
Effects of Cardiac Contractility Modulation Electrodes on Tricuspid Regurgitation in Patients with Heart Failure with Reduced Ejection Fraction: A Pilot Study
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
- −
- Left ventricular ejection fraction of <40%;
- −
- New York Heart Association (NYHA) class II–III;
- −
- Referral for CCM implant due to the >2 unplanned visits or hospitalization in the last 12 months and/or the persistence of HF-related symptoms despite the use of optimal medical therapy;
- −
- A QRS duration of <120 msec.
- −
- Acute coronary syndrome in the previous three months;
- −
- ICD implantation in the previous twelve months;
- −
- Severe tricuspid regurgitation (i.e., vena contracta >7 mm, proximal isosurface radius >9 mm).
2.2. Echocardiographic Evaluation
2.3. Optimizer Smart® Implant
2.4. Statistical Analysis
3. Results
4. Discussion
- (1)
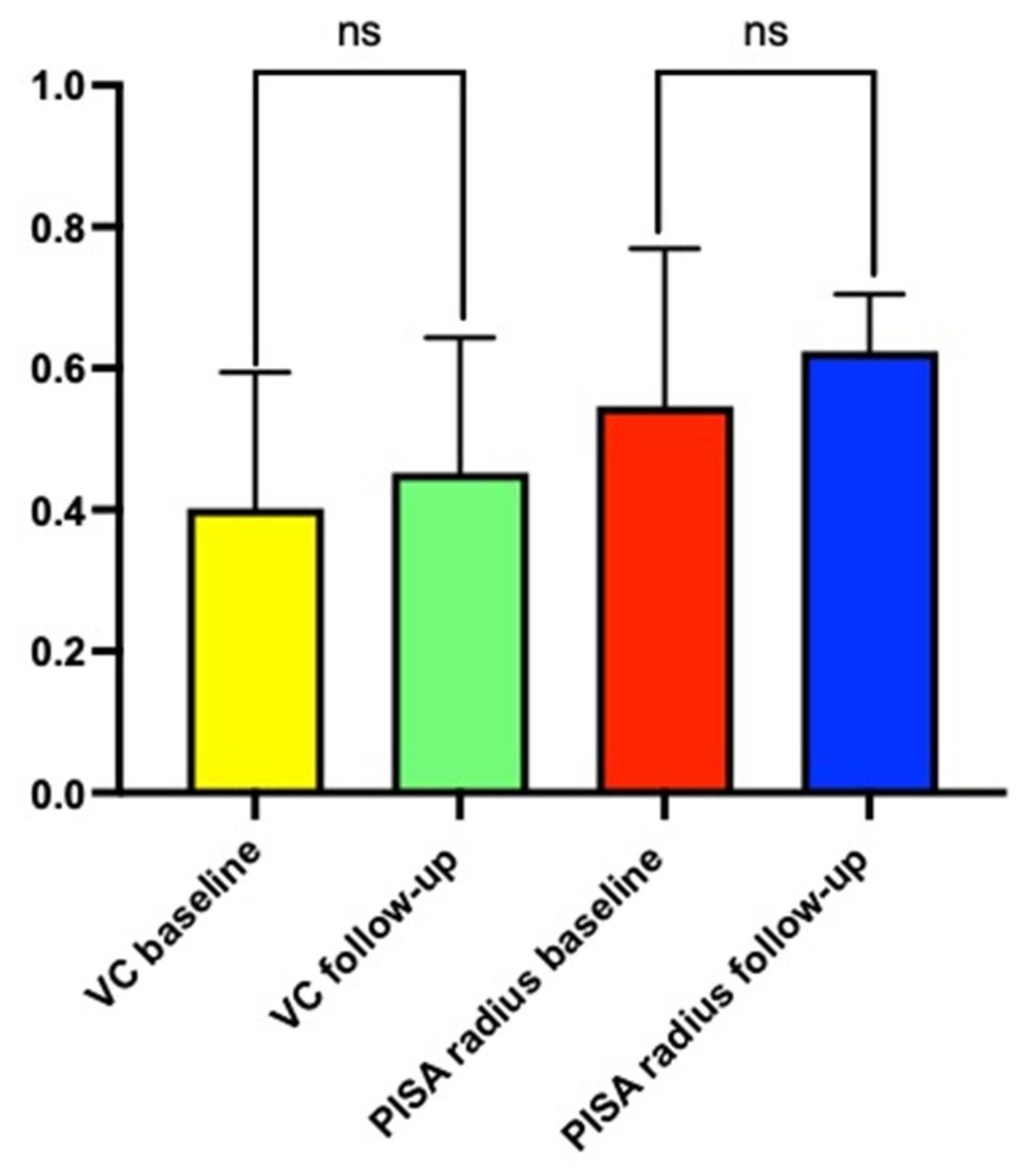
- The implantation of pacemaker leads to deliver CCM therapy did not result in a worsening of TR at six months compared with the baseline.
