
Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer: Where Are We Now and What Does the Future Entail?
 , ,
, ,
Abstract
:1. Introduction
2. Discussion
2.1. Artificial Intelligence and Its Utility in Gastroenterology
- Application in Premalignant Lesions: Esophagogastroduodenoscopy (EGD) and colonoscopy are pivotal procedures in diagnosing upper and lower premalignant GI lesions. However, there is significant variability in premalignant lesion detection due to the endoscopists’ skill level. To standardize and improve the quality of EGDs and colonoscopies, AI-assisted models have been utilized. In current literature, two randomized controlled trials (RCTs) have compared the endoscopic performance for the diagnosis of premalignant lesions between AI-assisted and non-AI-assisted models. The WISENSE system, which used deep convolutional neural networks (CNNs) and deep reinforcement learning, reported lower rates of blind spots (5.86% vs. 22.46%, p < 0.001) during EGD for upper GI lesions compared to the non-AI-assisted control group [25]. The authors ultimately concluded that the WISENSE system significantly improved the quality of EGDs [25]. Another RCT by Wang et al. noted a significantly higher adenoma detection rate (ADR; 29.1% vs. 20.3%, p < 0.001) and mean number of adenomas per patient (0.53 vs. 0.31, p < 0.001) for diagnostic colonoscopy for an AI-mediated real-time automatic polyp detection system that provided audio-visual alerts upon polyp detection compared to diagnostic colonoscopies without the assistance of an AI system [26].
- Application in Malignant Lesions: AI can help gastroenterologists accurately determine the prognosis of malignant GI neoplasms compared to conventional non-AI models [27,28,29,30]. A study by Gohari et al. compared the accuracy of prediction of survival rates for patients with colorectal cancer between an ANN AI-assisted model and Cox regression models [27]. The authors noted that the ANN model had more accurate predictions of survival for colon (89% vs. 78.6%) and rectal (82.7% vs. 70.7%) cancer patients compared to the Cox regression models [27]. Biglarian et al. compared the accuracy of prediction of distant metastasis for colorectal cancer between an ANN AI-assisted model and logistic regression models [28]. The authors observed that the ANN model had higher accuracy in predicting distant metastasis (area under the receiver operating characteristic curve (AUROC): 0.82 vs. 0.77) compared to the logistic regression models [28]. Another study by Nilsaz-Dezfouli et al. demonstrated the utility of a single time-point feed-forward ANN AI-assisted model to predict the probability of survival for gastric cancer patients at 1, 2, 3, 4, and 5 years after surgery [29]. The authors concluded that the prediction of survival for the ANN model was consistently accurate (88.7–90.2%), with sensitivity and specificity ranging from 70.2–92.5% and 66.7–96.2%, respectively [29]. Furthermore, DL algorithms have also found applications in the detection and treatment of GI malignancies [31,32,33]. A systematic review and meta-analysis of five RCTs (4354 patients) that assessed the performance of a DL computer-aided polyp detection system for the detection of colorectal neoplasia noted a significantly higher pooled adenoma detection rate (36.6% vs. 25.2%, RR 1.44; 95% confidence interval (CI) 1.27–1.62; p < 0.01; I2 = 42%) and adenomas detected per colonoscopy (58% vs. 36%, RR 1.70; 95% CI 1.53–1.89; p < 0.01; I2 = 33%) for the AI-assisted model compared to the control group [31]. From a treatment perspective, DL models can predict clinical response to chemotherapy and radiation with high accuracy (≥80%) [32,33].
- Application in Inflammatory Lesions: Numerous studies have investigated the use of AI-assisted models to identify a wide spectrum of inflammatory lesions. For identifying patients with inflammatory bowel disease (IBD), the support vector machine (SVM) model, a type of machine learning algorithm, had diagnostic accuracy, sensitivity, and specificity ranging from 80–100%, 80–95.2%, and 92.4–93.6%, respectively, using endoscopic or wireless capsule endoscopy (WCE) images as input data [20]. The SVM model has also been used to detect ulcerative disease (peptic ulcers, ulcers from Crohn’s disease, NSAID-induced ulcers, and unexplained ulcers) with high accuracy (74–96.3%), sensitivity (75–100%), and specificity (73.3–100%) [20]. Furthermore, a study by Cui et al. used an adaptive threshold classifier AI-assisted model on 7218 small bowel WCE images to identify lymphangiectasia with a diagnostic accuracy of 97.9% [20]. Another study by Wu et al. used the Rustboost AI-assisted model on small bowel WCE images from 10 patients to identify individuals with a hookworm infection with the accuracy, sensitivity, and specificity of 78.2%, 77.2%, and 77.9%, respectively [20]. In patients with celiac disease, the diagnostic accuracy of AI-assisted models ranges from 76.7–99.6% [20].
