%) | HR (95% CI) | p | |
|---|---|---|---|---|
| Cardiac death | ||||
| Unadjusted | 12 (10.2) | 17 (15.2) | 0.65 (0.31–1.35) | 0.25 |
| Multivariable adjusted * | - | - | 0.42 (0.16–1.12) | 0.08 |
| Post-PSM | 7 (10.6) | 11 (16.7) | 0.63 (0.25–1.63) | 0.34 |
| MI | ||||
| Unadjusted | 3 (2.5) | 4 (3.6) | 0.69 (0.16–3.02 | 0.62 |
| Multivariable adjusted * | - | - | 0.67 (0.07–6.60) | 0.73 |
| Post-PSM | 3 (4.5) | 3 (4.5) | 0.66 (0.11–3.98) | 0.65 |
| TVR | ||||
| Unadjusted | 12 (10.2) | 3 (2.7) | 3.25 (1.18–8.96) | 0.02 |
| Multivariable adjusted * | - | - | 9.71 (1.41–67.08) | 0.02 |
| Post-PSM | 7 (10.6) | 1 (1.5) | 7.33 (0.90–59.63) | 0.06 |
| Stroke | ||||
| Unadjusted | 3 (2.5) | 8 (7.1) | 0.35 (0.11–1.16) | 0.09 |
| Multivariable adjusted * | - | - | 0.22 (0.04–1.26) | 0.09 |
| Post-PSM | 2 (3.0) | 4 (6.1) | 0.48 (0.09–2.60) | 0.39 |
| MACE | ||||
| Unadjusted | 25 (21.2) | 28 (25.0) | 0.83 (0.48–1.42) | 0.49 |
| Multivariable adjusted * | - | - | 0.97 (0.48–1.94) | 0.92 |
| Post-PSM | 15 (22.7) | 15 (22.7) | 1.01 (0.49–2.10) | 0.99 |
| Hard MACE | ||||
| Unadjusted | 16 (13.6) | 26 (23.2) | 0.55 (0.30–1.02) | 0.06 |
| Multivariable adjusted * | - | - | 0.49 (0.22–1.07) | 0.07 |
| Post-PSM | 9 (13.6) | 15 (22.7) | 0.57 (0.25–1.30) | 0.18 |
| Covariate | MACE | Hard MACE * | ||||
|---|---|---|---|---|---|---|
| HRadj | 95% CI | p | HRadj | 95% CI | p | |
| PCI vs. CABG | 0.97 | 0.48–1.94 | 0.92 | 0.49 | 0.22–1.07 | 0.07 |
| Age | 0.99 | 0.95–1.04 | 0.73 | 1.03 | 0.98–1.08 | 0.30 |
| Male | 0.50 | 0.27–0.92 | 0.03 | 0.56 | 0.28–1.12 | 0.10 |
| HTN | 2.53 | 1.11–5.78 | 0.03 | 2.44 | 0.93–6.43 | 0.07 |
| DM | 0.91 | 0.50–1.67 | 0.77 | 0.99 | 0.50–1.96 | 0.97 |
| ACS | 0.60 | 0.30–1.18 | 0.14 | 0.60 | 0.26–1.36 | 0.22 |
| CKD | 2.30 | 1.14–4.60 | 0.02 | 2.30 | 1.06–4.95 | 0.03 |
| LVEF | 1.00 | 0.97–1.02 | 0.92 | 1.00 | 0.97–1.03 | 0.92 |
| EuroSCORE II | 1.54 | 1.23–1.93 | <0.01 | 1.59 | 1.25–2.02 | <0.01 |
| CTO | 1.52 | 0.69–3.35 | 0.30 | 1.33 | 0.54–3.30 | 0.54 |
| SYNTAX score > 32 | 0.98 | 0.44–2.20 | 0.97 | 0.88 | 0.37–2.10 | 0.78 |
| Distal LM bifurcation | 1.43 | 0.69–2.96 | 0.34 | 1.09 | 0.49–2.45 | 0.83 |
| Isolated LM disease | 0.60 | 0.14–2.63 | 0.50 | 0.50 | 0.06–3.93 | 0.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, A.Y.; Kim, M.; Lee, J.; Seo, J.; Shin, Y.H.; Oh, P.C.; Suh, S.Y.; Lee, K.; Kang, W.C.; Ahn, T.; et al. Real-World Treatment Selection Factors and 7-Year Clinical Outcomes between Percutaneous Coronary Intervention and Coronary Artery Bypass Graft Surgery in Left Main Disease. J. Clin. Med. 2022, 11, 503. https://doi.org/10.3390/jcm11030503
Jang AY, Kim M, Lee J, Seo J, Shin YH, Oh PC, Suh SY, Lee K, Kang WC, Ahn T, et al. Real-World Treatment Selection Factors and 7-Year Clinical Outcomes between Percutaneous Coronary Intervention and Coronary Artery Bypass Graft Surgery in Left Main Disease. Journal of Clinical Medicine. 2022; 11(3):503. https://doi.org/10.3390/jcm11030503
Chicago/Turabian StyleJang, Albert Youngwoo, Minsu Kim, Joonpyo Lee, Jeongduk Seo, Yong Hoon Shin, Pyung Chun Oh, Soon Yong Suh, Kyounghoon Lee, Woong Chol Kang, Taehoon Ahn, and et al. 2022. "Real-World Treatment Selection Factors and 7-Year Clinical Outcomes between Percutaneous Coronary Intervention and Coronary Artery Bypass Graft Surgery in Left Main Disease" Journal of Clinical Medicine 11, no. 3: 503. https://doi.org/10.3390/jcm11030503