- (2)
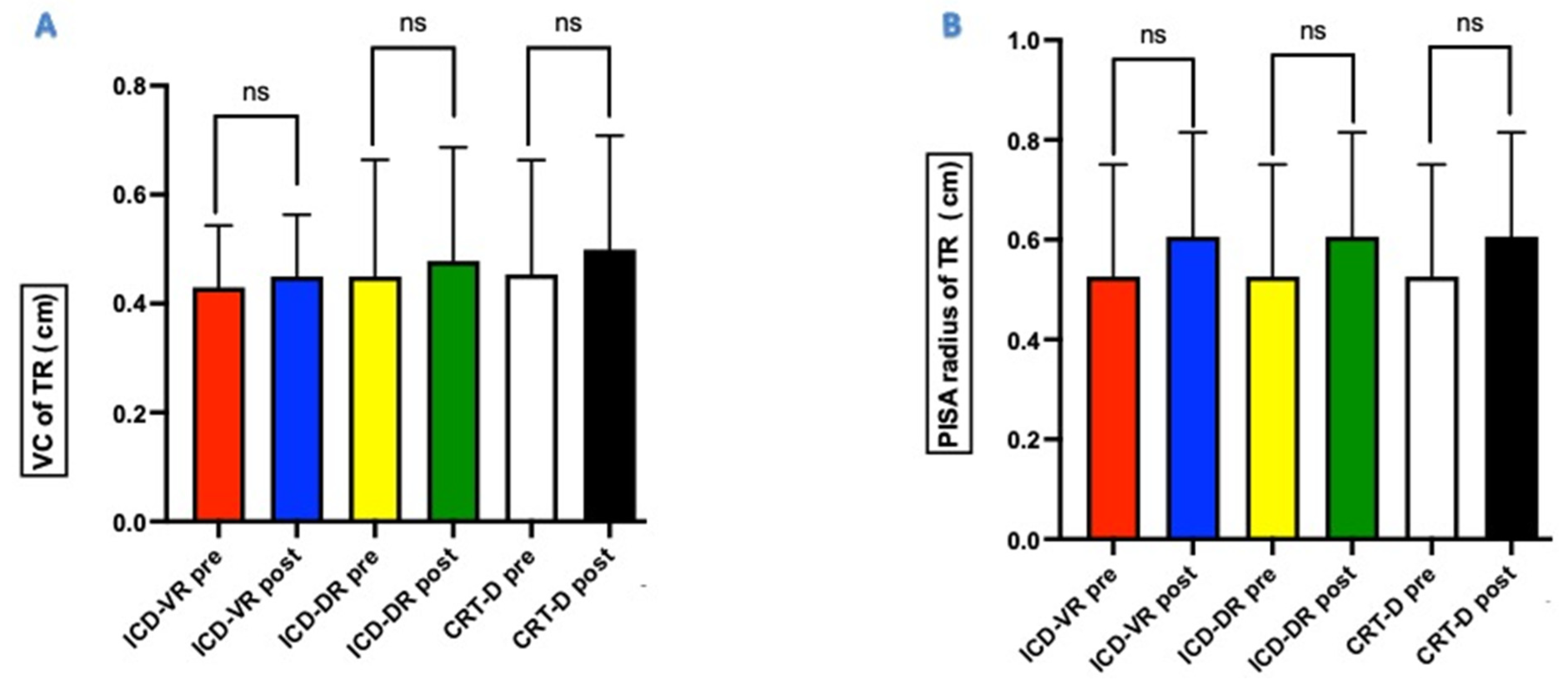
- The absence of TR worsening was independent of the type of CIED previously implanted and, therefore, the presence and number of endocardial leads already implanted.