- Application in Gastrointestinal Bleeding: GI bleeding is a common medical emergency associated with significant morbidity and mortality. In the current literature, twelve studies have assessed the use of AI-assisted models to detect small bowel bleeding using WCE images/videos as input data [20,34,35,36,37,38,39,40,41,42,43]. Of these, six studies using an SVM AI-assisted model to identify patients with small bowel bleeding reported diagnostic accuracy ranging from 91.8–99.6% [35,36,37,39,40,41]. Additionally, five studies that utilized various AI-assisted models, such as multilayer perceptron network (MLP), probabilistic neural network, joint diagonalization principal component analysis, and CNN reported diagnostic accuracy ranging from 87.4–98% [20,34,38,42,43]. However, a study by Jung et al. that utilized a color spectrum transformation AI-assisted model to identify small bowel GI bleeding using WCE images as input data had a diagnostic accuracy of only 30% but a sensitivity and specificity of 94.9% and 96.1%, respectively [20].
- Application in Hepatology: The utilization of AI-assisted models to detect liver fibrosis, non-alcoholic fatty liver disease (NAFLD), and esophageal varices has increased exponentially in recent years. Seven studies that used AI-assisted models to detect liver fibrosis associated with viral hepatitis (hepatitis B and C viruses) reported diagnostic accuracy of ≥84.4% [20]. The diagnostic accuracy of AI-assisted models from six studies that aimed to identify individuals with NAFLD ranged from 79% to 89% [20]. Two studies that used MLP and random forest AI-assisted models to detect esophageal varices noted a diagnostic accuracy of 87.8% and 0.82 (AUROC), respectively [20]. Overall, these AI models identified their target factor with ≥80% accuracy.
2.2. Utilization of Artificial Intelligence in Endoscopic Ultrasound for the Detection of Pancreatic Cancer
2.3. Utilization of Artificial Intelligence in Endoscopic Ultrasound to Differentiate Pancreatic Cancer from Chronic Pancreatitis
2.4. Utilization of Artificial Intelligence in Endoscopic Ultrasound to Differentiate Pancreatic Cancer from Autoimmune Pancreatitis
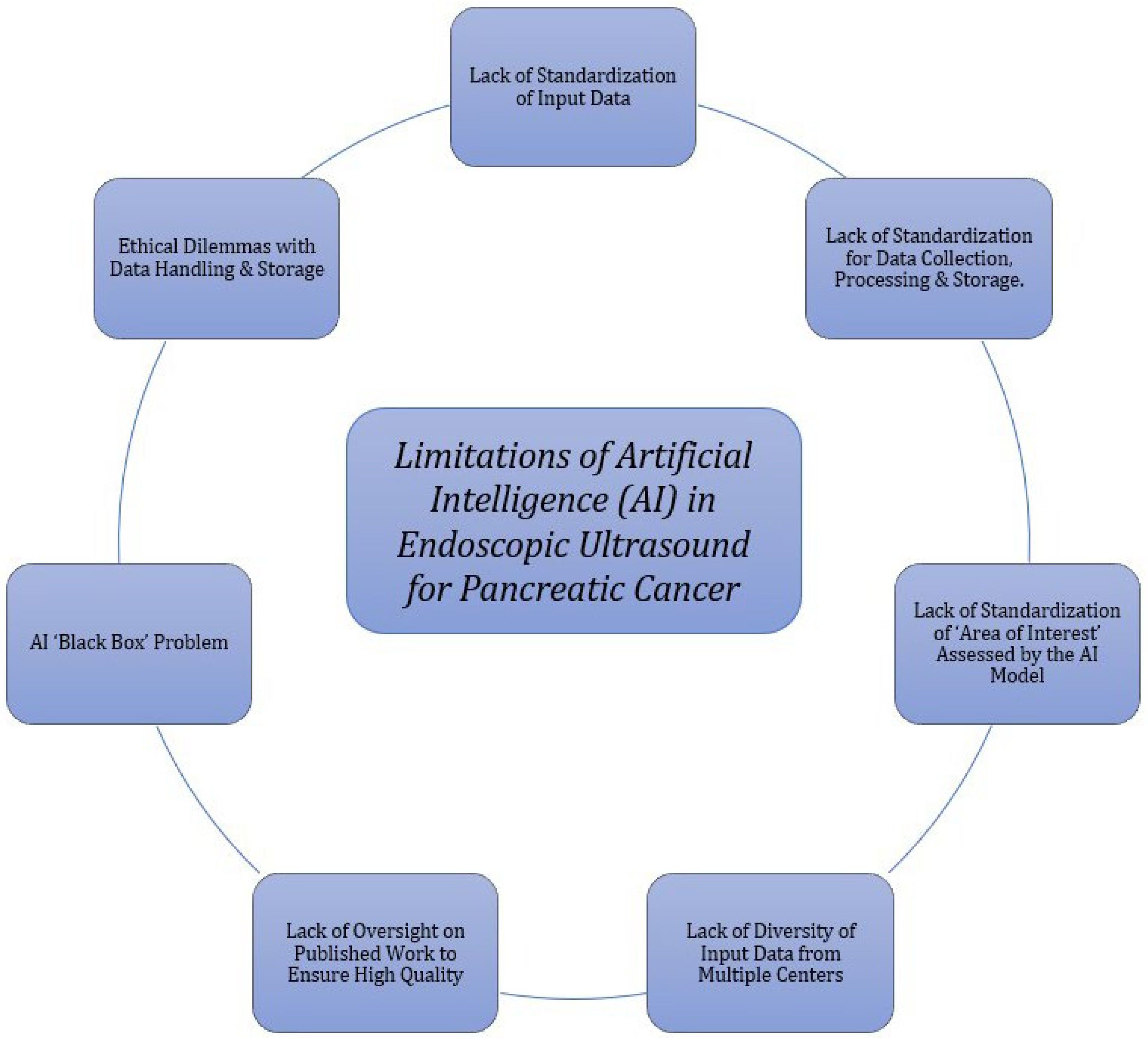
2.5. Limitations of Artificial Intelligence in Endoscopic Ultrasound for the Detection of Pancreatic Cancer
2.6. Future Directions of Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer
2.6.1. ‘Near’ Future Application of Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer
2.6.2. ‘Far’ Future Application of Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zheng, Y.; Yang, F.; Zhu, L.; Zhu, X.Q.; Wang, Z.F.; Wu, X.-L.; Zhou, C.-H.; Yan, J.-Y.; Hu, B.-Y.; et al. The molecular biology of pancreatic adenocarcinoma: Translational challenges and clinical perspectives. Signal Transduct. Target. Ther. 2021, 6, 249. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Liu, W. Pancreatic Cancer: A Review of Risk Factors, Diagnosis, and Treatment. Technol. Cancer Res. Treat. 2020, 19, 1533033820962117. [Google Scholar] [PubMed]
- National Cancer Institute: Surveillance Epidemiology, and End Results (SEER) Program. Cancer Stats Facts: Pancreatic Cancer: National Cancer Institute. 2022. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html (accessed on 3 September 2022).
- Kikuyama, M.; Kamisawa, T.; Kuruma, S.; Chiba, K.; Kawaguchi, S.; Terada, S.; Satoh, T. Early Diagnosis to Improve the Poor Prognosis of Pancreatic Cancer. Cancers 2018, 10, 48. [Google Scholar]
