
Evaluating the Value of Anti-SARS-CoV-2 Antibody-Based Tests for COVID-19 Diagnosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Ethics Statement
2.2. Nucleic Acid Test
2.3. Total Antibody Testing
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Diagnostic Performance of the RT-PCR Test on Different Quarantines for COVID-19
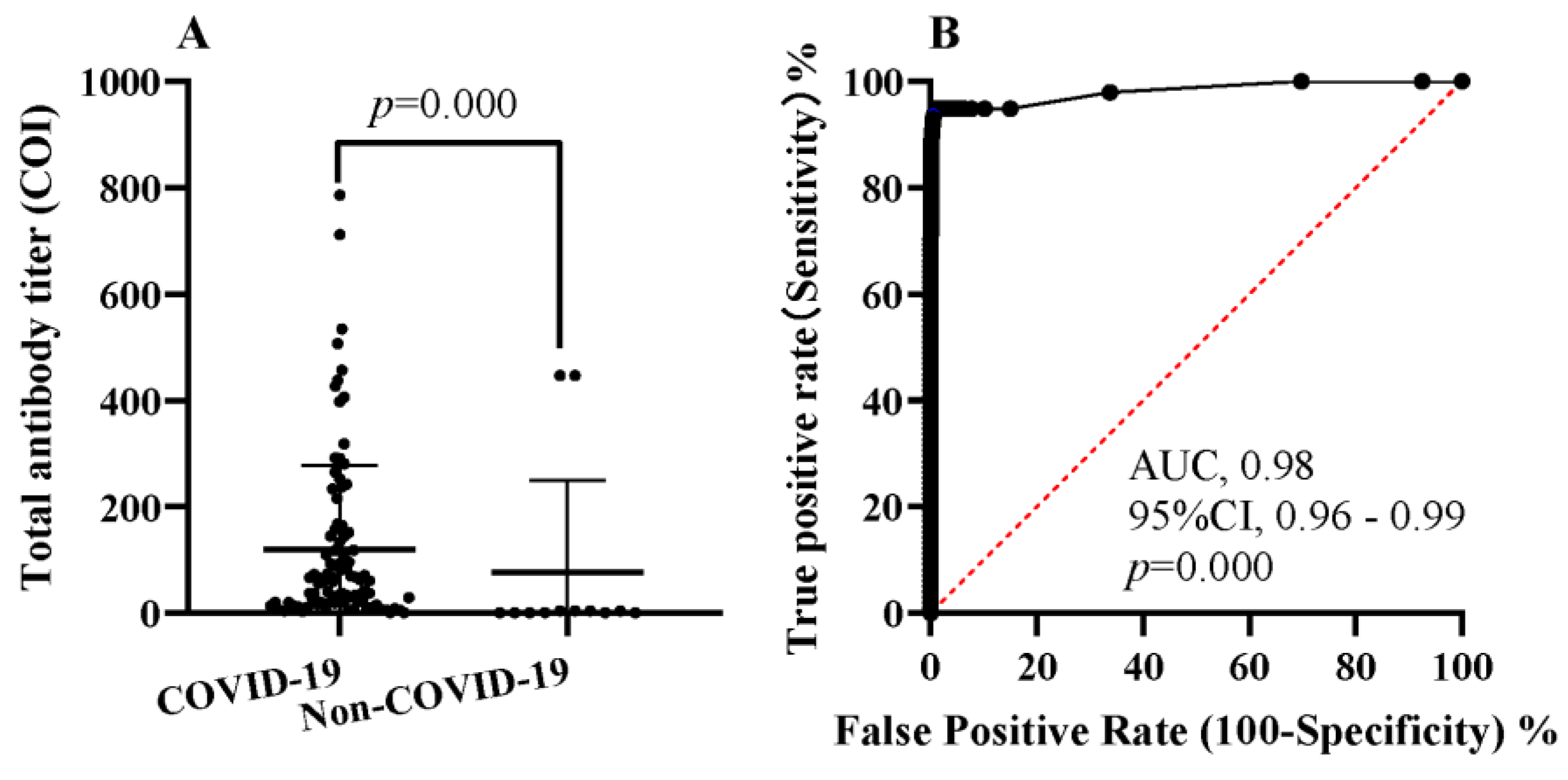
3.3. Diagnostic Performance of the Total Antibody Test for COVID-19
3.4. Comparison of the RT-PCR and Total Antibodies for COVID-19 Patients in Different Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeling, R.W.; Heymann, D.L.; Teo, Y.-Y.; Garcia, P.J. Diagnostics for COVID-19: Moving from pandemic response to control. Lancet 2022, 399, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Sule, W.F.; Oluwayelu, D.O. Real-time RT-PCR for COVID-19 diagnosis: Challenges and prospects. Pan Afr. Med. J. 2020, 35, 121. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Finana, M.; Buchan, I.E. Rapid antigen testing in COVID-19 responses. Science 2021, 372, 571–572. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Winkel, B.; Schram, E.; Gremmels, H.; Debast, S.; Schuurman, R.; Wensing, A.; Bonten, M.; Goedhart, E.; Hofstra, M.; Antigen Rapid Test Validation Group. Screening for SARS-CoV-2 infection in asymptomatic individuals using the Panbio COVID-19 antigen rapid test (Abbott) compared with RT-PCR: A prospective cohort study. BMJ Open 2021, 11, e048206. [Google Scholar] [CrossRef] [PubMed]
- Mandeng, N.; Fai, K.N.; Bebell, L.M.; Boum, Y. Negative antigen RDT and RT-PCR results do not rule out COVID-19 if clinical suspicion is strong Reply. Lancet Infect. Dis. 2021, 21, 1210. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Tirupathi, R.; Sule, A.A.; Aldali, J.; Mutair, A.A.; Alhumaid, S.; Gupta, N.; Koritala, T.; Adhikari, R.; Bilal, M.; et al. Viral Dynamics and Real-Time RT-PCR Ct Values Correlation with Disease Severity in COVID-19. Diagnostics 2021, 11, 1091. [Google Scholar] [CrossRef] [PubMed]
- Kucirka, L.; Lauer, S.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction-Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Wakui, M.; Uwamino, Y.; Kurafuji, T.; Noguchi, M.; Ohno, A.; Yokota, H.; Kikuchi, H.; Hasegawa, N.; Saya, H.; Murata, M.; et al. Assessment of humoral responses in COVID-19 using various quantitative antibody tests. Ann. Clin. Biochem. 2021, 58, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Wei, P.F. Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin. Med. J. 2020, 133, 1087–1095. [Google Scholar]
- Bouman, T.; Steg, L.; Dietz, T. Insights from early COVID-19 responses about promoting sustainable action. Nat. Sustain. 2020, 4, 194–200. [Google Scholar] [CrossRef]