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, P.A.; Nadarajah, R.; Ali, N.; Gierula, J.; Witte, K.K. Cardiac contractility modulation for the treatment of heart failure with reduced ejection fraction. Heart Fail Rev. 2021, 26, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Rao, I.V.; Burkhoff, D. Cardiac contractility modulation for treating moderate to severe HF. Expert Rev. Med. Devices 2021, 18, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kuschyk, J.; Falk, P.; Demming, T.; Marx, O.; Morley, D.; Rao, I.; Burkhoff, D. Long-term clinical experience with cardiac contractility modulation therapy delivered by the Optimizer Smart system. Eur. J. Heart Fail. 2021, 23, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Lindenfeld, J.; Reddy, V.Y.; Hasenfuss, G.; Kuck, K.H.; Boscardin, J.; Gibbons, R.; Burkhoff, D. FIX-HF-5C Investigators and Coordinators. A randomized controlled trial to evaluate the safety and efficacy of cardiac contractility modulation in patients with moderately reduced left ventricular ejection fraction and a narrow QRS duration: Study rationale and design. J. Card Fail. 2015, 21, 16–23. [Google Scholar]
- Cantillon, D.J.; Exner, D.V.; Badie, N.; Davis, K.; Gu, N.Y.; Nabutovsky, Y.; Doshi, R. Complications and Health Care Costs Associated With Transvenous Cardiac Pacemakers in a Nationwide Assessment. JACC Clin. Electrophysiol. 2017, 3, 1296–1305. [Google Scholar] [CrossRef]
- Chang, J.D.; Manning, W.J.; Ebrille, E.; Zimetbaum, P.J. Tricuspid Valve Dysfunction Following Pacemaker or Cardioverter-Defibrillator Implantation. J. Am. Coll. Cardiol. 2017, 69, 2331–2341. [Google Scholar] [CrossRef]
- Trankle, C.R.; Gertz, Z.M.; Koneru, J.N.; Kasirajan, V.; Nicolato, P.; Bhardwaj, H.L.; Ellenbogen, K.A.; Kalahasty, G. Severe tricuspid regurgitation due to interaction with right ventricular permanent pacemaker or defibrillator leads. Pacing Clin. Electrophysiol. 2018, 41, 845–853. [Google Scholar] [CrossRef]
- Ebrille, E.; Chang, J.D.; Zimetbaum, P.J. Tricuspid Valve Dysfunction Caused by Right Ventricular Leads. Card. Electrophysiol. Clin. 2018, 10, 447–452. [Google Scholar] [CrossRef]
- Van De Heyning, C.M.; Elbarasi, E.; Masiero, S.; Brambatti, M.; Ghazal, S.; Al-Maashani, S.; Capucci, A.; Leong, D.; Shivalkar, B.; Saenen, J.B.; et al. Prospective Study of Tricuspid Regurgitation Associated With Permanent Leads After Cardiac Rhythm Device Implantation. Can. J. Cardiol. 2019, 35, 389–395. [Google Scholar] [CrossRef]