- Iglesias-Garcia, J.; Poley, J.W.; Larghi, A.; Giovannini, M.; Petrone, M.C.; Abdulkader, I.; Monges, G.; Costamagna, G.; Arcidiacono, P.; Biermann, K.; et al. Feasibility and yield of a new EUS histology needle: Results from a multicenter, pooled, cohort study. Gastrointest. Endosc. 2011, 73, 1189–1196. [Google Scholar] [CrossRef]
- Crinò, S.F.; Di Mitri, R.; Nguyen, N.Q.; Tarantino, I.; de Nucci, G.; Deprez, P.H.; Carrara, S.; Kitano, M.; Shami, V.M.; Fernández-Esparrach, G.; et al. Endoscopic Ultrasound-guided Fine-needle Biopsy with or Without Rapid On-site Evaluation for Diagnosis of Solid Pancreatic Lesions: A Randomized Controlled Non-Inferiority Trial. Gastroenterology 2021, 161, 899–909.e5. [Google Scholar] [CrossRef]
- Goyal, H.; Sherazi, S.A.A.; Mann, R.; Gandhi, Z.; Perisetti, A.; Aziz, M.; Chandan, S.; Kopel, J.; Tharian, B.; Sharma, N.; et al. Scope of Artificial Intelligence in Gastrointestinal Oncology. Cancers 2021, 13, 5494. [Google Scholar] [CrossRef]
- Cao, J.S.; Lu, Z.Y.; Chen, M.Y.; Zhang, B.; Juengpanich, S.; Hu, J.H.; Li, S.-J.; Topatana, W.; Zhou, X.-Y.; Feng, X.; et al. Artificial intelligence in gastroenterology and hepatology: Status and challenges. World J. Gastroenterol. 2021, 27, 1664–1690. [Google Scholar] [CrossRef]
- Panch, T.; Szolovits, P.; Atun, R. Artificial intelligence, machine learning and health systems. J. Glob. Health 2018, 8, 020303. [Google Scholar] [CrossRef]
- Gonzalo-Marin, J.; Vila, J.J.; Perez-Miranda, M. Role of endoscopic ultrasound in the diagnosis of pancreatic cancer. World J. Gastrointest. Oncol. 2014, 6, 360–368. [Google Scholar] [CrossRef]
- Liu, E.; Bhutani, M.S.; Sun, S. Artificial intelligence: The new wave of innovation in EUS. Endosc. Ultrasound 2021, 10, 79–83. [Google Scholar]
- Hsieh, M.H.; Sun, L.M.; Lin, C.L.; Hsieh, M.J.; Hsu, C.Y.; Kao, C.H. Development of a prediction model for pancreatic cancer in patients with type 2 diabetes using logistic regression and artificial neural network models. Cancer Manag. Res. 2018, 10, 6317–6324. [Google Scholar] [CrossRef] [Green Version]
- Kenner, B.; Chari, S.T.; Kelsen, D.; Klimstra, D.S.; Pandol, S.J.; Rosenthal, M.; Rustgi, A.K.; Taylor, J.A.; Yala, A.; Abul-Husn, N.; et al. Artificial Intelligence and Early Detection of Pancreatic Cancer: 2020 Summative Review. Pancreas 2021, 50, 251–279. [Google Scholar] [CrossRef]
- Lovejoy, C.A.; Arora, A.; Buch, V.; Dayan, I. Key considerations for the use of artificial intelligence in healthcare and clinical research. Future Healthc. J. 2022, 9, 75–78. [Google Scholar] [CrossRef]
- Jones, L.D.; Golan, D.; Hanna, S.A.; Ramachandran, M. Artificial intelligence, machine learning and the evolution of healthcare: A bright future or cause for concern? Bone Joint Res. 2018, 7, 223–225. [Google Scholar] [CrossRef]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 64. [Google Scholar] [CrossRef] [Green Version]
- Le Berre, C.; Sandborn, W.J.; Aridhi, S.; Devignes, M.D.; Fournier, L.; Smaïl-Tabbone, M.; Danese, S.; Peyrin-Biroulet, L. Application of Artificial Intelligence to Gastroenterology and Hepatology. Gastroenterology 2020, 158, 76–94.e2. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Gao, J.; Zhao, D. A review of the application of deep learning in medical image classification and segmentation. Ann. Transl. Med. 2020, 8, 713. [Google Scholar] [CrossRef]