- Wang, Y.J.; Xue, J.H.; Fang, Z.X.; Xie, J.W.; Niu, J.J.; Yang, T.C.; Lin, L.R. A 14+ 7 day quarantine period and a dual nucleic acid testing reagent strategy detect potentially indiscoverable Coronavirus disease 2019 infections in Xiamen, China. Clin. Chim. Acta Int. J. Clin. Chem. Appl. Mol. Biol. 2022, 532, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Kankam, H.K.N.; Hourston, G.J.M.; Ravindran, P.; Azhar, B.; Pope, C. COVID-19 antibody tests: Statistical implications. Br. J. Hosp. Med. 2020, 81, 1–5. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| RT-PCR | Clinical Diagnosis (Gold Standard) | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | Positive Predictive Value (%) (95% CI) | Negative Predictive Value (%) (95% CI) | Accuracy (%) (95% CI) | Kappa (95% CI) | ||
|---|---|---|---|---|---|---|---|---|---|
| COVID-19 | Non-COVID-19 | ||||||||
| Day 1 | Positive | 14 | 0 | 14.29 | 100 | 100 | 97.30 | 97.31 | 0.24 |
| Negative | 84 | 3022 | (7.36–21.21) | (99.87–100) | (78.5–100) | (96.67–97.81) | (96.74–97.88) | (0.14–0.35) | |
| Up to day 7 | Positive | 70 | 0 | 71.43 | 100 | 100 | 97.58 | 99.10 | 0.82 |
| Negative | 28 | 3022 | (61.81–79.43) | (99.87–100) | (94.80–100) | (96.68–98.36) | (98.77–99.43) | (0.76–0.89) | |
| Up to day 14 | Positive | 84 | 0 | 85.71 | 100 | 100 | 99.54 | 99.55 | 0.92 |
| Negative | 14 | 3022 | (77.44–91.30) | (99.87–100) | (95.63–100) | (99.23–99.73) | (99.32–99.79) | (0.87–0.96) | |
| Total Antibody | Clinical Diagnosis (Gold Standard) | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | Positive Predictive Value (%) (95% CI) | Negative Predictive Value (%) (95% CI) | Accuracy (%) (95% CI) | Kappa (95% CI) | |
|---|---|---|---|---|---|---|---|---|
| COVID-19 | Non-COVI D-19 | |||||||
| Positive | 92 | 18 | 93.88 | 99.40 | 83.64 | 99.80 | 99.23 | 0.88 |
| Negative | 6 | 3004 | 87.28–97.16 | 99.06–99.62 | 75.61–89.39 | 99.57–99.91 | 98.92–99.54 | (0.83 0.93) |
| Test | Symptomatic COVID-19 (n = 27) | Asymptomatic COVID-19 (n = 71) | Statistical Analysis * | Statistical Analysis # |
|---|---|---|---|---|
| Positive Case n (%) | Positive Case n (%) | |||
| RT-PCR | 2 (7.41) | 12 (16.90) | χ2 = 1.440, p = 0.338 | χ2 = 47.725, p = 0.000 |
| Total antibody | 26 (96.30) | 66 (92.96) | χ2 = 0.379, p = 0.676 | χ2 = 82.947, p = 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.-L.; Xie, J.-W.; Wang, M.; Lin, M.-Q.; Zheng, Y.-W.; Lin, L.-R. Evaluating the Value of Anti-SARS-CoV-2 Antibody-Based Tests for COVID-19 Diagnosis. J. Clin. Med. 2022, 11, 7489. https://doi.org/10.3390/jcm11247489
Yu X-L, Xie J-W, Wang M, Lin M-Q, Zheng Y-W, Lin L-R. Evaluating the Value of Anti-SARS-CoV-2 Antibody-Based Tests for COVID-19 Diagnosis. Journal of Clinical Medicine. 2022; 11(24):7489. https://doi.org/10.3390/jcm11247489
Chicago/Turabian StyleYu, Xiao-Lu, Jia-Wen Xie, Mao Wang, Mei-Qi Lin, Ya-Wen Zheng, and Li-Rong Lin. 2022. "Evaluating the Value of Anti-SARS-CoV-2 Antibody-Based Tests for COVID-19 Diagnosis" Journal of Clinical Medicine 11, no. 24: 7489. https://doi.org/10.3390/jcm11247489