- Abraham, W.T.; Burkhoff, D.; Nademanee, K.; Carson, P.; Bourge, R.; Ellenbogen, K.A.; Parides, M.; Kadish, A. A randomized controlled trial to evaluate the safety and efficacy of cardiac contractility modulation in patients with systolic heart failure: Rationale, design, and baseline patient characteristics. Am. Heart J. 2008, 156, 641–648. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef]
- Quiñones, M.A.; Otto, C.M.; Stoddard, M.; Waggoner, A.; Zoghbi, W.A. Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. Recommendations for quantification of Doppler echocardiography: A report from the Doppler Quantification Task Force of the Nomenclature and Standards Committee of the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2002, 1, 167–184. [Google Scholar]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Non invasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Addetia, K.; Harb, S.C.; Hahn, R.T.; Kapadia, S.; Lang, R.M. Cardiac Implantable Electronic Device Lead-Induced Tricuspid Regurgitation. JACC Cardiovasc. Imaging 2019, 12, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.X.; Wei, M.; Xiang, R.; Lu, Y.M.; Zhang, L.; Li, Y.D.; Zhang, J.H.; Xing, Q.; Tang, B.P.; Zhou, X.H. Incidence, Risk Factors, and Prognosis of Tricuspid Regurgitation After Cardiac Implantable Electronic Device Implantation: A Systematic Review and Meta-analysis. J. Cardiothorac. Vasc. Anesth. 2021, 25, 1741–1755. [Google Scholar] [CrossRef]
- Al-Mohaissen, M.A.; Chan, K.L. Prevalence and mechanism of tricuspid regurgitation following implantation of endocardial leads for pacemaker or cardioverter-defibrillator. J. Am. Soc. Echocardiogr. 2012, 25, 245–252. [Google Scholar] [CrossRef]
- Alizadeh, A.; Sanati, H.R.; Haji-Karimi, M.; Yazdi, A.H.; Rad, M.A.; Haghjoo, M.; Emkanjoo, Z. Induction and aggravation of atrioventricular valve regurgitation in the course of chronic right ventricular apical pacing. Europace 2011, 13, 1587–1590. [Google Scholar] [CrossRef]
- Yücel, G.; Fastner, C.; Hetjens, S.; Toepel, M.; Schmiel, G.; Yazdani, B.; Husain-Syed, F.; Liebe, V.; Rudic, B.; Akin, I.; et al. Impact of baseline left ventricular ejection fraction on long-term outcomes in cardiac contractility modulation therapy. Pacing Clin. Electrophysiol. 2022, 45, 639–648. [Google Scholar] [CrossRef]
- Dreyfus, G.D.; Martin, R.P.; Chan, K.M.; Dulguerov, F.; Alexandrescu, C. Functional tricuspid regurgitation: A need to revise our understanding. J. Am. Coll. Cardiol. 2015, 65, 2331–2336. [Google Scholar] [CrossRef] [Green Version]
- Margonato, D.; Ancona, F.; Ingallina, G.; Melillo, F.; Stella, S.; Biondi, F.; Boccellino, A.; Godino, C.; Margonato, A. Tricuspid Regurgitation in Left Ventricular Systolic Dysfunction: Marker or Target? Front. Cardiovasc. Med. 2021, 8, 702589. [Google Scholar] [CrossRef]