- Shahid, N.; Rappon, T.; Berta, W. Applications of artificial neural networks in health care organizational decision-making: A scoping review. PLoS ONE 2019, 14, e0212356. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Mohamed, K.; Zeeshan, S.; Dong, X. Artificial intelligence with multi-functional machine learning platform development for better healthcare and precision medicine. Database 2020, 2020, baaa010. [Google Scholar] [CrossRef] [PubMed]
- Kinney, E.L. Medical expert systems. Who needs them? Chest 1987, 91, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhang, J.; Zhou, W.; An, P.; Shen, L.; Liu, J.; Jiang, X.; Huang, X.; Mu, G.; Wan, X.; et al. Randomised controlled trial of WISENSE, a real-time quality improving system for monitoring blind spots during esophagogastroduodenoscopy. Gut 2019, 68, 2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Berzin, T.M.; Glissen Brown, J.R.; Bharadwaj, S.; Becq, A.; Xiao, X.; Liu, P.; Li, L.; Song, Y.; Zhang, D.; et al. Real-time automatic detection system increases colonoscopic polyp and adenoma detection rates: A prospective randomised controlled study. Gut 2019, 68, 1813–1819. [Google Scholar] [CrossRef] [Green Version]
- Gohari, M.R.; Biglarian, A.; Bakhshi, E.; Pourhoseingholi, M.A. Use of an artificial neural network to determine prognostic factors in colorectal cancer patients. Asian Pac. J. Cancer Prev. 2011, 12, 1469–1472. [Google Scholar]
- Biglarian, A.; Bakhshi, E.; Gohari, M.R.; Khodabakhshi, R. Artificial neural network for prediction of distant metastasis in colorectal cancer. Asian Pac. J. Cancer Prev. 2012, 13, 927–930. [Google Scholar] [CrossRef] [Green Version]
- Nilsaz-Dezfouli, H.; Abu-Bakar, M.R.; Arasan, J.; Adam, M.B.; Pourhoseingholi, M.A. Improving Gastric Cancer Outcome Prediction Using Single Time-Point Artificial Neural Network Models. Cancer Inform. 2017, 16, 1176935116686062. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.H.; Fang, Y.J.; Li, C.X.; Ou, Q.J.; Jiang, W.; Lu, S.X.; Lu, Z.-H.; Li, P.-X.; Yun, J.-P.; Zhang, R.-X.; et al. A scoring system based on artificial neural network for predicting 10-year survival in stage II A colon cancer patients after radical surgery. Oncotarget 2016, 7, 22939–22947. [Google Scholar] [CrossRef] [Green Version]
- Hassan, C.; Spadaccini, M.; Iannone, A.; Maselli, R.; Jovani, M.; Chandrasekar, V.T.; Antoneli, G.; Yu, H.; Areia, M.; Dinis-Ribeiro, M.; et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: A systematic review and meta-analysis. Gastrointest Endosc. 2021, 93, 77–85.e6. [Google Scholar] [CrossRef]
- Bibault, J.E.; Giraud, P.; Housset, M.; Durdux, C.; Taieb, J.; Berger, A.; Coriat, R.; Chaussade, S.; Dousset, B.; Nordlinger, B.; et al. Deep Learning and Radiomics predict complete response after neo-adjuvant chemoradiation for locally advanced rectal cancer. Sci. Rep. 2018, 8, 12611. [Google Scholar] [CrossRef]
- Lee, J.; An, J.Y.; Choi, M.G.; Park, S.H.; Kim, S.T.; Lee, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S.; Lee, H.; et al. Deep Learning–Based Survival Analysis Identified Associations Between Molecular Subtype and Optimal Adjuvant Treatment of Patients with Gastric Cancer. JCO Clin. Cancer Inform. 2018, 2, 1–14. [Google Scholar] [CrossRef]
- Pan, G.; Yan, G.; Qiu, X.; Cui, J. Bleeding detection in Wireless Capsule Endoscopy based on Probabilistic Neural Network. J. Med. Syst. 2011, 35, 1477–1484. [Google Scholar] [CrossRef]
- Lv, G.; Yan, G.; Wang, Z. Bleeding detection in wireless capsule endoscopy images based on color invariants and spatial pyramids using support vector machines. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2011, 2011, 6643–6646. [Google Scholar]
- Fu, Y.; Zhang, W.; Mandal, M.; Meng, M.Q. Computer-aided bleeding detection in WCE video. IEEE J. Biomed. Health Inform. 2014, 18, 636–642. [Google Scholar] [CrossRef]
- Ghosh, T.; Fattah, S.A.; Shahnaz, C.; Wahid, K.A. An automatic bleeding detection scheme in wireless capsule endoscopy based on histogram of an RGB-indexed image. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2014, 2014, 4683–4686. [Google Scholar]
- Sainju, S.; Bui, F.M.; Wahid, K.A. Automated bleeding detection in capsule endoscopy videos using statistical features and region growing. J. Med. Syst. 2014, 38, 25. [Google Scholar] [CrossRef]
- Hassan, A.R.; Haque, M.A. Computer-aided gastrointestinal hemorrhage detection in wireless capsule endoscopy videos. Comput. Methods Programs Biomed. 2015, 122, 341–353. [Google Scholar] [CrossRef]
- Jia, X.; Meng, M.Q. A deep convolutional neural network for bleeding detection in Wireless Capsule Endoscopy images. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2016, 2016, 639–642. [Google Scholar]
- Usman, M.A.; Satrya, G.B.; Usman, M.R.; Shin, S.Y. Detection of small colon bleeding in wireless capsule endoscopy videos. Comput. Med. Imaging Graph. 2016, 54, 16–26. [Google Scholar] [CrossRef]
- Liu, D.Y.; Gan, T.; Rao, N.N.; Xing, Y.W.; Zheng, J.; Li, S.; Luo, C.-S.; Zhou, Z.-J.; Wan, Y.-L. Identification of lesion images from gastrointestinal endoscope based on feature extraction of combinational methods with and without learning process. Med. Image Anal. 2016, 32, 281–294. [Google Scholar] [CrossRef]
- Leenhardt, R.; Vasseur, P.; Li, C.; Saurin, J.C.; Rahmi, G.; Cholet, F.; Becq, A.; Marteau, P.; Histace, A.; Dray, X.; et al. A neural network algorithm for detection of GI angiectasia during small-bowel capsule endoscopy. Gastrointest. Endosc. 2019, 89, 189–194. [Google Scholar] [CrossRef]
- Ang, T.L.; Kwek, A.B.E.; Wang, L.M. Diagnostic Endoscopic Ultrasound: Technique, Current Status and Future Directions. Gut Liver 2018, 12, 483–496. [Google Scholar] [CrossRef] [Green Version]
- Harmsen, F.R.; Domagk, D.; Dietrich, C.F.; Hocke, M. Discriminating chronic pancreatitis from pancreatic cancer: Contrast-enhanced EUS and multidetector computed tomography in direct comparison. Endosc. Ultrasound 2018, 7, 395–403. [Google Scholar] [CrossRef]
- Shahidi, N.; Ou, G.; Lam, E.; Enns, R.; Telford, J. When trainees reach competency in performing endoscopic ultrasound: A systematic review. Endosc. Int. Open 2017, 5, E239–E243. [Google Scholar] [CrossRef] [Green Version]
- Kuwahara, T.; Hara, K.; Mizuno, N.; Okuno, N.; Matsumoto, S.; Obata, M.; Kurita, Y.; Koda, H.; Toriyama, K.; Onishi, S.; et al. Usefulness of Deep Learning Analysis for the Diagnosis of Malignancy in Intraductal Papillary Mucinous Neoplasms of the Pancreas. Clin. Transl. Gastroenterol. 2019, 10, 1–8. [Google Scholar] [CrossRef]
- Zhang, M.M.; Yang, H.; Jin, Z.D.; Yu, J.G.; Cai, Z.Y.; Li, Z.S. Differential diagnosis of pancreatic cancer from normal tissue with digital imaging processing and pattern recognition based on a support vector machine of EUS images. Gastrointest. Endosc. 2010, 72, 978–985. [Google Scholar] [CrossRef]
- Ozkan, M.; Cakiroglu, M.; Kocaman, O.; Kurt, M.; Yilmaz, B.; Can, G.; Korkmaz, U.; Dandil, E.; Eksi, Z. Age-based computer-aided diagnosis approach for pancreatic cancer on endoscopic ultrasound images. Endosc. Ultrasound 2016, 5, 101–107. [Google Scholar]