- Contaldi, C.; De Vivo, S.; Martucci, M.L.; D’Onofrio, A.; Ammendola, E.; Nigro, G.; Errigo, V.; Pacileo, G.; Masarone, D. Effects of Cardiac Contractility Modulation Therapy on Right Ventricular Function: An Echocardiographic Study. Appl. Sci. 2022, 12, 7917–7923. [Google Scholar] [CrossRef]
- Fukuda, S.; Gillinov, A.M.; Song, J.M.; Daimon, M.; Kongsaerepong, V.; Thomas, J.D.; Shiota, T. Echocardiographic insights into atrial and ventricular mechanisms of functional tricuspid regurgitation. Am. Heart J. 2006, 152, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Kim, Y.J.; Park, J.S.; Kim, K.H.; Kim, K.B.; Ahn, H.; Sohn, D.W.; Oh, B.H.; Park, Y.B.; Choi, Y.S. Determinants of the severity of functional tricuspid regurgitation. Am. J. Cardiol 2006, 98, 236–242. [Google Scholar] [CrossRef]
- Lin, G.; Nishimura, R.A.; Connolly, H.M.; Dearani, J.A.; Sundt, T.M., 3rd; Hayes, D.L. Severe symptomatic tricuspid valve regurgitation due to permanent pacemaker or implantable cardioverter-defibrillator leads. J. Am. Coll. Cardiol. 2005, 45, 1672–1675. [Google Scholar] [CrossRef] [Green Version]
- Vinciguerra, M.; Sitges, M.; Luis Pomar, J.; Romiti, S.; Domenech-Ximenos, B.; D’Abramo, M.; Wretschko, E.; Miraldi, F.; Greco, E. Functional Tricuspid Regurgitation: Behind the Scenes of a Long-Time Neglected Disease. Front. Cardiovasc. Med. 2022, 9, 836441. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total Population (n = 30) |
|---|---|
| Age (mean ± SD) | 59.5 ± 12.9 years |
| Female sex (n, %) | 5 (16.6%) |
| Ischemic etiology (n, %) | 13 (43.3%) |
| Hypertension (n, %) | 10 (33.3%) |
| Diabetes (n, %) | 8 (26.6%) |
| NYHA class II (n, %) | 6 (20%) |
| NYHA class III (n, %) | 24 (80%) |
| SBP (mean ± SD) | 108 ± 12.3 mmHg |
| DBP (mean ± SD) | 62 ± 5.7 mmHg |
| HR (mean ± SD) | 62 ± 10.2 b/m |
| NT-pro-BNP (mean ± SD) | 3956 ± 2872 pg/mL |
| Atrial fibrillation | 12 (40%) |
| ICD-DR | 14 (46.6%) |
| ICD-VR | 2 (6.6%) |
| S-ICD | 2 (6.6%) |
| CRT-D | 12 (40%) |
| Hb (mean ± SD) | 11.3 ± 1.2 g/dL |
| Creatinine (mean ± SD) | 1.2 ± 0.7 mg/d: |
| e-GFR (mean ± SD) | 45.9 ± 13.6 mL/min/1.73 m² |
| LVEDV (mean ± SD) | 225.8 ± 51.6 mL |
| LVESV (mean ± SD) | 162.4 ± 41.8 mL |
| LVEF (mean ± SD) | 30.5 ± 3.6% |
| E wave (mean ± SD) | 110.5 ± 38.7 cm/sec |
| E’ average (mean ± SD) | 5.8 ± 3.2 cm/sec |
| E/e’ average (mean ± SD) | 15.5 ± 4.2 |
| DecT (mean ± SD) | 142.8 ± 45.3 m/sec |
| LAVi (mean ± SD) | 47.3 ± 11.5 mL/m2 |
| RVOT prox (mean ± SD) | 28.7 ± 4.2 mm |
| RVOT dist (mean ± SD) | 25.3 ± 3.8 mm |
| RVD 1 (mean ± SD) | 29.2 ± 4.8 mm |