- Goyal, H.; Sherazi, S.A.A.; Gupta, S.; Perisetti, A.; Achebe, I.; Ali, A.; Tharian, B.; Thosani, N.; Sharma, N.R. Application of artificial intelligence in diagnosis of pancreatic malignancies by endoscopic ultrasound: A systemic review. Therap. Adv. Gastroenterol. 2022, 15, 17562848221093873. [Google Scholar] [CrossRef]
- Miura, F.; Takada, T.; Amano, H.; Yoshida, M.; Furui, S.; Takeshita, K. Diagnosis of pancreatic cancer. HPB (Oxf.) 2006, 8, 337–342. [Google Scholar] [CrossRef] [Green Version]
- Wolske, K.M.; Ponnatapura, J.; Kolokythas, O.; Burke, L.M.B.; Tappouni, R.; Lalwani, N. Chronic Pancreatitis or Pancreatic Tumor? A Problem-solving Approach. Radiographics 2019, 39, 1965–1982. [Google Scholar] [CrossRef]
- Das, A.; Nguyen, C.C.; Li, F.; Li, B. Digital image analysis of EUS images accurately differentiates pancreatic cancer from chronic pancreatitis and normal tissue. Gastrointest. Endosc. 2008, 67, 861–867. [Google Scholar] [CrossRef]
- Norton, I.D.; Zheng, Y.; Wiersema, M.S.; Greenleaf, J.; Clain, J.E.; Dimagno, E.P. Neural network analysis of EUS images to differentiate between pancreatic malignancy and pancreatitis. Gastrointest. Endosc. 2001, 54, 625–629. [Google Scholar] [CrossRef]
- Săftoiu, A.; Vilmann, P.; Gorunescu, F.; Gheonea, D.I.; Gorunescu, M.; Ciurea, T.; Popescu, G.L.; Iordache, A.; Hassan, H.; Iordache, S. Neural network analysis of dynamic sequences of EUS elastography used for the differential diagnosis of chronic pancreatitis and pancreatic cancer. Gastrointest. Endosc. 2008, 68, 1086–1094. [Google Scholar] [CrossRef]
- Tonozuka, R.; Itoi, T.; Nagata, N.; Kojima, H.; Sofuni, A.; Tsuchiya, T.; Ishii, K.; Tanaka, R.; Nagakawa, Y.; Mukai, S. Deep learning analysis for the detection of pancreatic cancer on endosonographic images: A pilot study. J. Hepatobiliary Pancreat. Sci. 2021, 28, 95–104. [Google Scholar] [CrossRef]
- Zhu, M.; Xu, C.; Yu, J.; Wu, Y.; Li, C.; Zhang, M.; Jin, Z.; Li, Z. Differentiation of pancreatic cancer and chronic pancreatitis using computer-aided diagnosis of endoscopic ultrasound (EUS) images: A diagnostic test. PLoS ONE 2013, 8, e63820. [Google Scholar] [CrossRef] [Green Version]
- Săftoiu, A.; Vilmann, P.; Gorunescu, F.; Janssen, J.; Hocke, M.; Larsen, M.; Iglesias–Garcia, J.; Arcidiacono, P.; Will, U.; Giovannini, M.; et al. Efficacy of an artificial neural network-based approach to endoscopic ultrasound elastography in diagnosis of focal pancreatic masses. Clin. Gastroenterol. Hepatol. 2012, 10, 84–90.e1. [Google Scholar] [CrossRef]
- Săftoiu, A.; Vilmann, P.; Dietrich, C.F.; Iglesias-Garcia, J.; Hocke, M.; Seicean, A.; Ignee, A.; Hassan, H.; Streba, C.T.; Ioncică, A.M.; et al. Quantitative contrast-enhanced harmonic EUS in differential diagnosis of focal pancreatic masses (with videos). Gastrointest. Endosc. 2015, 82, 59–69. [Google Scholar] [CrossRef]
- Yoshida, K.; Toki, F.; Takeuchi, T.; Watanabe, S.; Shiratori, K.; Hayashi, N. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig. Dis. Sci. 1995, 40, 1561–1568. [Google Scholar] [CrossRef]
- Sureka, B.; Rastogi, A. Autoimmune Pancreatitis. Pol. J. Radiol. 2017, 82, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Marya, N.B.; Powers, P.D.; Chari, S.T.; Gleeson, F.C.; Leggett, C.L.; Abu Dayyeh, B.K.; Chandrasekhara, V.; Iyer, P.G.; Majumder, S.; Pearson, R.K.; et al. Utilisation of artificial intelligence for the development of an EUS-convolutional neural network model trained to enhance the diagnosis of autoimmune pancreatitis. Gut 2021, 70, 1335. [Google Scholar] [CrossRef] [PubMed]
- Mendoza Ladd, A.; Diehl, D.L. Artificial intelligence for early detection of pancreatic adenocarcinoma: The future is promising. World J. Gastroenterol. 2021, 27, 1283–1295. [Google Scholar] [CrossRef]
- Norori, N.; Hu, Q.; Aellen, F.M.; Faraci, F.D.; Tzovara, A. Addressing bias in big data and AI for health care: A call for open science. Patterns (N. Y.) 2021, 2, 100347. [Google Scholar] [CrossRef]
- Jayakumar, S.; Sounderajah, V.; Normahani, P.; Harling, L.; Markar, S.R.; Ashrafian, H.; Darzi, A. Quality assessment standards in artificial intelligence diagnostic accuracy systematic reviews: A meta-research study. NPJ Digit. Med. 2022, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Price, W.N. Big data and black-box medical algorithms. Sci. Transl. Med. 2018, 10, eaao5333. [Google Scholar] [CrossRef]
- Taub, S.; Pianykh, O.S. An alternative to the black box: Strategy learning. PLoS ONE 2022, 17, e0264485. [Google Scholar] [CrossRef]
- Gerke, S.; Minssen, T.; Cohen, G. Ethical and Legal Challenges of Artificial Intelligence-Driven Healthcare. In Artificial Intelligence in Healthcare; Elsevier Inc.: Amsterdam, The Netherlands, 2020; pp. 295–336. [Google Scholar]
- Huang, B.; Huang, H.; Zhang, S.; Zhang, D.; Shi, Q.; Liu, J.; Guo, J. Artificial intelligence in pancreatic cancer. Theranostics 2022, 12, 6931–6954. [Google Scholar] [CrossRef]
- Henry, N.L.; Hayes, D.F. Cancer biomarkers. Mol. Oncol. 2012, 6, 140–146. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Artificial Intelligence Model | Patient Population | Outcomes for the Artificial Intelligence Model |
|---|---|---|---|---|
| Kuwahara et al. [47] | Retrospective (Japan) | Deep Learning (Convolutional Neural Networks (CNNs)) | Total IPMN Patients = 50 Benign IPMN Patients = 27 Malignant IPMN Patients = 23 | Recognition of Malignant IPMN: Sensitivity = 95.7% Specificity = 92.6% Accuracy = 94% |
| Zhang et al. [48] | Retrospective (China) | Support Vector Machine (SVM) | Total Patients = 216 Pancreatic Cancer Patients = 153 Non-Cancer Patients = 63 | Recognition of Pancreatic Cancer: Sensitivity = 94.32% Specificity = 99.45% Accuracy = 97.98% |
| Ozkan et al. [49] | Retrospective (Turkey) | Artificial Neuronal Networks (ANNs) | Total Patients = 332 Pancreatic Cancer Patients = 202 Non-Cancer Patients = 130 | Recognition of Pancreatic Cancer (All Ages): Sensitivity = 83.3% Specificity = 93.33% Accuracy = 87.5% Recognition of Pancreatic Cancer (>60 years): Sensitivity = 93.3% Specificity = 88.88% Accuracy = 91.66% Recognition of Pancreatic Cancer (40–60 years): Sensitivity = 85.7% Specificity = 91.66% Accuracy = 88.46% Recognition of Pancreatic Cancer (<40 years): Sensitivity = 87.5% Specificity = 94.11% Accuracy = 92% |
| Goyal et al. [50] | Systematic Review | Artificial Neural Network (ANN) Convolutional Neural Networks (CNNs) Support Vector Machine (SVM) | Total Patients = 2292 Pancreatic Cancer Patients = 1409 Non-Cancer Patients = 883 | Recognition of Pancreatic Cancer: Sensitivity = 83–100% Specificity = 50–99%, Accuracy = 80–97.5% |
| Study | Study Design | Artificial Intelligence Model | Patient Population | Outcomes for the Artificial Intelligence Model |
|---|---|---|---|---|