| RVD 2 (mean ± SD) | 27.5 ± 5.2 mm |
| RVD3 (mean ± SD) | 63.4 ± 6.2 mm |
| TAPSE (mean ± SD) | 13.6 ± 5.6 mm |
| S wave (mean ± SD) | 10.3 ± 1.5 cm/sec |
| PASP (mean ± SD) | 37.6 ± 8.2 mmHg |
| TR mild (n, %) | 17 (56.6%) |
| TR moderate (n, %) | 13 (43.4%) |
| Parameter | Baseline | 6-Month Follow-Up | p-Value |
|---|---|---|---|
| RVOT prox (mean ± SD) | 28.7 ± 4.2 mm | 26.3 ± 3.8 | 0.042 |
| RVOT dist (mean ± SD) | 25.3 ± 3.8 mm | 22.9 ± 4.5 mm | 0.037 |
| RVD 1 (mean ± SD) | 29.2 ± 4.8 mm | 27.2 ± 3.3 mm | 0.026 |
| RVD 2 (mean ± SD) | 27.5 ± 5.2 mm | 26.2 ± 4.8 mm | 0.022 |
| RVD3 (mean ± SD) | 63.4 ± 6.2 mm | 61.9 ± 3.8 mm | 0.031 |
| TAPSE (mean ± SD) | 13.6 ± 5.6 mm | 16.7 ± 4.6 mm | 0.012 |
| S wave (mean ± SD) | 10.3 ± 1.5 cm/s | 12.3 ± 2.8 cm/s | 0.017 |
| PASP (mean ± SD) | 37.6 ± 8.2 mmHg | 33.6 ± 4.7 mmHg | 0.035 |
| PAMP | 20.3 ± 7.5 mmHg | 15.8 ± 4.2 mmHg | 0.043 |
| PCWP | 12.6 ± 5.8 mmHg | 9.3 ± 2.9 mmHg | 0.031 |
| Variable | Mean + SD | Β | t | p-Value |
|---|---|---|---|---|
| Δ TR degree at six months | 2.5 ± 0.03 | - | - | - |
| Age (years) | 59.5 ± 12.9 | −0984 | 0.756 | 0.082 |
| SBP (mmHg) | 108 ± 12.3 | −0.063 | 0.250 | 0.767 |
| HR (b/m) | 62 ± 10.2 | −0.265 | 0.371 | 0.428 |
| LVEF (%) | 30.5 ± 3.6% | 0.189 | 0.465 | 0.021 |
| PCWP (mmHg) | 12.6 ± 5.8 | −0543 | 0.751 | 0.065 |
| PASP (mmHg) | 37.6 ± 8.2 | −0345 | 0.651 | 0.048 |
| TAPSE (mm) | 13.6 ± 5.6 | −0012 | 0.345 | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masarone, D.; Kittleson, M.M.; De Vivo, S.; D’Onofrio, A.; Rao, I.; Ammendola, E.; Errigo, V.; Martucci, M.L.; Nigro, G.; Pacileo, G. Effects of Cardiac Contractility Modulation Electrodes on Tricuspid Regurgitation in Patients with Heart Failure with Reduced Ejection Fraction: A Pilot Study. J. Clin. Med. 2022, 11, 7442. https://doi.org/10.3390/jcm11247442
Masarone D, Kittleson MM, De Vivo S, D’Onofrio A, Rao I, Ammendola E, Errigo V, Martucci ML, Nigro G, Pacileo G. Effects of Cardiac Contractility Modulation Electrodes on Tricuspid Regurgitation in Patients with Heart Failure with Reduced Ejection Fraction: A Pilot Study. Journal of Clinical Medicine. 2022; 11(24):7442. https://doi.org/10.3390/jcm11247442
Chicago/Turabian StyleMasarone, Daniele, Michelle M. Kittleson, Stefano De Vivo, Antonio D’Onofrio, Ishu Rao, Ernesto Ammendola, Vittoria Errigo, Maria L. Martucci, Gerardo Nigro, and Giuseppe Pacileo. 2022. "Effects of Cardiac Contractility Modulation Electrodes on Tricuspid Regurgitation in Patients with Heart Failure with Reduced Ejection Fraction: A Pilot Study" Journal of Clinical Medicine 11, no. 24: 7442. https://doi.org/10.3390/jcm11247442