| Das et al. [53] | Retrospective (United States) | Artificial Neural Network (ANN) | Normal Pancreas Patients = 22 Chronic Pancreatitis Patients = 12 Pancreatic Cancer Patients = 22 | Recognition of Pancreatic Cancer: Sensitivity = 93% Specificity = 92% Recognition of Chronic Pancreatitis versus Normal Pancreas: Sensitivity = 100% Specificity = 100% |
| Norton et al. [54] | Retrospective (United States) | Artificial Neural Network (ANN) | Total Patients = 35 Pancreatic Cancer Patients = 21 Focal Pancreatitis Patients = 14 | Recognition of Pancreatic Cancer by AI: Sensitivity = 100% Specificity = 50% Accuracy = 80% Recognition of Pancreatic Cancer by EUS: Sensitivity = 89% Specificity = 79% Accuracy = 85% Recognition of Pancreatic Cancer by Human Interpretation: Sensitivity = 73% Specificity = 100% Accuracy = 83% |
| Săftoiu et al. [55] | Retrospective (Europe) | Artificial Neural Network (ANN) | Total Patients = 68 Pancreatic Cancer Patients = 32 Pancreatic Neuroendocrine Tumor Patients = 3 Chronic Pancreatitis Patients = 11 Normal Pancreas Patients = 22 | Recognition of Pancreatic Cancer and Pancreatic Neuroendocrine Tumors: Sensitivity = 91.4% Specificity = 87.9% Accuracy = 89.7% |
| Tonozuka et al. [56] | Cross-Sectional (Japan) | Convolutional Neural Networks (CNNs) | Total Patients = 139 Pancreatic Cancer Patients = 76 Chronic Pancreatitis Patients = 34 Normal Pancreas Patients = 29 | Recognition of Pancreatic Cancer (Validation Set): Sensitivity = 90.2% Specificity = 74.9% Area Under the Curve = 0.924 Recognition of Pancreatic Cancer (Test Set): Sensitivity = 92.4% Specificity = 84.1% Area Under the Curve = 0.940 |
| Zhu et al. [57] | Retrospective (China) | Support Vector Machine (SVM) | Total Patients = 388 Pancreatic Cancer Patients = 262 Chronic Pancreatitis Patients = 126 | Recognition of Pancreatic Cancer: Sensitivity = 96.25% Specificity = 93.38% Accuracy = 94.2% |
| Săftoiu et al. [58] | Prospective Multicenter (Europe) | Artificial Neural Network (ANN) | Total Patients = 258 Pancreatic Cancer Patients = 211 Chronic Pancreatitis Patients = 47 | Recognition of Pancreatic Cancer: Sensitivity = 87.59% Specificity = 82.94% Area Under the Curve = 0.94 |
| Săftoiu et al. [59] | Prospective Multicenter Observational (Europe) | Artificial Neural Network (ANN) | Total Patients = 167 Pancreatic Cancer Patients = 112 Chronic Pancreatitis Patients = 55 | Recognition of Pancreatic Cancer by AI: Sensitivity = 94.64% Specificity = 94.44% Recognition of Pancreatic Cancer by Contrast-Enhanced EUS: Sensitivity = 87.5% Specificity = 92.72% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dahiya, D.S.; Al-Haddad, M.; Chandan, S.; Gangwani, M.K.; Aziz, M.; Mohan, B.P.; Ramai, D.; Canakis, A.; Bapaye, J.; Sharma, N. Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer: Where Are We Now and What Does the Future Entail? J. Clin. Med. 2022, 11, 7476. https://doi.org/10.3390/jcm11247476
Dahiya DS, Al-Haddad M, Chandan S, Gangwani MK, Aziz M, Mohan BP, Ramai D, Canakis A, Bapaye J, Sharma N. Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer: Where Are We Now and What Does the Future Entail? Journal of Clinical Medicine. 2022; 11(24):7476. https://doi.org/10.3390/jcm11247476
Chicago/Turabian StyleDahiya, Dushyant Singh, Mohammad Al-Haddad, Saurabh Chandan, Manesh Kumar Gangwani, Muhammad Aziz, Babu P. Mohan, Daryl Ramai, Andrew Canakis, Jay Bapaye, and Neil Sharma. 2022. "Artificial Intelligence in Endoscopic Ultrasound for Pancreatic Cancer: Where Are We Now and What Does the Future Entail?" Journal of Clinical Medicine 11, no. 24: 7476. https://doi.org/10.3390/jcm11247476